BRAINSTEM REFLEXES: ELECTRODIAGNOSTIC TECHNIQUES ...
BRAINSTEM REFLEXES: ELECTRODIAGNOSTIC TECHNIQUES ...
BRAINSTEM REFLEXES: ELECTRODIAGNOSTIC TECHNIQUES ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
INVITED REVIEW ABSTRACT: An overview is provided on the physiological aspects of the<br />
brainstem reflexes as they can be examined by use of clinically applicable<br />
neurophysiological tests. Brainstem reflex studies provide important information<br />
about the afferent and efferent pathways and are excellent physiological<br />
tools for the assessment of cranial nerve nuclei and the functional<br />
integrity of suprasegmental structures. In this review, the blink reflex after<br />
trigeminal and nontrigeminal inputs, corneal reflex, levator palpebrae inhibitory<br />
reflex, jaw jerk, masseter inhibitory reflex, and corneomandibular reflex<br />
are discussed. Following description of the recording technique, physiology,<br />
central pathways, and normative data of these reflexes, including an account<br />
of the recording of recovery curves, the application of these reflexes is<br />
reviewed in patients with various neurological abnormalities, including trigeminal<br />
pain and neuralgia, facial neuropathy, and brainstem and hemispherical<br />
lesions. Finally, simultaneous electromyographic recording from<br />
the orbicularis oculi and the levator palpebrae muscles is discussed briefly in<br />
different eyelid movement disorders.<br />
© 2002 Wiley Periodicals, Inc. Muscle Nerve 26: 14–30, 2002<br />
<strong>BRAINSTEM</strong> <strong>REFLEXES</strong>: <strong>ELECTRODIAGNOSTIC</strong><br />
<strong>TECHNIQUES</strong>, PHYSIOLOGY, NORMATIVE DATA,<br />
AND CLINICAL APPLICATIONS<br />
M. ARAMIDEH, MD, PhD, 1,2 and B.W. ONGERBOER DE VISSER, MD, PhD 1<br />
1 Department of Neurology and Clinical Neurophysiology Unit, Academic Medical Center, Meibergdreef 9, 1105 AZ,<br />
Amsterdam, The Netherlands<br />
2 Department of Neurology/Clinical Neurophysiology, Medical Center Alkmaar, P.O. Box 501, 1800 AM,<br />
Alkmaar, The Netherlands<br />
Accepted 1 February, 2002<br />
The recording of brainstem reflexes provides valuable<br />
information on the functional integrity of the<br />
brainstem and allows the afferent and efferent pathways<br />
of these reflexes to be assessed. Many structural<br />
abnormalities, such as tumors or infarcts at the level<br />
of the brainstem, may cause abolition of these reflexes.<br />
Recording of different brainstem reflexes is<br />
helpful to exclude structural lesions or, conversely,<br />
to localize more accurately lesions within the brainstem.<br />
In the latter case, tailored magnetic resonance<br />
imaging (MRI) of this region may be sufficient. Recording<br />
of the brainstem reflexes also plays an important<br />
role in the selection of patients for additional<br />
MRI and in assessing objectively functional<br />
abnormalities of the cranial nerves by elucidating<br />
Abbreviations: LP, levator palpebrae superioris muscle; MIR, masseter<br />
inhibitory reflex; OO, orbicularis oculi muscle; R1, early response of blink<br />
reflex; R2, late response of blink reflex; SP1, first silent period; SP2, second<br />
silent period<br />
Key words: blink reflex; brainstem reflexes; corneal reflex; cranial nerves;<br />
masseter reflex<br />
Correspondence to: M. Aramideh; e-mail: m.Aramideh@mca.nl<br />
© 2002 Wiley Periodicals, Inc.<br />
Published online 1 May 2002 in Wiley InterScience (www.<br />
interscience.wiley.com). DOI 10.1002/mus.10120<br />
subtle changes in one or more variables of the reflex<br />
features, such as amplitude or latency of the responses.<br />
67 Studies of different reflex responses also<br />
provide information about the physiology and<br />
pathophysiology of segmental and suprasegmental<br />
control mechanisms on the brainstem reflexes and<br />
help to differentiate between the segmental and suprasegmental<br />
origin of abnormalities.<br />
This article provides an overview on the recording<br />
techniques, physiology, and normative data of<br />
different brainstem reflexes. Clinical applications<br />
are discussed briefly in patients with trigeminal and<br />
facial neuropathies, brainstem or hemispheric lesions,<br />
and extrapyramidal or eyelid movement disorders.<br />
ORBICULARIS OCULI <strong>REFLEXES</strong><br />
Blink Reflex. The British physician Overend 85 first<br />
elicited the blink reflex by tapping one side of the<br />
forehead. Kugelberg 62 analyzed the blink reflex electromyographically<br />
by electrically stimulating the supraorbital<br />
nerve. Reflex responses from the inferior<br />
portion of both orbicularis oculi muscles may be recorded<br />
simultaneously by surface or needle elec-<br />
14 Brainstem Reflexes MUSCLE & NERVE July 2002
trodes. Stimuli should be delivered at intervals of 7 s<br />
or longer, while the subject is kept alert. 14 The afferent<br />
limb of the reflex is mediated by the ophthalmic<br />
division of the trigeminal nerve. 25,62 The facial<br />
nerve subserves the efferent limb.<br />
The electrical stimulation of the supraorbital<br />
nerve elicits two responses (Fig. 1); the first or early<br />
response, R1, is a brief unilateral response that occurs<br />
with a latency of about 10 ms in the orbicularis<br />
oculi muscle ipsilateral to the side of stimulation.<br />
The second or late response, R2, has a latency of<br />
about 30 ms. The R1 response is regarded as delayed<br />
if its latency exceeds 13.0 ms and R2 is regarded as<br />
delayed if its latency exceeds 41 ms. 59,80 A latency<br />
difference between the two sides exceeding 1.5 ms<br />
for R1 and 5.0 ms 59 or 8.0 ms 80 for R2 is also considered<br />
abnormal.<br />
Stimulation of the infraorbital nerve always<br />
evokes an R2 response but not necessarily an R1.<br />
When R1 is not present, it is difficult to evaluate R2,<br />
because of its wide range in latency. An absent R2,<br />
however, is certainly abnormal.<br />
The R1 response is conducted through the pons<br />
and is relayed via an oligosynaptic arc, probably consisting<br />
of one or two interneurons, located in the<br />
vicinity of the main sensory nucleus of the trigeminal<br />
nerve 56,74,90 (Fig. 1). For the R2 responses, it has<br />
been established that afferent impulses are conducted<br />
through the descending spinal tract of the<br />
trigeminal nerve in the pons and medulla oblongata<br />
before they reach the caudal spinal trigeminal<br />
nucleus. 58,82 From there, impulses are relayed by a<br />
medullary pathway that ascends bilaterally to reach<br />
the facial nuclei in the pons. These trigeminofacial<br />
connections are thought to pass through the lateral<br />
tegmental field, which lies medial to the spinal trigeminal<br />
