here - Great Ormond Street Hospital Laboratory Medicine
here - Great Ormond Street Hospital Laboratory Medicine
here - Great Ormond Street Hospital Laboratory Medicine

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
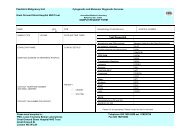
Paediatric Malignancy Unit<br />
<strong>Great</strong> <strong>Ormond</strong> <strong>Street</strong> <strong>Hospital</strong> NHS Trust<br />
Cytogenetic and Molecular Diagnostic Services<br />
SAMPLE REQUEST FORM<br />
NAME<br />
SEX<br />
F M<br />
SAMPLE TYPE VOLUME DATE AND TIME TAKEN<br />
DOB Histopathology ID/Lab Reference HOSPITAL NUMBER<br />
Test Requested<br />
NHS NUMBER<br />
CONSULTANT NAME<br />
CLINICAL DETAILS:<br />
Karyotyping and FISH analysis<br />
for leukemia, lymphoma,<br />
Mutation Detection by Direct Sequencing:<br />
ELA2<br />
multiple myeloma and solid tumours<br />
HAX1<br />
NAME AND ADDRESS OF REFERRING HOSPITAL<br />
FFPE FISH<br />
SMARCB1<br />
GATA1<br />
KRAS<br />
Translocation Detection:<br />
NRAS<br />
Leukemia<br />
PTPN11<br />
Sarcoma<br />
CBL<br />
KIAA1549-BRAF<br />
cKIT<br />
Lymphoma<br />
PDGFRa<br />
TP53<br />
CONTACT TELEPHONE NUMBER<br />
AND EMAIL ADDRESS<br />
PRIORITY:<br />
URGENT/ROUTINE<br />
Other:<br />
B-catenin<br />
BRAF<br />
GNAS<br />
WT1<br />
WTX<br />
IDH1<br />
IDH2<br />
JAK2<br />
FOXF1<br />
CONTACT FAX NUMBER FOR REPORT<br />
PATIENT CONSENT<br />
Has consent been given for:<br />
Testing for this referral reason?<br />
YES/NO<br />
MLPA:<br />
Neuroblastoma kit 251and 252<br />
SMARCB1 Kit 258<br />
Please tick as appropriate. Please contact the lab for new tests.<br />
Pease send samples to: Telephone 020 7405 9200 ext. 5762/5755<br />
PMU, Level 2 Camelia Botnar Laboratories Fax 020 7829 8803<br />
<strong>Great</strong> <strong>Ormond</strong> <strong>Street</strong> <strong>Hospital</strong> NHS Trust<br />
<strong>Great</strong> <strong>Ormond</strong> St<br />
London WC1N 3JH
Paediatric Malignancy Unit<br />
<strong>Great</strong> <strong>Ormond</strong> <strong>Street</strong> <strong>Hospital</strong> NHS Trust<br />
Cytogenetic and Molecular Diagnostic Services<br />
SAMPLE REQUEST FORM<br />
INSTRUCTIONS:<br />
Bone marrow and blood samples for Karyotyping and<br />
FISH analysis:<br />
<br />
<br />
<br />
<br />
Any other sample:<br />
<br />
Please send 5 mls in preservative free<br />
heparin.<br />
Sample must be labelled with patient name,<br />
DOB and hospital number.<br />
Date and time taken must be written on the<br />
sample and request form.<br />
Mix sample well to prevent clotting.<br />
Please phone the lab for advice.<br />
Samples for karyotyping and RT-PCR must reach the<br />
laboratory within 24 hours of being taken. All other<br />
samples can be sent by 1 st class post.<br />
Blood samples for mutation detection<br />
and MLPA analysis:<br />
<br />
<br />
<br />
<br />
Please send 5 mls in EDTA or<br />
preservative free heparin.<br />
Sample must be labelled with<br />
patient name, DOB and hospital<br />
number.<br />
Date and time taken must be<br />
written on the sample and<br />
request form.<br />
Mix sample well to prevent<br />
clotting.<br />
DNA for mutation detection and<br />
MLPA analysis:<br />
<br />
Please send a minimum of 10ug<br />
of DNA to perform mutation<br />
detection.<br />
Please ensure a minimum of 2<br />
unique identifiers on the DNA<br />
tube.<br />
Blood and Bone marrow samples for RT-PCR analysis<br />
<br />
<br />
<br />
5 mls in preservative free heparin.<br />
Sample must be labelled with patient name, DOB and hospital number.<br />
Date and time taken must be written on the sample and request form.<br />
FFPE material for FISH and RT-PCR:<br />
<br />
<br />
<br />
FFPE section on slides should be between 2-4uM thick.<br />
Please send a minimum of 4 slides with a minimum of 2 unique identifiers.<br />
For RNA extraction please send 5-10 rolled sections (5-10 uM thick) in an eppendorf<br />
with a minimum of 2 unique identifiers.<br />
Patient Consent Clarification:<br />
Under the Human Tissue Act 2004 informed patient consent is required for all tests from all<br />
patients, and for storage of RNA, DNA and relevant material from DECEASED patients.<br />
Cell suspensions, slides, RNA and DNA from LIVING patients may be stored without<br />
consent for the following purposes (patients should be made aware of this): Audit,<br />
education and training, performance assessment, quality assurance and anonymised<br />
research.<br />
Pease send samples to: Telephone 020 7405 9200 ext. 5762/5755<br />
PMU, Level 2 Camelia Botnar Laboratories Fax 020 7829 8803<br />
<strong>Great</strong> <strong>Ormond</strong> <strong>Street</strong> <strong>Hospital</strong> NHS Trust<br />
<strong>Great</strong> <strong>Ormond</strong> St<br />
London WC1N 3JH