INSPECTION FORM OF RURAL HEALTH CENTRE - PHSRP - Punjab
INSPECTION FORM OF RURAL HEALTH CENTRE - PHSRP - Punjab
INSPECTION FORM OF RURAL HEALTH CENTRE - PHSRP - Punjab

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
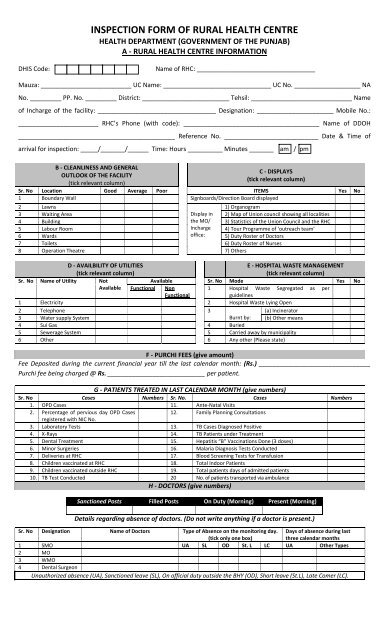
<strong>INSPECTION</strong> <strong>FORM</strong> <strong>OF</strong> <strong>RURAL</strong> <strong>HEALTH</strong> <strong>CENTRE</strong><br />
<strong>HEALTH</strong> DEPARTMENT (GOVERNMENT <strong>OF</strong> THE PUNJAB)<br />
A ‐ <strong>RURAL</strong> <strong>HEALTH</strong> <strong>CENTRE</strong> IN<strong>FORM</strong>ATION<br />
DHIS Code:<br />
Name of RHC: __________________________________<br />
Mauza: __________________________ UC Name: _______________________________ UC No. ___________________ NA<br />
No. _________ PP. No. _________ District: _________________________ Tehsil: _____________________________ Name<br />
of Incharge of the facility: __________________________________ Designation: ______________________ Mobile No.:<br />
_______________________ RHC’s Phone (with code): _______________________________________ Name of DDOH<br />
_____________________________________________ Reference No. ___________________________ Date & Time of<br />
arrival for inspection: _____/_______/______ Time: Hours __________ Minutes _______<br />
am / pm<br />
B ‐ CLEANLINESS AND GENERAL<br />
OUTLOOK <strong>OF</strong> THE FACILITY<br />
(tick relevant column)<br />
C ‐ DISPLAYS<br />
(tick relevant column)<br />
Sr. No Location Good Average Poor ITEMS Yes No<br />
1 Boundary Wall Signboards/Direction Board displayed<br />
2 Lawns<br />
1) Organogram<br />
3 Waiting Area Display in 2) Map of Union council showing all localities<br />
4 Building the MO/ 3) Statistics of the Union Council and the RHC<br />
5 Labour Room Incharge 4) Tour Programme of ‘outreach team’<br />
6 Wards office: 5) Duty Roster of Doctors<br />
7 Toilets 6) Duty Roster of Nurses<br />
8 Operation Theatre 7) Others<br />
D ‐ AVAILBILITY <strong>OF</strong> UTILITIES<br />
(tick relevant column)<br />
E ‐ HOSPITAL WASTE MANAGEMENT<br />
(tick relevant column)<br />
Sr. No Name of Utility Not<br />
Available Sr. No Mode Yes No<br />
Available Functional Non<br />
1 Hospital Waste Segregated as per<br />
Functional<br />
guidelines<br />
1 Electricity 2 Hospital Waste Lying Open<br />
2 Telephone 3<br />
(a) Incinerator<br />
3 Water supply System Burnt by: (b) Other means<br />
4 Sui Gas 4 Buried<br />
5 Sewerage System 5 Carried away by municipality<br />
6 Other 6 Any other (Please state)<br />
F ‐ PURCHI FEES (give amount)<br />
Fee Deposited during the current financial year till the last calendar month: (Rs.) ________________________________<br />
Purchi fee being charged @ Rs. ____________________________ per patient.<br />
G ‐ PATIENTS TREATED IN LAST CALENDAR MONTH (give numbers)<br />
Sr. No Cases Numbers Sr. No. Cases Numbers<br />
1. OPD Cases 11. Ante‐Natal Visits<br />
2. Percentage of pervious day OPD Cases<br />
12. Family Planning Consultations<br />
registered with NIC No.<br />
3. Laboratory Tests 13. TB Cases Diagnosed Positive<br />
4. X‐Rays 14. TB Patients under Treatment<br />
5. Dental Treatment 15. Hepatitis “B” Vaccinations Done (3 doses)<br />
6. Minor Surgeries 16. Malaria Diagnosis Tests Conducted<br />
7. Deliveries at RHC 17. Blood Screening Tests for Transfusion<br />
8. Children vaccinated at RHC 18. Total Indoor Patients<br />
9. Children vaccinated outside RHC 19. Total patients days of admitted patients<br />
10. TB Test Conducted 20 No. of patients transported via ambulance<br />
H ‐ DOCTORS (give numbers)<br />
Sanctioned Posts Filled Posts On Duty (Morning) Present (Morning)<br />
Details regarding absence of doctors. (Do not write anything if a doctor is present.)<br />
Sr. No Designation Name of Doctors Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
1 SMO UA SL OD St. L LC UA Other Types<br />
2 MO<br />
3 WMO<br />
4 Dental Surgeon<br />
Unauthorized absence (UA), Sanctioned leave (SL), On official duty outside the BHY (OD), Short leave (St.L), Late Comer (LC).