nucleus. 50,82 The observations of Aramideh<br />
et al. 6 established that the uncrossed, ascending trigeminofacial<br />
pathway originates at the level of the<br />
lower medulla oblongata and that the contralateral<br />
R2 response is established by way of an ascending<br />
trigeminofacial connection that crosses the midline<br />
at the level of the lower third of the medulla oblongata.<br />
The blink reflex is influenced by many suprasegmental<br />
structures, including the motor cortex, the<br />
postcentral area of the cortex, and the basal ganglia.<br />
38<br />
Blink Reflexes Evoked by Nontrigeminal Inputs. Somatosensory<br />
Blink Reflex. An electrical stimulus to<br />
peripheral nerves, specifically the median nerve at<br />
the wrist, may induce responses in the orbicularis<br />
oculi muscles. 71,94 The circuits involved in these re-<br />
FIGURE 1. (A) Normal early (R1) and bilateral late (R2) responses<br />
of the blink reflex. Responses are shown from the right<br />
(r) and left (l) OO muscles after stimulation of the right (r*) and (l*)<br />
supraorbital nerves. (B) Diagram showing the presumed location<br />
of the bulbar interneurons subserving the two components of the<br />
blink reflex. (VII, facial nucleus; VII N, facial nerve; VI, abducens<br />
nucleus; Vp, principal trigeminal nucleus; Vm, trigeminal motor<br />
nucleus; V N, trigeminal nerve; MED RET, medial reticular field;<br />
LAT RET, lateral reticular field).<br />
sponses are not fully understood. However, the somatosensory-induced<br />
blink reflex may be part of a<br />
generalized activation of the startle circuit 53 or the<br />
expression of a release phenomenon. 72 Electrical<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 15
stimulation of the median nerve may also induce<br />
responses in lower facial muscles, as an electrophysiological<br />
equivalent of the palmomental reflex. 31<br />
Acoustic Blink Reflex. Sound induces a response<br />
in the orbicularis oculi muscle, which may be isolated<br />
and limited to this muscle or involve neck and<br />
extremity muscles as in the generalized auditory<br />
startle reaction. When the response is limited to the<br />
orbicularis oculi, it is known as the auditory blink<br />
reflex. Some authors consider the acoustic blink reflex<br />
the least expression of the generalized startle<br />
response. 99 However, different physiological features<br />
with regard to habituation and latency of the<br />
acoustic blink reflex and the startle reaction have<br />
been described. 18 Specific circuits have been proposed<br />
for the acoustic blink reflex 51 and the startle<br />
reaction. 30 In practical terms, however, if two different<br />
responses are indeed generated by sound stimulation<br />
in the orbicularis oculi muscles, they cannot<br />
be easily differentiated in single individuals in routine<br />
practice. The latency of the orbicularis oculi<br />
response to sound is usually between 40 and 60 ms.<br />
Photic Blink Reflex. Yates and Brown 100 studied<br />
the orbicularis oculi reflex responses evoked by light<br />
stimuli using a photic stimulator. In a control group,<br />
the authors obtained optimal responses of shortest<br />
latency (50.0 ms ± 4.5 ms) with the stimulator held at<br />
a distance of 200 mm in front of the eyes. Afferent<br />
optic fibers probably enter the brainstem in the pretectum<br />
and impulses are then conveyed to the facial<br />
nuclei in the pons. 92 It seems that the cerebral cortex<br />
is not involved in the generation of the photic<br />
blink reflex, as experimental ablation of occipital<br />
cortex does not influence the response. 97 Further<br />
research is required to trace the central circuit mediating<br />
this reflex.<br />
Corneal Reflex. Technique of Recording. During recording<br />
of the corneal reflex responses, the subject<br />
lies supine on a bed or sits in a reclining chair. Responses<br />
are recorded simultaneously from the two<br />
eyes, with surface electrodes positioned as for recording<br />
of the blink reflex responses. The optimal<br />
time to stimulate the cornea is between spontaneous<br />
blinks. The cornea can be stimulated mechanically<br />
or electrically. With mechanical stimulation, orbicularis<br />
oculi responses are evoked by successive manual<br />
application of a small metal sphere, 2 mm in diameter,<br />
to the cornea. 83 The examiner holds the upper<br />
eyelid open with one finger. When the sphere<br />
touches the cornea, contact is made between the<br />
subject and an electronic trigger circuit, which delivers<br />
a pulse. When the corneal reflex is studied by<br />
electrical stimulation, the cornea is touched lightly<br />
with a thin saline-soaked cotton thread connected to<br />
the cathode of a constant-current stimulator. The<br />
anode is placed on the earlobe or forearm. 1 Square<br />
pulses, 1 ms in duration, of 0.1 to 3 mA are delivered<br />
manually, and the oscilloscope is triggered by the<br />
stimulus. Electrical shocks excite the A-delta nerve<br />
fibers directly. To measure the reflex threshold and<br />
for studying the recovery curve with the doubleshock<br />
technique (vide infra), it is necessary to use<br />
electrical stimulation, which provides a controlled<br />
and reproducible stimulus.<br />
Physiology and Normative Data. The corneal reflex<br />
is typically nociceptive and serves to protect the<br />
eye. The cornea is innervated by unmyelinated (C)<br />
and small myelinated (A-delta) fibers. 66 After penetrating<br />
the cornea, the myelinated axons lose myelin<br />
and both types of axons terminate in the stroma<br />
and epithelium as free nerve endings. The mechanical<br />
or electrical stimulation of the cornea gives rise<br />
to a bilateral contraction of the orbicularis oculi,<br />
leading to closure of the eyelids.<br />
Three pairs of latency times should be assessed<br />
from stimulus artifact to onset of the electromyographic<br />
(EMG) response (Fig. 2). In contrast to the<br />
blink reflex, the corneal reflex does not evoke an<br />
early R1 response. When the cornea is touched mechanically,<br />
the latency time of the direct (ipsilateral)<br />
response should not exceed the consensual (contralateral)<br />
response latency by more than 8 ms. The<br />
latencies of the direct responses, evoked by stimulation<br />
of both corneas separately, should never differ<br />
by more than 10 ms. This also applies to the consensual<br />
response latencies. 83 With an electrical stimulus,<br />
the difference between the direct and consensual<br />
responses never exceeds 5 ms, and the difference<br />
between direct responses should never exceed 8 ms.<br />
The reflex threshold in normal subjects rarely exceeds<br />
0.5 mA. 1 Mechanical and electrical stimuli<br />
