Imaging & Oncology - Society of Radiographers
Imaging & Oncology - Society of Radiographers
Imaging & Oncology - Society of Radiographers

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
are several areas <strong>of</strong> research potential, including the early detection <strong>of</strong><br />
microvascular dysfunction, (which helps in the early detection <strong>of</strong> CAD) and<br />
the assessment <strong>of</strong> vascular dysfunction in cardiomyopathies 23,24,25 .<br />
Figures 5a and b (opposite page) show globally reduced perfusion in the<br />
left ventricular myocardium unmasked more easily with globally reduced<br />
MBF reserve.<br />
Figure 6a shows significant reversibility and ischaemia in the right<br />
coronary artery territory involving the inferior and lateral walls, however,<br />
the MBF as shown in figure 6b is globally reduced therefore also implying<br />
multivessel disease.<br />
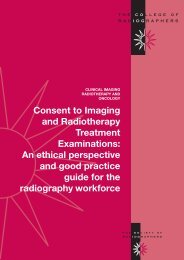
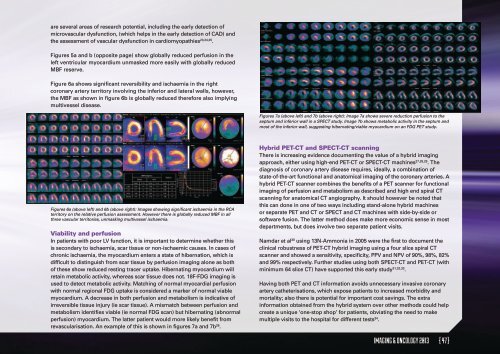
Figures 7a (above left) and 7b (above right): Image 7a shows severe reduction perfusion to the<br />
septum and inferior wall in a SPECT study. Image 7b shows metabolic activity in the septum and<br />
most <strong>of</strong> the inferior wall, suggesting hibernating/viable myocardium on an FDG PET study.<br />
Figures 6a (above left) and 6b (above right): Images showing significant ischaemia in the RCA<br />
territory on the relative perfusion assessment. However there is globally reduced MBF in all<br />
three vascular territories, unmasking multivessel ischaemia.<br />
Viability and perfusion<br />
In patients with poor LV function, it is important to determine whether this<br />
is secondary to ischaemia, scar tissue or non-ischaemic causes. In cases <strong>of</strong><br />
chronic ischaemia, the myocardium enters a state <strong>of</strong> hibernation, which is<br />
difficult to distinguish from scar tissue by perfusion imaging alone as both<br />
<strong>of</strong> these show reduced resting tracer uptake. Hibernating myocardium will<br />
retain metabolic activity, whereas scar tissue does not. 18F-FDG imaging is<br />
used to detect metabolic activity. Matching <strong>of</strong> normal myocardial perfusion<br />
with normal regional FDG uptake is considered a marker <strong>of</strong> normal viable<br />
myocardium. A decrease in both perfusion and metabolism is indicative <strong>of</strong><br />
irreversible tissue injury (ie scar tissue). A mismatch between perfusion and<br />
metabolism identifies viable (ie normal FDG scan) but hibernating (abnormal<br />
perfusion) myocardium. The latter patient would more likely benefit from<br />
revascularisation. An example <strong>of</strong> this is shown in figures 7a and 7b 26 .<br />
Hybrid PET-CT and SPECT-CT scanning<br />
There is increasing evidence documenting the value <strong>of</strong> a hybrid imaging<br />
approach, either using high-end PET-CT or SPECT-CT machines 27,28,29 . The<br />
diagnosis <strong>of</strong> coronary artery disease requires, ideally, a combination <strong>of</strong><br />
state-<strong>of</strong>-the-art functional and anatomical imaging <strong>of</strong> the coronary arteries. A<br />
hybrid PET-CT scanner combines the benefits <strong>of</strong> a PET scanner for functional<br />
imaging <strong>of</strong> perfusion and metabolism as described and high end spiral CT<br />
scanning for anatomical CT angiography. It should however be noted that<br />
this can done in one <strong>of</strong> two ways including stand-alone hybrid machines<br />
or separate PET and CT or SPECT and CT machines with side-by-side or<br />
s<strong>of</strong>tware fusion. The latter method does make more economic sense in most<br />
departments, but does involve two separate patient visits.<br />
Namdar et al 30 using 13N-Ammonia in 2005 were the first to document the<br />
clinical robustness <strong>of</strong> PET-CT hybrid imaging using a four slice spiral CT<br />
scanner and showed a sensitivity, specificity, PPV and NPV <strong>of</strong> 90%, 98%, 82%<br />
and 99% respectively. Further studies using both SPECT-CT and PET-CT (with<br />
minimum 64 slice CT) have supported this early study 31,32,33 .<br />
Having both PET and CT information avoids unnecessary invasive coronary<br />
artery catheterisations, which expose patients to increased morbidity and<br />
mortality; also there is potential for important cost savings. The extra<br />
information obtained from the hybrid system over other methods could help<br />
create a unique ‘one-stop shop’ for patients, obviating the need to make<br />
multiple visits to the hospital for different tests 34 .<br />
IMAGING & ONCOLOGY 2013 { 47 }