I ‐ PARAMEDICS (OTHER THAN DOCTORS)<br />
PARAMEDICS<br />
INCLUDES:<br />
Charge Nurse, Dispenser, Dresser, Dental Assistant, Operation Theatre Assistant, Medical Assistant,<br />
Anesthesia Assistant, Medical Technician, Health Technician<br />
Sr. No Staff Category Sanctioned Filled Posts Present<br />
1 Nurses<br />
2 Other paramedics (Other than nurses)<br />
Details regarding absence of Paramedics. (Do not write anything if staff is present.)<br />
Sr. No<br />
1<br />
2<br />
3<br />
Designation<br />
Name of Staff<br />
Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
UA SL OD St. L LC UA Other Types<br />
J ‐ ALTERNATIVE MEDICATION STAFF<br />
ALTERNATIVE MEDICATION<br />
STAFF INCLUDES:<br />
Homeo Doctor, Hakeem/Tabeeb, Dawa Saaz, Homeo Dispenser, Dawa Kobe<br />
Sanctioned Posts Filled Posts Present<br />
Details regarding absence of alternative medication staff. (Do not write anything if staff is present.)<br />
Sr. No<br />
1<br />
2<br />
3<br />
Designation<br />
Name of Staff<br />
Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
UA SL OD St. L LC UA Other Types<br />
K ‐ PREVENTIVE / OUTREACH STAFF<br />
PREVENTIVE / OUTREACH STAFF<br />
INCLUDES:<br />
LHV, RHI< Midwife, Dai, Vaccinator, CDC Supervisor, Sanitary Patrol, Sanitary Inspector,<br />
Sanitary Worker<br />
Sanctioned Posts Filled Posts Present<br />
Sr. No<br />
1<br />
2<br />
3<br />
Details regarding absence of Preventive / outreach staff.(Do not write anything if staff is present.)<br />
Designation<br />
Name of Staff<br />
Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
UA SL OD St. L LC UA Other Types<br />
L ‐ TECHNICAL STAFF<br />
TECHNICAL STAFF INCLUDES:<br />
Dental Technician, Lab. Technician, X‐Ray Technician, X‐Ray Assistant, Lab. Assistant, Microscopist,<br />
Radiographer<br />
Sanctioned Posts Filled Posts On Duty (Morning) Present (Morning)<br />
Sr. No<br />
1<br />
2<br />
3<br />
Designation<br />
Detail regarding absence of Technical Staff. (Do not write anything if staff is present).<br />
Name of Staff<br />
Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
UA SL OD St. L LC UA Other Types
M ‐ ADMIN / SUPPORT STAFF<br />
ADMIN / SUPPORT INCLUDES:<br />
Accountant, Senior Clerk, Junior Clerk, Computer Operator, Driver, Cook, Store Keeper, Naib Qasid,<br />
Tubewell Operator, Ward Servant, Water Carrier, Chowkidar, Mali, Peon, Sweeper<br />
Sanctioned Posts Filled Posts On Duty (Morning) Present (Morning)<br />
Detail regarding absence of Admin / Support Staff. (Do not write anything if staff is present).<br />
Sr. No<br />
1<br />
2<br />
3<br />
Designation<br />
Name of Staff<br />
Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
UA SL OD St. L LC UA Other Types<br />
N ‐ VACANT POSTS (please write full name of post)<br />
Sr. No Name of Post Number of Vacant<br />
Post<br />
Sr. No Name of Post Number of<br />
Vacant Post<br />
1 7<br />
2 8<br />
3 9<br />
4 10<br />
5 11<br />
6 12<br />
O ‐ <strong>INSPECTION</strong> <strong>OF</strong> THE FACILITY BY DISTRICT GOVERNMENT <strong>OF</strong>FICERS<br />
From Inspection Register. (give number / dates)<br />
Sr. No Inspecting Officer DDO (H) DO (H) EDO (H) DCO or his<br />
Representative<br />
1 Number of inspections made during<br />
the last six calendar months as per<br />
record of inspection book<br />
2 Date of Last Inspection<br />
Sr.<br />
No.<br />
P ‐ AVAILABILITY <strong>OF</strong> MEDICINES (give numbers of tablets / bottles etc.)<br />
(Medicines physically available on the date of visit in the stock & as per Medicines Stock Register)<br />
Medicines<br />
1 Cap. Amoxicillin<br />
2 Syp. Amoxicillin<br />