elicit reflex responses with similar latency times. Absolute<br />
latency values range from 36 ms to 64 ms with<br />
mechanical stimulation and from 35 ms to 50 ms<br />
with electrical stimulation. This wide range of latencies<br />
narrows if control subjects are divided into<br />
groups that take age into account.<br />
Central Pathway. The reflex afferents are A-<br />
delta fibers 25 passing through the long ciliary nerves<br />
and the ophthalmic division of the trigeminal sensory<br />
root to reach the pons. 32,74 The central circuit is<br />
grossly similar to that of the R2 responses of the<br />
blink reflex (Fig. 2). The corneal reflex differs from<br />
R2, however, because it is a purely nociceptive reflex.<br />
The corneal reflex is relayed through different and<br />
fewer interneurons than R2, 84 and it is far more resistant<br />
to suprasegmental influences. 27<br />
16 Brainstem Reflexes MUSCLE & NERVE July 2002
muscle is innervated by the third cranial nerve. The<br />
inhibitory reflex of the LP can be examined together<br />
with the OO excitatory reflex. 8<br />
Technique of Recording. The EMG recordings<br />
from the LP and the OO muscles can be obtained<br />
with the subject supine. To record from the LP, a<br />
bipolar needle electrode is inserted through the skin<br />
in the middle portion of the upper eyelid and directed<br />
toward the LP, while the subject looks downward<br />
and keeps the eyelids gently closed. The subject<br />
is then asked to open the eyes. This maneuver results<br />
in EMG activity from the LP, which can be verified<br />
on the monitor and by the sound signal. To record<br />
from the OO, a bipolar needle electrode is inserted<br />
into the upper or lower eyelids. The position of the<br />
needles is adjusted depending on the response obtained<br />
when the subject blinks or closes the eyes<br />
gently (Fig. 3). Supraorbital nerve stimulation, similar<br />
to that used for eliciting the blink reflex, can be<br />
used in the absence of spontaneous blinking, while<br />
the subject keeps the eyes open voluntarily.<br />
FIGURE 2. Normal corneal reflex. (A) Responses from the right<br />
(r) and left (l) OO muscles after mechanical stimulation of the<br />
right (r*) and (l*) cornea. (B) Presumed central pathways subserving<br />
the corneal reflex. (For key abbreviations, see legend to<br />
Fig. 1.)<br />
Afferent impulses descend along the spinal trigeminal<br />
tract, reach below the obex at the level of<br />
the trigeminal subnucleus caudalis, and ascend<br />
along a multisynaptic chain of interneurons in the<br />
lateral tegmental field before impinging on the facial<br />
motoneurons.<br />
LEVATOR PALPEBRAE INHIBITORY REFLEX<br />
The levator palpebrae superioris (LP) muscle and<br />
the orbicularis oculi (OO) muscle act antagonistically<br />
during various movements of the eyelid. The LP<br />
Physiology and Normative Data. Stimulation of the<br />
supraorbital nerve evokes two silent periods in the<br />
LP muscle 8 (Fig. 4). The first or early silent period is<br />
designated SP1, and the second or late period is SP2.<br />
In contrast to the R1 response of the OO muscle, the<br />
SP1 occurs bilaterally, regardless of the stimulation<br />
site. The latency of SP1 varies from 9 to 13 ms and is<br />
slightly shorter than the latency of the corresponding<br />
R1 response after ipsilateral stimulation. The SP1<br />
has a duration of 12 to 15 ms. Previous experimental<br />
work, including tracing studies, has shown that a<br />
small percentage of the LP motoneurons have axon<br />
collaterals to both LP muscles. 96 Whether these motoneurons<br />
are involved in the generation of SP1 is<br />
unclear. The latency of SP2 varies from 27 to 35 ms<br />
and is again slightly shorter than that of the corresponding<br />
R2 responses. The SP2 has a duration of 32<br />
to 50 ms.<br />
There is a slight variability in the features of the<br />
LP inhibitory reflex, depending on the prestimulus<br />
contraction level of the LP muscle and the stimulus<br />
intensity; when the prestimulus contraction of the<br />
levator is weak, SP1 and SP2 may form a single, large<br />
inhibitory period. At lower stimulus intensities, SP1<br />
may not be evoked. The SP2 latency decreases and<br />
its duration increases following supramaximal stimulation<br />
of the supraorbital nerve.<br />
The antagonistic behavior between OO and LP<br />
muscles can therefore be observed not only during<br />
closure and opening of the eyelids, or during spontaneous<br />
or voluntary blinks, but also during the<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 17
FIGURE 3. Electromyograms from the LP and OO muscles,<br />
showing the reciprocal inhibition between the two muscles in a<br />
healthy subject. (A) When the subject is asked to close the eyes,<br />
LP activity ceases abruptly, followed by contraction of OO. (B)<br />
Note the occurrence of dense bursts of action potentials with high<br />
amplitude preceding the return of LP activity on the order “open<br />
eyes,” following the inhibition of OO. (C) Total inhibition of the LP<br />
muscle activity and a brief contraction of the OO during two spontaneous<br />
blinking (Aramideh et al. 5 ).<br />
evoked blink reflex. Preliminary data indicate that<br />
inhibition of the LP muscle is probably relayed<br />
through central pathways other than those involved<br />
in R1 and R2 responses of the OO muscle. The data<br />
obtained from the examination of the recovery curve<br />
of LP inhibition responses are also in agreement<br />
with this assumption (vide infra).<br />
JAW <strong>REFLEXES</strong><br />
Jaw Jerk. The jaw jerk induced by a tap on the<br />
chin was first described by De Watteville. 34 It is also<br />
called the jaw reflex, mandibular reflex, or masseter<br />
reflex. Without EMG recording, the clinical value of<br />
the mandibular reflex is generally confined to the<br />
distinction between normal and brisk reactions, because<br />
in healthy subjects, the movement of the mandible<br />
is often undetectable. Furthermore, on clinical<br />
examination alone, unilateral interruption of the reflex<br />
arc cannot be detected.<br />
Technique of Recording. To elicit the jaw jerk, the<br />
examiner puts one finger on the subject’s chin and<br />
taps it with a reflex hammer provided with a microswitch<br />
that triggers the sweep of the oscilloscope.<br />
45,80,81 Electromyographic responses are recorded<br />
simultaneously from the two sides by surface<br />
electrodes. The active electrode is placed on the<br />
masseter muscle belly, in the lower third of the distance<br />
between the zygoma and the lower edge of the<br />
mandible, and the reference electrode is placed below<br />
the mandibular angle. Reflex responses can also<br />
