Joint Annual Research Report 2005 - The Royal Marsden
Joint Annual Research Report 2005 - The Royal Marsden
Joint Annual Research Report 2005 - The Royal Marsden

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
IMAGING RESEARCH & CANCER DIAGNOSIS – MAGNETIC RESONANCE<br />
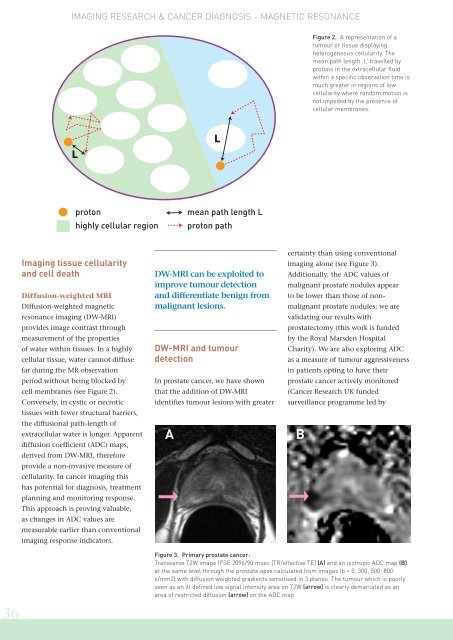
Figure 2. A representation of a<br />
tumour or tissue displaying<br />
heterogeneous cellularity. <strong>The</strong><br />
mean path length ‘L’ travelled by<br />
protons in the extracellular fluid<br />
within a specific observation time is<br />
much greater in regions of low<br />
cellularity where random motion is<br />
not impeded by the presence of<br />
cellular membranes.<br />
L<br />
L<br />
proton<br />
highly cellular region<br />
mean path length L<br />
proton path<br />
Imaging tissue cellularity<br />
and cell death<br />
Diffusion-weighted MRI<br />
Diffusion-weighted magnetic<br />
resonance imaging (DW-MRI)<br />
provides image contrast through<br />
measurement of the properties<br />
of water within tissues. In a highly<br />
cellular tissue, water cannot diffuse<br />
far during the MR observation<br />
period without being blocked by<br />
cell membranes (see Figure 2).<br />
Conversely, in cystic or necrotic<br />
tissues with fewer structural barriers,<br />
the diffusional path-length of<br />
extracellular water is longer. Apparent<br />
diffusion coefficient (ADC) maps,<br />
derived from DW-MRI, therefore<br />
provide a non-invasive measure of<br />
cellularity. In cancer imaging this<br />
has potential for diagnosis, treatment<br />
planning and monitoring response.<br />
This approach is proving valuable,<br />
as changes in ADC values are<br />
measurable earlier than conventional<br />
imaging response indicators.<br />
DW-MRI can be exploited to<br />
improve tumour detection<br />
and differentiate benign from<br />
malignant lesions.<br />
DW-MRI and tumour<br />
detection<br />
In prostate cancer, we have shown<br />
that the addition of DW-MRI<br />
identifies tumour lesions with greater<br />
A<br />
certainty than using conventional<br />
imaging alone (see Figure 3).<br />
Additionally, the ADC values of<br />
malignant prostate nodules appear<br />
to be lower than those of nonmalignant<br />
prostate nodules; we are<br />
validating our results with<br />
prostatectomy (this work is funded<br />
by the <strong>Royal</strong> <strong>Marsden</strong> Hospital<br />
Charity). We are also exploring ADC<br />
as a measure of tumour aggressiveness<br />
in patients opting to have their<br />
prostate cancer actively monitored<br />
(Cancer <strong>Research</strong> UK funded<br />
surveillance programme led by<br />
B<br />
Figure 3. Primary prostate cancer:<br />
Transverse T2W image (FSE 2096/90 msec [TR/effective TE] (A) and an isotropic ADC map (B)<br />
at the same level through the prostate apex calculated from images (b = 0, 300, 500, 800<br />
s/mm2) with diffusion weighted gradients sensitised in 3 planes. <strong>The</strong> tumour which is poorly<br />
seen as an ill defined low signal intensity area on T2W (arrow) is clearly demarcated as an<br />
area of restricted diffusion (arrow) on the ADC map.<br />
36