3 Tab. Cotrimoxazole<br />
4 Syp. Cotrimoxazole<br />
5 Any Other antibiotic Tablet<br />
6 Tab. Metronidazole<br />
7 Syp. Metronidazole<br />
8 Inj. Ampicillin<br />
9 Tab Diclofenac<br />
10 Inj. Diclofenac<br />
11 Syrup Paracetamol<br />
12 Chloroquine Tab<br />
13 Syrup Salbutamol<br />
14 Syp. Antihelminthic<br />
15 I/V Infusions<br />
16 Inj. Dexamethasone<br />
17 Iron/Folic Tab.<br />
18 ORS (Packets)<br />
19 Oral Contraceptive Pills<br />
20 Anti‐Histamine Tab.<br />
21 Inj. Anti‐Histamine<br />
22 Anti‐Tuberculosis Drugs<br />
23 Tetanus Toxoid Injections<br />
24 Inj. Atropin<br />
25 Inj. Adrenaline<br />
26 Ant acid Tab.<br />
27 Bandages<br />
28 Antiseptic Solution (Bottles)<br />
29 Disposable Syringes<br />
Yes<br />
Available<br />
No<br />
Balance as on<br />
1 st of last<br />
month (1)<br />
Received Since<br />
1 st of last<br />
month (2)<br />
Total<br />
3=(1+2)<br />
Consumed<br />
since 1 st of last<br />
month till<br />
today (4)<br />
Balance as per<br />
register<br />
5=(3‐4)
Q ‐ PUBLIC OPINION (please give number of persons in the relevant columns.)<br />
Views<br />
1) Presence of Doctors<br />
2) Attitude of doctors towards patients<br />
3) Waiting Time<br />
4) Free availability of medicines<br />
5) Vaccinators outreach<br />
6) Vaccination at RHC<br />
Note:<br />
Number of persons<br />
contacted in the<br />
catchment area<br />
Satisfactory<br />
Names and Contact Numbers of at least two persons interviewed during the visit<br />
PUBLIC OPINION<br />
Unsatisfactory<br />
Average<br />
No Response<br />
Sr. No. Name Address Contact Number<br />
R ‐ INDOOR PATIENTS DEPARTMENT<br />
Functional<br />
Non‐Functional<br />
Total Number of<br />
admitted patients<br />
Male<br />
Female<br />
Children<br />
(under 12 Years)<br />
Sr.<br />
No.<br />
S ‐ DEVELOPMENT SCHEMES / PROVISION <strong>OF</strong> MISSING FACILITIES (TICK THE COLUMN)<br />
Missing facilities Funds provided by Status of work Quality Observations<br />
<strong>PHSRP</strong> District<br />
Govt.<br />
Not<br />
Started<br />
Halted % Completed<br />
(Give number)<br />
Poor Avg. Good (Use extra page if<br />
required)<br />
1 RHC Building<br />
2 Residences<br />
3 Boundary wall<br />
4 Electricity<br />
5 Drinking Water<br />
6 Latrine/Toilet<br />
7 Furniture Sui Gas<br />
8 Sewerage<br />
9 Other<br />
10<br />
Sr. No.<br />
Name of Equipment<br />
1 X‐Ray Machine<br />
2 Dental Unit<br />
3 Dental X‐ray Machine<br />
4 ECG Machine<br />
5 Hot Air Oven<br />
6 Auto Clave<br />
7 Sterilizer<br />
8 Nebulizer<br />
9 Ultrasound Machine<br />
10 O.T. ceiling Light<br />
11 O.T. Table<br />
12 General Surgery Instrument Set<br />
13 Obstetric Instrument Set<br />
14 Fetal Heart Detector<br />
15 Oxygen Cylinder with flow meters<br />
16 Lab Equipment<br />
17 Ambu Bag<br />
18 Bulb Sucker<br />
19 Baby Warmer<br />
Sr. No.<br />
Name of Equipment<br />
1 Ambulance<br />
2 Air‐conditioner for Operation Theatre<br />
3 Computer<br />
4 Printer<br />
5 UPS<br />
6 Electric Generator<br />
7 General Store (Liren, Bedside lockers etc.)<br />
T (i) – Medical Equipment (give numbers)<br />
Available<br />
Functional<br />
If Non‐Functional<br />
Repairable Unserviceable<br />
T (ii) – NON MEDICAL Equipment (give numbers)<br />
Available<br />
Functional<br />
If Non‐Functional<br />
Repairable Unserviceable<br />
Remarks<br />
Remarks
U– RESIDENCES (give numbers)<br />
Sr. No.<br />
1<br />
2<br />
3<br />
Name of Post<br />
Residence<br />
Available<br />
Residence<br />
Occupied<br />
(Yes/No)<br />
Physical Status of Residence<br />
Reside able Not reside able<br />
Remarks<br />