be recorded by a small-diameter concentric-needle<br />
electrode inserted into each masseter. In this case, a<br />
ground electrode is taped onto the forehead, neck,<br />
or upper arm. To ensure a constant latency, taps<br />
should be delivered at intervals of 5sormore.<br />
Physiology and Normative Data. The reflex afferents<br />
are Ia fibers from muscle spindles of the jawclosing<br />
muscles. The reflex latency, which provides<br />
the most useful parameter, should be evaluated in<br />
several trials or measured on the averaged signal.<br />
81,101<br />
The mean latency in healthy subjects is 6.8 ms<br />
(SD, 0.8 ms), with a range of 5 to 10 ms 28 (Fig. 5).<br />
Comparison of the latency of the jaw jerk responses,<br />
recorded simultaneously on the two sides, is of great<br />
value. A difference of more than 0.8 ms or a consistent<br />
unilateral absence of the reflex is abnormal.<br />
This reflex is strongly influenced by dental occlusion<br />
and can be asymmetrical or even absent in patients<br />
with temporomandibular disorders. 24 Changing the<br />
position of the mandible or the level of preinnervation<br />
may markedly reduce or worsen the asymmetry<br />
in patients with dental problems but not in patients<br />
with a lesion along the reflex arc. A bilaterally absent<br />
reflex in elderly subjects has no definite clinical significance,<br />
because this may occur in healthy subjects.<br />
Central Pathway. Whether the afferent fibers<br />
travel in the trigeminal motor root 69,87 or the trigeminal<br />
sensory root 41,46,73 is still controversial (Fig. 5).<br />
Unique among the primary sensory neurons, these<br />
afferents have their cell body in the central nervous<br />
system, in the trigeminal mesencephalic nucleus,<br />
rather than in the ganglion. Collaterals from the trigeminal<br />
mesencephalic nucleus descend to the midpons<br />
to activate monosynaptically jaw-closing motoneurons<br />
of the ipsilateral side only.<br />
Masseter Inhibitory Reflex. The masseter inhibitory<br />
reflex (MIR), also called the cutaneous silent<br />
18 Brainstem Reflexes MUSCLE & NERVE July 2002
FIGURE 4. (A) Superimposition of three traces of the right LP muscle (upper traces) and the right OO muscle (lower traces) after<br />
stimulation of the ipsilateral right supraorbital nerve (R*). The ipsilateral stimulation causes an ipsilateral early (SP1) and late (SP2) period<br />
in the LP and an ipsilateral R1 and R2 in the OO. (B) The superimposition of three traces is as in (A), after stimulation of the contralateral<br />
left supraorbital nerve (L*). In contrast to R1 response, regardless of the stimulation site, SP1 could still be evoked (Aramideh et al. 8 ).<br />
period or exteroceptive suppression reflex was first<br />
described by Hoffman and Tonnies 49 as the inhibitory<br />
component of the tongue–jaw reflex seen after<br />
electrical stimulation of the tongue. The EMG silent<br />
period (SP) refers to a transitory relative or absolute<br />
decrease in EMG activity evoked in the midst of an<br />
otherwise sustained contraction. 90<br />
Technique of Recording. The MIR is recorded bilaterally<br />
with the electrodes placed as described for<br />
the jaw jerk. Subjects are seated upright and are instructed<br />
to clench the teeth as hard as possible for a<br />
period of 2–3 s, with the aid of auditory feedback.<br />
The reflex can be measured properly only if the patient<br />
is able to clench the teeth and produce a full<br />
interference pattern in the EMG. It may be necessary<br />
to use a concentric-needle electrode, instead of surface<br />
electrodes, particularly when the signal is contaminated<br />
by facial muscle activity.<br />
Single electrical shocks, 0.2 ms in duration, are<br />
delivered to the mentalis or infraorbital nerves,<br />
through surface electrodes placed over the homonymous<br />
foramina. A stimulus intensity of about 2–3<br />
times the reflex threshold (usually 20–50 mA) yields<br />
the best results. It is always necessary to examine<br />
several trials, usually 8 to 16, allowing 10–30 s of rest<br />
between contractions. Some authors measure the latency<br />
at the last EMG peak, some at the last crossing<br />
of the isoelectric line, and others at the beginning of<br />
the electric silence. Each of these methods is clinically<br />
satisfactory if the same criterion is maintained<br />
and intraindividual differences between right and<br />
left stimulations are examined.<br />
Physiology and Normative Data. Mechanical or<br />
electrical stimulation, applied anywhere within the<br />
mouth or on the facial skin of the maxillary and<br />
mandibular trigeminal divisions, evokes a reflex inhibition<br />
in the jaw-closing muscles. These reflexes<br />
probably play a role in the reflex control of mastication<br />
by preventing intraoral damage that could occur<br />
with uncontrolled contraction of jaw-closing<br />
muscles and in jaw movements during speech.<br />
The MIR consists of two electrical silent periods<br />
interrupting the voluntary EMG activity in the ipsilateral<br />
and contralateral masseter muscles 43,79,81,90<br />
(Fig. 6). The early silent period, SP1, has a latency of<br />
10–15 ms. The late silent period, SP2, has a latency<br />
of 40–50 ms. A latency difference between the ipsilateral<br />
and contralateral responses exceeding 2 ms<br />
for SP1 or 6 ms for SP2 is abnormal.<br />
In a few subjects, little or no EMG activity occurs<br />
between the two SPs, for example, SP1 and SP2<br />
merge in a single long-lasting SP, even when the<br />
strength of contraction is maximal. In this case, the<br />
latency to the resumption of EMG activity is taken as<br />
a measure of SP2. The interside latency difference<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 19
FIGURE 5. (A) Normal jaw-jerk responses from the right (R) and<br />
left (L) masseter muscles. The lower traces are made by averaging,<br />
and arrows mark the latency times. (B) Presumed central<br />
pathways subserving the jaw-jerk responses. (Ophth, ophthalmic<br />
trigeminal root; Max, maxillary trigeminal root; Mand, mandibular<br />
trigeminal root; Mot Root N V, trigeminal motor root; NIII, oculomotor<br />
nerve; N VI= abducens nerve; Ncl Mes N V, mesencephalic<br />
nucleus of the trigeminal nerve; Ncl Mot N V, motor nucleus of<br />
the trigeminal nerve; Ncl Princ N V, principal sensory nucleus of<br />
the trigeminal nerve; Ncl Tract Spin N V, nucleus of the trigeminal<br />
spinal tract.)<br />
FIGURE 6. (A) Normal early (SP1) and late (SP2) phase of the<br />
MIR. The responses are shown from the right (upper trace) and<br />
left (lower trace) masseter muscles after stimulation of the right<br />
(R*) mental nerve. (B) Presumed location of the bulbar interneurons<br />
