

GAT Issue: The Olympics and Anaesthesia - aagbi
GAT Issue: The Olympics and Anaesthesia - aagbi
GAT Issue: The Olympics and Anaesthesia - aagbi

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
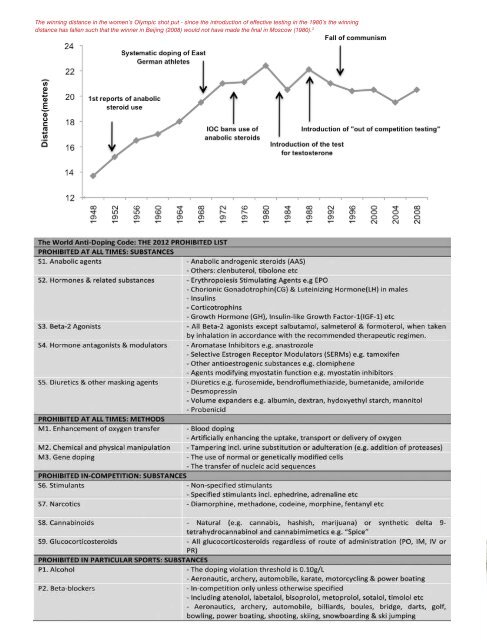
<strong>The</strong> winning distance in the women’s Olympic shot put - since the introduction of effective testing in the 1980’s the winning<br />
distance has fallen such that the winner in Beijing (2008) would not have made the final in Moscow (1980). 3<br />
Penalties for Doping<br />
<strong>The</strong> WADA code discusses in detail the types of doping violations<br />
<strong>and</strong> their associated penalties, but the responsible body for the<br />
administration <strong>and</strong> enforcement of this is the individual National Anti-<br />
Doping Organisation’s. Ineligibility sanctions range from 1 year to lifetime<br />
bans <strong>and</strong> the penalties h<strong>and</strong>ed down by doping authorities depend on<br />
many factors, for example, first versus second time offences <strong>and</strong> missed<br />
tests versus trafficking activities. This remains an area of controversy<br />
in the international anti-doping community as the lack of hard <strong>and</strong> fast<br />
rules introduces a degree of inconsistency; the penalties h<strong>and</strong>ed down<br />
in different countries <strong>and</strong> different sports for the same violation can vary<br />
greatly. It is felt that this “loophole” allows some organisations to take a<br />
“soft approach” to performance enhancement.<br />
On home soil, Dwain Chambers, the British sprinter banned from<br />
competition for 2 years in 2003 for using tetrahyrdrogestrinone, has<br />
recently won his appeal against the British Olympic Association <strong>and</strong> will<br />
now be eligible to compete in this month’s games here in London if he<br />
qualifies for Team GB. <strong>The</strong> BOA bylaw in contention held that any athlete<br />
receiving a sanction of 6 months or more on doping violations would<br />
not be eligible to represent Great Britain at Olympic events at any time<br />
in their future career. <strong>The</strong> Court of Arbitration in Sport has upheld the<br />
appeal by ruling in support of WADA’s stance that this policy amounts<br />
to an additional sanction on the athlete, which is in breach of its global<br />
code of which the BOA is a signatory. <strong>The</strong> WADA code is under review<br />
at present, amendments will come into effect in 2013, <strong>and</strong> the BOA is<br />
now likely to concentrate its efforts on their proposal to WADA that first<br />
offences should carry a m<strong>and</strong>atory 4-year ban as well as missing one<br />
Olympic Games, in the wake of this decision.<br />
Substances in use<br />
Androgenic Anabolic steroids (AAS)<br />
<strong>The</strong> impact of anabolic steroid use came to the public’s attention with the<br />
disqualification of Ben Johnson, after winning gold in the men’s 100-metre<br />
sprint in Seoul in 1988, when stanazolol was detected in his urine. Clinical<br />
trials confirm that AAS increase muscle strength <strong>and</strong> mass through a<br />
number of mechanisms that are dose dependant, <strong>and</strong> that these effects<br />
are additive to resistance training alone. Athletes are known to have used<br />
doses up to 30-times higher than the physiological replacement dose<br />
of these hormones. AAS have a wide range of serious adverse effects<br />
including virilisation <strong>and</strong> reduced fertility, hepatotoxicity <strong>and</strong> increased<br />
risk of hepatocellular carcinoma, dyslipidaemia <strong>and</strong> increased risk of<br />
myocardial infarction, depression, mania <strong>and</strong> aggression.<br />
Erythropoietin (EPO) <strong>and</strong> Blood Transfusion<br />
Thought to have started in the 1970’s, blood doping is a method still<br />
utilised by elite athletes <strong>and</strong> has resulted in high profile bans recently.<br />
Training at high altitude can induce endogenous EPO production in the<br />
renal tubules, promoting an increase in the total red cell volume, which<br />
increases oxygen delivery to the muscles, in turn improving performance<br />
particularly in endurance sports. Only about 50% of competitive athletes<br />
respond to altitude training <strong>and</strong> it is notable that non-responders do not<br />
improve their aerobic capacity. Recombinant EPO <strong>and</strong> its analogues, or<br />
homologous <strong>and</strong> autologous blood transfusion, are alternative methods<br />
used by athletes to exp<strong>and</strong> their erythrocyte volume. <strong>The</strong> chief risk<br />
associated with this practice is thrombosis, but the risk of infections<br />
associated with blood transfusion is of particular concern when this<br />
occurs in an unregulated fashion.<br />
