Alan Thompson - The Royal Marsden
Alan Thompson - The Royal Marsden
Alan Thompson - The Royal Marsden

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Bladder cancer:who, when, where andhowMr <strong>Alan</strong> <strong>Thompson</strong>Head of Urology Unit,Consultant Urologist Surgeon
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Who ?
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>How common is bladder cancer ?• Bladder cancer (BC) is 7 th most common overallcancer in the UK4 th most common in men – 7,300 cases12 th most common in women – 2,800 cases• Approx 10,100 diagnosed with BC in 2007 – 28/day• More than 2 x as many men get BC than women• 80% cases of BC occur over age 65 years
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>How many people survive bladder cancer ?• Bladder cancer survival rates have improved over thelast 30 years or so57% of men - survive > 5 years47% of women - survive > 5 years• Approx half of patients diagnosed are likely to survivefor at least 10 years• Survival rates are higher for patients diagnosed at ayounger age
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>How many people die from bladder cancer ?• Bladder cancer is the eighth most common cause ofcancer death in the UK• Approx 5000 deaths in 2008 – 96/week• Approx 90% deaths are in patients over age 65 years• From a peak in 1990 death rates in men have fallenby 1/3
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Summary – incidence, survival & deaths
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Bladder cancer – main causes/risk factors• Tobacco – main preventable risk2/3 cases in men1/3 cases in women• Smokers have 2 – 6 x increased risk (length & number)• Cessation reduces risk – > 20 years ‘til risk end• Environmental tobacco smoke during childhoodincreases risk of BC by nearly 40%
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Bladder cancer – main causes/risk factors• Age• Family History – 1 st degree esp. if diagnosed under 45• Occupational exposure (5-10% in men in Europe)Polycyclic aromatic hydrocarbons• Hair dyes?• Medicines/irradiation – chemotherapy. Testicular/cervical• Medical Conditions – Schistosomiasis/paraplegics/Earlymenopause/diabetics/HPV
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Where ?
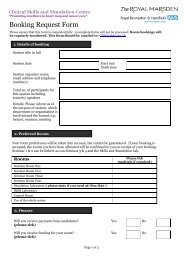
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Central referrals – <strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Phone 0800 731 2325Fax 020 8661 3149Emailrmh.referrals@nhs.net
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>When ?
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>When
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Diagnosis - Haematuria• Paediatric population – 1%• Young Adults – 5%• Adults over 50 – 10%• Macroscopic haematuria is the commonest presentation ofbladder cancer• Almost all patients will have macro or microhaematuria• Degree of bleeding is not proportional to stage• Bleeding due to infection – some patients will have necroticinfected element within a tumour not just inflammation
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Bladder cancer - symptoms• Commonest symptom is painless haematuria• DO NOT IGNORE painful haematuria• Pronounced irritative symptoms (? cis/invasive)• Loin pain (ureteric obstruction) - rare• Pelvic mass & cachexia – very rare
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Definition - Haematuria• According to Renal Association and British Associationof Urological Surgeons blood in the urine is eitherdefined as• Visible haematuria (VH) – macroscopic or gross• Non visible haematuria (NVH) - microscopic• NVH is subdivided into symptomatic –s-NVH andasymptomatic a-NVH• Definition of NVH varies from >3 rbc/hpf spun to >5rbc/microlitre (dipstick + is >10 rbc/hpf)
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Dipstick testing - pitfalls• Dip testing is based on the alteration of a chromagenby the peroxidase activity of haemoglobin• False positives - myoglobinuria/oxidisingagents/peroxidases• False negatives – high levels ascorbic acid/nitrite/pH
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Haematuria – evidence for investigation2 studies• 1930 pts attending haematuria clinic (1994-97)• 61% patients no pathology / 13% UTI / 2% stone disease• 12% bladder cancer• Macroscopic – 24% / microscopic – 9.4%• 4020 pts• Incidence of bladder cancer• Macroscopic haematuria 19% / microscopic 5%
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Screening for bladder cancer: Is it effective ?• Dipstick testing in 2356 men over 60 years (1992)• 20% had recurrent haematuria (n=474)• 319 agreed to urological examination• 17 (5.3% of cohort / 0.7% of tested) asymptomatic mendiagnosed with cancer• Large no. investigations• Prohibitive cost• Targeted screening – smokers 3.3% (inc. cytol/NMP22)
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>How ?
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Diagnosis – In clinic• History/examination• MSU• Urine Cytology (specificity 95%, sensitivity 49%)Other urinary markers – NMP22/BTA/Telomerase• Flexible cystoscopy• Upper tract imaging (USS)/CTU• TURBT (transurethral resection of bladder tumour) – followedby single dose Mitomycin C
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Bladder cancer – cell types?• Transitional cell carcinoma – 95%• Squamous cell carcinoma – 3% (Egypt 75%)• Adenocarcinoma (primary or urachal) – 1-2%• Rarely metastases from uterus, rectum, breast andovary
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Superficial Bladder Cancer
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Superficial Bladder Cancer
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Superficial Bladder Cancer• Up to 80% patients present with superficial disease• In such patients risk of distant disease is low• Natural history of bladder cancer based on 2 separate butrelated processesTumour recurrence - 50 to 70% overall (Grossman H,Oncology: 1996). This high recurrence rate in distantfields, so called polychronotropism suggests ‘field defect’in the entire lining epitheliumTumour progression to a higher stage (10 - 15%)
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Superficial Bladder Cancer - management• Management requires a long term commitment• Follow-up may be for life• Most cases “routine” but important to recognisethose with disease that will progress• Such patients must be identified early and selectedfor more aggressive therapy e.g.cystectomy/radiotherapy
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Superficial Bladder Cancer• Superficial bladder cancer is a stage grouping of 3distinct tumours– pTa (papillary and non invasive)– pT1 (invading lamina propria only)– pTis (cis - carcinoma in situ)• <strong>The</strong>y are grouped together as they can be managedin a similar way; endoscopically and usingintravesical therapy
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Bladder Cancer - G1pTa
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Muscle Invasive Bladder Cancer
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Muscle Invasive Bladder Cancer
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Muscle Invasive Bladder Cancer• Stage Grouping T2-T4• Historical standard treatment – radical surgeryNow treatment options are• Neo-adjuvant chemotherapy then radical surgery• Radical surgery then adjuvant chemotherapy• Chemo-radiotherapy
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>Surgical Solutions after Radical Cystectomy• Incontinent cutaneous urinary diversion– ileal (or other) conduit• Continent stomal diversions– Mitrofanoff, Indiana, Kock• Orthotopic neobladder– Ileal (Studer, Hautman), Hemi-Kock, Ileocaecal• Ureterosigmoidostomies
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>
<strong>The</strong> <strong>Royal</strong> <strong>Marsden</strong>
Fin – Thank you<strong>Alan</strong> <strong>Thompson</strong>Consultant Urological Surgeon