subserving the SP1 and SP2 of the MIR. (For key abbreviations,<br />
see legend to Fig. 5).<br />
when recording from one muscle should not exceed<br />
8 ms.<br />
If full-wave rectification is available, 8–16 trials<br />
should be averaged. The latency and duration of SPs<br />
can be measured from the intersection of the rectified<br />
and averaged signal and a line indicating 80% of<br />
the background EMG level. In 100 normal subjects<br />
aged 15–80 years, the mean latency of SP1 was 11.8<br />
ms (SD, 0.8) and of SP2 was 45 ms (SD, 5.2). The<br />
duration of SP1 was 20 ms (SD, 4) and the duration<br />
of SP2 was 40 ms (SD, 15). 28<br />
Probably because electrical stimuli yield a mixed<br />
nociceptive and nonnociceptive input, whether the<br />
SP1, SP2, or both components are nociceptive reflexes<br />
remains controversial. 37,70 Both inhibitory responses<br />
can nevertheless be elicited with innocuous<br />
mechanical stimuli, and indirect evidence supports<br />
the view that the afferents belong to the intermediately<br />
myelinated A beta group. 22,89<br />
Central Pathway. After stimulation of the mental<br />
or infraorbital nerve, impulses reach the pons<br />
through the sensory mandibular or maxillary root of<br />
the trigeminal nerve, respectively 81 (Fig. 6). The SP1<br />
20 Brainstem Reflexes MUSCLE & NERVE July 2002
esponse is probably mediated by one inhibitory interneuron,<br />
located close to the ipsilateral trigeminal<br />
motor nucleus. The inhibitory interneuron projects<br />
onto jaw-closing motoneurons bilaterally. The whole<br />
circuit lies in the midpons. 79 The afferents for SP2<br />
descend in the spinal trigeminal tract and connect<br />
with a polysynaptic chain of excitatory interneurons,<br />
probably located in the lateral reticular formation,<br />
at the level of the pontomedullary junction. The<br />
last interneuron of the chain is inhibitory and<br />
gives rise to ipsilateral and contralateral collaterals<br />
that ascend medial to the right and left spinal trigeminal<br />
complexes to reach the trigeminal motoneurons.<br />
79<br />
Corneomandibular Reflex. The trigemino–<br />
trigeminal corneomandibular reflex is elicited clinically<br />
by touching the cornea with a dry wisp of cotton<br />
wool. 47,48 The reflex response is a slight protrusion<br />
and contralateral deviation of the mandible due to<br />
contraction of the inferior head of the lateral pterygoid<br />
muscle. The corneomandibular reflex must not<br />
be confused with the trigeminofacial corneomental<br />
reflex. 10,98 This latter response, seen as a subtle<br />
movement of the skin over the chin caused by contraction<br />
of the mental muscle, occurs in many<br />
healthy subjects. Electromyographic investigation<br />
has demonstrated that the corneomandibular reflex<br />
is absent in healthy subjects and can be recorded in<br />
patients with corticobulbar tract lesions. 77<br />
Technique of Recording. For EMG recording, the<br />
cornea is touched with a 2-mm–diameter metal<br />
sphere, connected to an electronic trigger circuit,<br />
identical to the arrangement used for corneal reflex<br />
response recordings. 77 The lateral inferior pterygoid<br />
muscle can be studied best with a unipolar wire electrode.<br />
This is composed of a fine Teflon-coated wire,<br />
0.1 mm in diameter, threaded into the tip of a 4-cm<br />
disposable needle. The needle is positioned in the<br />
mandibular notch, just in front of the condylar head<br />
and about 1 cm below the zygomatic arch, and is<br />
then placed approximately perpendicular to the sagittal<br />
plane and advanced to a depth of about 4 cm.<br />
Gentle removal of the needle leaves the wire electrode<br />
in place. Its free end is connected to a preamplifier<br />
lead through a tightly coiled steel spring. An<br />
inactive surface electrode is located over the posterior<br />
zygoma. Pterygoid electrode placement can be<br />
checked by recording EMG activity during downward<br />
and contralateral mandible movement. A pair<br />
of surface electrodes placed ipsilaterally over the<br />
lateral half of the chin will allow simultaneous examination<br />
of reflex discharges in the mentalis<br />
muscle.<br />
Latency and Central Pathway of Responses. After<br />
mechanical stimulation of the cornea, the average<br />
latency of the EMG response (Fig. 7) in the lateral<br />
inferior pterygoid muscle is 73.3 ms (SD, 7.4), and<br />
the interside difference is 5 ms (range 0–12 ms). 77<br />
The long latency suggests multiple intramedullary<br />
synaptic connections. Afferent impulses for the corneomandibular<br />
reflex and afferent impulses for the<br />
corneal reflex pass along similar fibers, whereas ascending<br />
trigemino–trigeminal interneuronal connections<br />
probably run in the bulbar lateral reticular<br />
formation. Efferent impulses to the lateral inferior<br />
pterygoid muscle are mediated through the trigeminal<br />
motor root.<br />
FIGURE 7. Example of the corneomandibular reflex responses.<br />
Upper two traces show responses from the right (r) and left (l)<br />
inferior head of the lateral pterygoid muscle obtained by stimulation<br />
of the right (r*) cornea. The lower two traces show the<br />
responses evoked by stimulation of the left (l*) cornea.<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 21
INTEGRATIVE FUNCTIONS OF THE <strong>BRAINSTEM</strong><br />
Recovery Curves to Paired Stimuli. Because of passive<br />
mechanisms (e.g., afterhyperpolarization potential)<br />
or the intervention of negative feedback circuits,<br />
the excitability of a reflex circuit is depressed<br />
after the passage of an earlier impulse. With the<br />
double-shock technique, it is possible to draw the<br />
recovery curve (or excitability cycle) of a given reflex<br />
and thus obtain a measure of the excitability of the<br />
reflex circuit. 55<br />
Stimulus intensity and position of the stimulating<br />
and recording electrodes are the same as used in<br />
standard reflex studies. Electrical stimuli of equal<br />
intensity are delivered in pairs, at varying interstimulus<br />
intervals. The first shock is called the “conditioning”<br />
stimulus, and the second shock is the “test”<br />
shock. The size (amplitude, duration, or area) of<br />
the conditioning and test responses are measured,<br />
and that of the test response is expressed as a percentage<br />
of the conditioning response. The recovery<br />
curve is drawn by plotting the size of the test response,<br />
as a percentage of the conditioning response,<br />
on the y-axis and the time-interval on the<br />
x-axis 55 (Fig. 8).<br />
Recovery of Orbicularis Oculi Reflexes. A complete<br />
excitability cycle of the orbicularis oculi reflex can be<br />