Growth Hormone (GH)<br />
GH is a naturally occurring peptide hormone produced by the anterior<br />
pituitary gl<strong>and</strong>. “<strong>The</strong> Underground Steroid H<strong>and</strong>book” written by Dan<br />
Duchaine in 1982 advocated its use for performance enhancement at least<br />
a decade before endocrinologists began prescribing it for therapeutic<br />
replacement. <strong>The</strong> startling results achieved with replacement of GH in<br />
deficient individuals have not been reproduced to the same extent in<br />
trials using healthy adults, but increased skeletal muscle mass leading<br />
to increased strength <strong>and</strong> power output have been observed, as well<br />
as increases in the bioavailability of glucose <strong>and</strong> fatty acids. <strong>The</strong> effects<br />
are short-lived, disappearing within weeks of the cessation of GH use,<br />
<strong>and</strong> are not necessarily matched by an increase in other performance<br />
indices such as the maximal uptake of oxygen (VO 2<br />
max). However, these<br />
clinical studies may not be suited to assess the effects of GH in individual<br />
athletes who often use higher doses than those used in the trials <strong>and</strong> who<br />
often combine GH with other performance enhancing drugs. <strong>The</strong> specific<br />
test utilised by WADA for GH has a limited detection window of 24 hours,<br />
which ensures this remains a concern for doping organisations. Indeed,<br />
a recent investigation into Major League Baseball by a US senator found<br />
a high level of GH use among players for performance enhancement<br />
<strong>and</strong> to speed recovery from injury. <strong>The</strong> side effects of GH use include<br />
fluid retention leading to hypertension <strong>and</strong> headaches, diabetes <strong>and</strong> a<br />
cardiomyopathy. Anecdotally, some athletes use doses much higher than<br />
those required for therapeutic replacement, <strong>and</strong> it is reasonable to predict<br />
that they may develop features of acromegaly over time. Pharmaceutically<br />
available GH is all produced using recombinant technology, but some of<br />
the GH available to athletes on the black market is still pituitary-derived<br />
which introduces the risk of prion disease to illicit users.<br />
Insulin Like Growth Factor-1 (IGF-1) <strong>and</strong> Insulin<br />
As the tests for detecting GH abuse develop there are anecdotal reports<br />
that athletes, for example weightlifters, are increasingly turning to insulin<br />
<strong>and</strong> IGF-1 as alternative performance enhancing agents. <strong>The</strong> two<br />
substances have broadly similar actions in their anabolic effects <strong>and</strong> their<br />
action on glucose metabolism, both of which might have abuse potential.<br />
Adverse effects are principally hypoglycaemia <strong>and</strong> weight gain, but this<br />
may be less problematic in an individual whose diet <strong>and</strong> training regimen<br />
are closely monitored. After concerns were raised by the Russian medical<br />
officer at the Nagano Olympic Games, the IOC immediately banned the<br />
use of insulin in individuals without diabetes. WADA has subsequently<br />
endorsed this <strong>and</strong> people with diabetes requiring insulin treatment must<br />
obtain a TUE, however this might prove a difficult area to police.<br />
<strong>The</strong> true prevalence of doping today is unknown due to the secrecy around<br />
it; but the advent of professional sport <strong>and</strong> the huge financial rewards that<br />
go with being the best, coupled with an ever increasing pharmacopoeia<br />
<strong>and</strong> the athlete’s innate drive to win may all act to encourage continued<br />
use of these methods. This damages the reputation of sport <strong>and</strong> may<br />
harm the health of the athletes. Stringent efforts are therefore needed to<br />
allow athletes around the world to “play true”.<br />
Kate O’Connor<br />
ST6, Bristol School of <strong>Anaesthesia</strong><br />
Professor Richard I.G. Holt<br />
Human Development <strong>and</strong> Health Academic Unit,<br />
University of Southampton<br />
References<br />
1. <strong>The</strong> official website of the World Anti-Doping Agency: www.wada-ama.org<br />
2. <strong>The</strong> official website of UK Anti-Doping: www.ukad.org.uk<br />
3. Holt, R.I.G. Diabetes <strong>and</strong> Doping. Chapter 8, 167-192. In Gallen, I. Type 1<br />
Diabetes. Clinical Management of the Athlete. (1st Ed, 2012) Springer.<br />
4. www.wada-ama.org/en/Anti-Doping-Community/Athletes-/QA-on-<br />
Whereabouts/<br />
5. www.wada-ama.org/en/Science-Medicine/Prohibited-List/QA-on-2012-<br />
Prohibited-List/<br />
6. www.wada-ama.org/en/Anti-Doping-Community/Athletes-/QA-on-TUEs/<br />
<strong>Anaesthesia</strong> News July 2012 • <strong>Issue</strong> 300 19