V– EMERGENCY<br />
Sr.<br />
No.<br />
Emergency Yes No<br />
1 Emergency Room Properly equipped<br />
2 Medicines available in Emergency Room<br />
3 Medicines supplied free of cost during first 24 hrs.<br />
4 Emergency staff available as per roster<br />
W– SERVICES<br />
Services Yes No<br />
AIDS & HEPATTIS CONTROL<br />
1 100% Blood screening for HIV, HBV & HCV<br />
2 Syringe cutters available<br />
3 Syringe cutters being used<br />
EPI<br />
4 Cold chain intact<br />
5 Temperature chart maintained<br />
6 All vaccines available at EPI center<br />
NATIONAL PROGAM FOR FP/PHC<br />
7 LHW monthly meeting held<br />
8 LHW monthly meeting compiled<br />
9 Monthly supplies / medicines replenished<br />
MCH<br />
10 Labour Room Functional equipment available<br />
11 Operation Theater for Gynae / Obstetrics functional<br />
12 Family Planning services being provided<br />
X– REFERRALS<br />
Sr. No. Indicator Yes Number<br />
1 Patients referred to the facilities<br />
2 Patients referred from the facilities<br />
Y– MONTHLY PER<strong>FORM</strong>ANCE<br />
Sr. No. Indicator Monthly Target Performance<br />
1 Daily OPD attendance<br />
2 Children given full Immunization coverage<br />
3 Delivery coverage at facility<br />
Z– GENERAL REMARKS<br />
Time of Departure from the facility: Hours______Minutes____________am<br />
/ pm<br />
Certified that this Rural Health Centre was inspected today by the undersigned and the information stated<br />
above is as per facts and record.<br />
____________________ ________________________________ ______________________<br />
Signature of DDOH/MEA Signatures & Stamp of MO/Incharge Signatures of DMO/EDO(H)
EVENING SHIFT<br />
Date of Visit:______/______/________<br />
Sr.<br />
No.<br />
Designation<br />
1 Doctor<br />
2 Nurses<br />
On duty in evening shift<br />
(give numbers)<br />
Present in<br />
evening shift<br />
(give numbers)<br />
Time of Arrival: Hours___________Minutes__________<br />
3 Other Paramedics<br />
4 Technical Staff<br />
Time of Departure: Hours_________Minutes_________<br />
5 Admn/Support Staff<br />
DETAILS <strong>OF</strong> ABSENCE<br />
(Do not write anything if staff is present.)<br />
Sr. No. Designation Name Type of Absence on the monitoring day.<br />
(tick only one box)<br />
Days of absence during<br />
last three calendar<br />
months<br />
UA SL OD St. L LC UA Other Types<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
______________ ________________________________ _________________<br />
Signature of DDOH/MEA Signatures & Stamp of MO/Incharge Signatures of DMO/EDOH<br />
NIGHT SHIFT<br />
Date of Visit:______/______/________<br />
Sr.<br />
No.<br />
Designation<br />
1 Doctor<br />
On Call as per duty<br />
roster (give numbers)<br />
Available on<br />
Call (give<br />
numbers)<br />
Sr.<br />
No.<br />
Designation<br />
1 Nurses<br />
2 Other Paramedics<br />
3 Technical Staff<br />
4 Admn/Support Staff<br />
On duty in evening shift<br />
(give numbers)<br />
Present in<br />
evening shift<br />
(give numbers)<br />
Time of Arrival: Hours___________Minutes__________<br />
Time of Departure: Hours_________Minutes_________<br />
DETAILS <strong>OF</strong> ABSENCE<br />
(Do not write anything if staff is present.)<br />
Sr. No. Designation Name Type of Absence on the monitoring<br />
day. (tick only one box)<br />
Days of absence during last<br />
three calendar months<br />
UA SL OD St. L LC UA Other Types<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
______________ ________________________________ _________________<br />
Signature of DDOH/MEA Signatures & Stamp of MO/Incharge Signatures of DMO/EDOH