examined with 10-ms time intervals between 10 ms<br />
and 100 ms, and 100-ms intervals between 100 ms<br />
and 1500 ms. However, it is not clinically necessary to<br />
check all these intervals.<br />
The test R1 summates with the conditioning R1<br />
or R2 at short (up to 60–70 ms) interstimulus intervals.<br />
The apparent facilitation may reach 250% at<br />
30–40-ms intervals. With longer intervals, R1 is affected<br />
little by the conditioning shock. It may be<br />
slightly reduced (80% at the 100-ms interval) and<br />
slowly recovers to 90–100% of the conditioning response<br />
at intervals of 200–500 ms. 55<br />
Test R2 is usually completely abolished at interstimulus<br />
intervals shorter than 200 ms; it then slowly<br />
recovers, reaching about 40–50% at the 500-ms<br />
interval and 70–90% at the 1500-ms interval 3,35<br />
(Fig. 8).<br />
The recovery of the corneal reflex parallels but is<br />
more rapid than that of R2. The test corneal reflex<br />
already measures about 30% at the 200-ms interval,<br />
whereas R2 of the blink reflex is still abolished, and<br />
reaches 90–100% at the 1500-ms interval. 20,55<br />
As the same motoneurons are shared by the various<br />
orbicularis oculi reflexes, the difference in recovery<br />
times (progressively longer for R1, corneal<br />
reflex, and R2) is commonly attributed to differences<br />
in the interneuronal net. The R2 of the blink<br />
FIGURE 8. Recovery curve of the R2 response of the blink reflex.<br />
Rectified and averaged (n = 6) EMG responses are presented at<br />
intervals from 220 ms to 10 s between conditioning and test<br />
stimuli, in a control subject (A) and in a patient with blepharospasm<br />
(B). (C) Complete recovery curves for both subjects. The<br />
patient (B) shows significantly less suppression at intervals<br />
smallerthan1s(S1,conditioning stimulus; S2, test stimulus).<br />
reflex response is most susceptible to changes in excitability,<br />
and the R2 recovery curve has provided<br />
valuable information in research and clinical settings.<br />
It may also be valuable to measure the recovery<br />
index. 3,35<br />
22 Brainstem Reflexes MUSCLE & NERVE July 2002
Recovery of Levator Palpebrae Inhibitory Reflex.<br />
With the recording needle positioned as for<br />
recording of the levator palpebrae EMG activity and<br />
the inhibition reflex (see earlier), the recovery of the<br />
inhibition periods of the levator palpebrae muscle<br />
can be examined with the recovery curve of the orbicularis<br />
oculi responses 8 (Fig. 9). The durations of<br />
the two silent periods are measured, and that of the<br />
test response is expressed as a percentage of the conditioning<br />
response. The recovery curve is drawn by<br />
plotting the size of the test response, as a percentage<br />
of the conditioning response, on the y-axis and the<br />
time-interval on the x-axis.<br />
At interstimulus intervals higher than 500 ms, the<br />
percentage of inhibition recovery of the second silent<br />
period (SP2) is similar to that of the excitability<br />
recovery of the R2 response (Fig. 9). At lower intervals,<br />
the recovery curve of SP2 is shifted upward, i.e.,<br />
SP2 recovers faster than the corresponding R2 response.<br />
For example, at 200 ms where the R2 response<br />
is completely abolished, the SP2 could still be<br />
recruited at a level of about 20–30%. These findings<br />
are in accord with our earlier hypothesis that responses<br />
are probably relayed on different central<br />
pathways.<br />
Recovery of Masseter Inhibitory Reflex. The recovery<br />
cycle of the MIR is studied by delivering paired<br />
stimuli at interstimulus intervals of 100 ms, 150 ms,<br />
250 ms, and 500 ms, with the same low-rate stimulation<br />
and alternation of “clench” and “rest” phases<br />
described for the assessment of the reflex values.<br />
The recovery curve is drawn by plotting the timeintervals<br />
on the x-axis and the size (area or duration)<br />
of the test response as a percentage of the size of the<br />
conditioning on the y-axis (Fig. 10).<br />
The recovery of SP1 in normal subjects varies<br />
from about 85% at 100-ms intervals to approximately<br />
96% at 500 ms. The recovery of SP2 varies from 24%<br />
at 100 ms to 79% at 500 ms. The function of correlation<br />
between time interval (milliseconds) and size<br />
of the test response (percent) is linear for SP1 (y =<br />
0.02 ×+ 85) and logarithmic in base 10 for SP2 (y =<br />
75 log ×− 120). 29<br />
Recovery can also be evaluated by simply measuring<br />
the duration of SP1 and SP2 in nonrectified recordings,<br />
and for clinical use, it may be sufficient to<br />
measure the recovery of SP2 at the 250-ms interval.<br />
24,28<br />
CLINICAL APPLICATIONS<br />
Trigeminal Neuropathy. For diagnosing extra-axial<br />
trigeminal nerve lesions, the short-latency responses,<br />
such as R1 of the orbicularis oculi muscle, SP1 of the<br />
MIR, and the jaw jerk, are far more sensitive than are<br />
FIGURE 9. (A) Recovery curve of SP2 of the LP (L. Palpebrae)<br />
and (B) recovery curve of the R2 response of the OO (O. Oculi).<br />
(C) Recovery curves of both muscles together. At higher stimulus<br />
intervals, e.g., 1 s and 0.5 s, the percentage of inhibition recovery<br />
of the SP2 was similar to that of the excitability recovery of the R2<br />
response. At lower stimulus intervals, the recovery curve of inhibition<br />
responses were shifted upward, i.e., SP2 recovered faster<br />
than did corresponding R2 response; at 200 ms, where R2 response<br />
did not show any recovery, the SP2 could still be recorded<br />
for about 20–30 %. The SP1 is not examined systematically<br />
(Aramideh et al. 8 ).<br />
the long-latency responses, such as R2 of the blink<br />
reflex and SP2 of the MIR. One reason is that they<br />
are supplied by fewer reflex afferents. In addition,<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 23
they exhibit less variability and have a smaller normal<br />
range than do polysynaptic responses. 9,57,78<br />
The blink reflex may be abnormal, with lesions of<br />
the supraorbital nerve branch or more proximal lesions<br />
affecting the ophthalmic division of the trigeminal<br />
nerve. An abnormal corneal reflex can reflect<br />
damage to the long ciliary nerves or the ophthalmic<br />
division where ciliary nerves join the ophthalmic<br />
root. Blink and corneal reflexes are not necessarily<br />
both affected, because they are mediated by different<br />
sets of afferents and different central circuits.<br />
11,75 Furthermore, the corneal reflex is more<br />
sensitive, because it is mediated by fewer afferents<br />
than is the blink reflex. In lesions of the infraorbital<br />
nerve or, more proximally, of the maxillary root, the<br />
blink reflex and the MIR may be abnormal after infraorbital<br />
nerve stimulation. Damage to the mental<br />
nerve or the trigeminal mandibular root may cause<br />
MIR abnormalities.<br />
To localize the site of lesion, it is helpful to study<br />
trigeminal reflexes evoked from all three divisions.<br />
Abnormalities in all divisions of the trigeminal nerve<br />
indicate a trigeminal root lesion in the middle or<br />
posterior cranial fossa.<br />
As a general rule, peripheral lesions are more<br />
likely to affect both blink reflex components to a<br />
similar degree (Fig. 11, type B) or more clearly affect<br />
R1 than R2. It is extremely rare to see absence or<br />
delay of R2 without accompanying abnormalities of<br />
R1 in peripheral lesions. By contrast, intra-axial lesions<br />
often affect R1 and R2 separately. Very discrete<br />
lesions limited to the upper pons may cause a delay<br />
or loss of the R1 component without accompanying<br />
R2 response abnormalities 56 (Fig. 11, type A). The<br />
most common finding with intra-axial involvement<br />
of the trigeminal sensory system, such as in multiple<br />
sclerosis or in olivopontocerebellar atrophy, is of an<br />
abnormal R2 response with normal R1 response.<br />
FIGURE 10. Recovery curves of the MIR. (A) Eight rectified and<br />
averaged signals, recorded in a healthy subject after stimulation<br />
of the mental nerve. The first (conditioning) shock is indicated by<br />
the dashed line. The second (test) shock is indicated by the arrows.<br />
After a second shock with an interstimulus interval of 100<br />
ms, the test SP2 is almost abolished (A1) and partly recovers with<br />
an interval of 250 ms (A2). (B) The same as in (A) but in a patient<br />
with Parkinson’s disease. The test SP2 is only slightly suppressed<br />
at the interstimulus interval of 100 ms (B1) and completely<br />
recovers at the interval of 250 ms (B2). (C) Recovery<br />
curve of the SP2 component of the MIR. Note: x-axis, interstimulus<br />
interval (ms); y-axis, area of the test response expressed as<br />
percentage of the conditioning response. The two curves are ±<br />
standard errors of the estimate in 20 healthy subjects. The two<br />
squares indicate the recovery value for the 100-ms and 250-ms<br />
intervals in (B). Note that the recovery of SP2 is enhanced in the<br />
patient with Parkinson’s disease.<br />
Trigeminal Pain and Neuralgia. In patients with<br />
pain in the trigeminal territory, neurophysiological<br />
testing of trigeminal function offers the clinician<br />
useful information. Abnormalities are often disclosed<br />
in divisions that appear clinically unaffected.<br />
An objective demonstration of dysfunction is provided<br />
in all patients with pain secondary to a documented<br />
disease, such as symptomatic trigeminal<br />
neuralgia, postherpetic neuralgia, vascular malformations,<br />
benign tumors of the cerebellopontine<br />
angle, and multiple sclerosis, even in those patients<br />
who have no clinical signs or complaints other than<br />
pain. 26,60,78<br />
Reflex responses are more affected in patients<br />
with constant pain than in those with paroxysmal<br />
24 Brainstem Reflexes MUSCLE & NERVE July 2002
FIGURE 11. (A) Schematic representation of various lesions within the brainstem (A-E) and corresponding blink reflex response<br />
abnormalities in the right (R) and left (L) OO muscles after stimulation (*) of the supraorbital nerves (B). Blink reflex responses are either<br />
delayed (left column) or absent (right column). See text for comments on different types of reflex abnormalities. (VII, facial nucleus; VI,<br />
abducens nucleus; Vpr, principal trigeminal nucleus; Vmot, trigeminal motor nucleus; Lat. tegm. field, lateral tegmental field; Med. tegm.<br />
field, medial tegmental field) (Aramideh et al. 6 ).<br />
pain. This agrees with the common notion that a<br />
dysfunction of few fibers provokes paroxysmal pain,<br />
whereas severe damage does not. Indeed, neuralgic<br />
pain is often relieved by surgical deafferentation,<br />
whereas constant pain is often worsened. In symptomatic<br />
trigeminal pains, the trigeminal reflexes<br />
have a very high sensitivity, probably because they<br />
allow examination of all three divisions. The most<br />
sensitive reflexes are the R1 of the blink reflex and<br />
the SP1 of the MIR. 26 Mild reflex abnormalities occur<br />
occasionally, 60,81 but in most patients with idiopathic<br />
trigeminal neuralgia (“tic douloureux”), all<br />
reflexes are normal. In patients with idiopathic trigeminal<br />
neuralgia, the presynaptic waves of the scalp<br />
evoked potential after percutaneous infraorbital<br />
stimulation are more sensitive than are reflex responses<br />
64 and in about half of the patients disclose<br />
abnormalities of the waves originating near the root<br />
entry into the pons. 63 The finding of any abnormality<br />
should nonetheless promote further investigation.<br />
The most commonly reported causes of symptomatic<br />
neuralgia are benign tumors of the<br />
cerebellopontine angle and vascular anomalies in<br />
the posterior fossa impinging on the proximal portion<br />
of the trigeminal root, and multiple sclerosis<br />
with a plaque in the root entry zone. 88 As in neuralgia<br />
secondary to well-documented lesions, the most<br />
likely site of conduction impairment in idiopathic<br />
trigeminal neuralgia is the region of the root entry<br />
into the pons. 26,63<br />
Facial Neuropathy. Recording the blink reflex,<br />
whose reflex arc includes the entire facial nerve, may<br />
provide information right from the onset of the<br />
palsy, although it has no prognostic value. The R1<br />
and R2 components are abnormal ipsilaterally to the<br />
affected side, regardless of the side of stimulation<br />
(Fig. 11, type C). Although most patients have a complete<br />
absence of responses, some have a delayed response<br />
or a response of reduced amplitude. The latter<br />
findings, or the reappearance of previously<br />
absent responses, indicate a conduction defect without<br />
substantial axonal loss, from which the patient<br />
will recover either completely or almost completely.<br />
It is common to observe an increased blink rate<br />
in patients with facial palsy. Pastor et al. 86 reported<br />
enhanced blink reflex excitability recovery curves in<br />
two patients examined within the first month after<br />
onset of a Bell’s palsy. This finding was later confirmed<br />
by Syed et al., 91 suggesting that plastic<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 25
changes may take place in the central nervous system<br />
in an attempt to compensate for the eyelid weakness.<br />
In patients without distal degeneration, the latency<br />
of R1 is usually delayed by a few milliseconds (2 ms<br />
in the series reported by Kimura et al. 59 ), and returns<br />
to normal in 2 to 4 months.<br />
In patients with substantial degeneration, R1 is<br />
absent and the direct motor response markedly reduced<br />
in amplitude for several months or longer.<br />
Eekhof et al. 36 recorded ephaptic transmission in<br />
50% of their patients who developed facial synkinesis<br />
after Bell’s palsy and suggested that there may be<br />
some alteration in excitability of the facial nucleus.<br />
Cranial Nerve Involvement in Polyneuropathies.<br />
Generalized polyneuropathies may induce<br />
bilateral abnormalities of the trigeminal reflexes. 65<br />
Kimura 54 has studied the blink reflex in a large series<br />
of patients with polyneuropathy. In patients with Sjögren’s<br />
neuronopathy, Valls-Solé et al. 95 found severely<br />
affected blink reflex and MIR, whereas the jaw<br />
jerk was spared. The masseter silent period after<br />
chin taps (tap-SP) tends to be delayed in patients<br />
with demyelinating neuropathies and normal in patients<br />
with axonopathies of various origin. Patients<br />
with chronic inflammatory demyelinating polyneuropathy<br />
or severe diabetic polyneuropathy often<br />
have subclinical trigeminal dysfunction. 21 This is<br />
best disclosed by demonstrating a delay of the first<br />
silent period SP1 of the MIR after mental nerve<br />
stimulation.<br />
Oculomotor, trigeminal, or facial nerve involvement<br />
may be a mononeuropathic expression of a<br />
systemic disorder. The trigeminal and facial nerves<br />
may be involved in patients with Guillain–Barré syndrome.<br />
Brainstem Lesions. Lesions affecting the mesencephalon,<br />
pons, or medulla cause different abnormalities,<br />
which may be revealed by neurophysiological<br />
examination of brainstem reflexes and functions.<br />
Changes in jaw jerk, blink reflex, light-evoked blink,<br />
and corneal reflex have been reported in multiple<br />
sclerosis. 78 Kimura 56 analyzed the blink reflex obtained<br />
from 260 patients with suspected multiple<br />
sclerosis. The R1 response of the blink reflex was<br />
delayed on one or both sides in 96 of 145 patients<br />
with a definite diagnosis (66%), 32 of 57 with probable<br />
multiple sclerosis (56%), and 17 of 58 with possible<br />
disease (29%). When the reflex was analyzed<br />
according to clinical localization of the lesion in the<br />
260 patients, R1 was abnormal in 49 of 63 patients<br />
with pontine signs (78%) and 59 of 104 with other<br />
brainstem signs (57%). Kimura 56 also found a delayed<br />
or absent R1 in 40% of patients in the absence<br />
of clinical signs of brainstem damage. Alteration of<br />
R2 was less specific. A combination of trigeminal reflex<br />
abnormalities, in particular an abnormal jaw<br />
jerk accompanied by a disorder of one of the other<br />
reflexes, reflects damage to different levels of the<br />
trigeminal system and may therefore make an important<br />
contribution to the diagnosis of multiple sclerosis.<br />
The finding of an abnormal jaw jerk with normal<br />
masseteric EMG may reflect a midbrain lesion involving<br />
structures adjacent to the aqueduct. 73,81 Abnormal<br />
jaw jerks have been found ipsilateral to midbrain<br />
lesions. 45,52 These observations have now been verified<br />
neuroanatomically in midbrain lesions involving<br />
the mesencephalic tract and nucleus of the trigeminal<br />
nerve and sparing the trigeminal motor nucleus<br />
and fibers in the pons. 73<br />
Lesions affecting the lower pons or the dorsolateral<br />
medulla oblongata, or both, cause several types<br />
of blink reflex abnormality, as shown in Figure 11.<br />
The figure may serve as a guide to relate a specific<br />
abnormality to the location of the causal lesion in<br />
the central reflex arc. In general, all the abnormal<br />
R2 features occurring in the blink reflex also occur<br />
in corneal reflex responses.<br />
Wallenberg’s syndrome is commonly associated<br />
with an abnormality of the corneal reflex and R2 of<br />
the blink reflex, whereas R1 is spared. 58,74,75,82 In<br />
most patients, an afferent type of reflex abnormality<br />
is present (Fig. 11, type B2).<br />
In predicting MRI results in patients with symptoms<br />
and signs related to classic trigeminal nerve<br />
dysfunction, Majoie et al. 67 showed that reflex studies<br />
yielded a sensitivity of 100%, a specificity of 81%,<br />
a positive predictive value of 57%, and a negative<br />
predictive value of 100%. However, the authors emphasized<br />
that further investigations in larger group<br />
of patients with different signs and symptoms related<br />
to trigeminal dysfunction are required.<br />
Hemispheric Lesions. Ischemic or hemorrhagic lesions<br />
or tumors in the cerebral hemispheres may<br />
alter some components of the corneal reflex and<br />
MIR responses. 23,61,75,76 Studying patients in the<br />
early phase after a stroke, Fisher et al. 42 reported<br />
delayed R1 responses, which subsequently returned<br />
to normal. During chronic states, however, changes<br />
in R2 may persist for several weeks or even longer. In<br />
hemispheric disorders, corneal and late blink reflex<br />
responses may be absent or diminished bilaterally<br />
when the affected side of the face is stimulated (similar<br />
to type B2 in Fig. 11). Stimulation of the normal<br />
side often reveals an additional absence or diminu-<br />
26 Brainstem Reflexes MUSCLE & NERVE July 2002
tion of the consensual response (similar to type D in<br />
Fig. 11). Because the polysynaptic R2 is more profoundly<br />
inhibited than is the oligosynaptic R1, interruption<br />
of corticobulbar pathways to the reflex system<br />
is more likely to result in diminished facilitation<br />
of interneurons. The descending facilitatory influence<br />
on the bulbar pathway itself probably originates<br />
in wide areas of the cortex, but the most common<br />
site of origin is the lower postcentral area, which<br />
corresponds to the sensory representation of the<br />
face. 61,76 By contrast, in chronic pyramidal tract lesions,<br />
the R1 response may be slightly facilitated on<br />
the paretic side. This facilitation is explained by removal<br />
of corticobulbar inhibitory influences on facial<br />
motoneurons as they impinge on spinal motoneurons.<br />
Extrapyramidal Disorders. In extrapyramidal disorders,<br />
facial reflexes with short latencies (jaw jerk, R1<br />
of the blink reflex, and SP1 of the MIR) are unaltered.<br />
This observation indicates that the afferent<br />
and efferent fibers of the reflex arc and the brainstem<br />
monosynaptic or oligosynaptic circuits are not<br />
directly affected by these diseases. In contrast, reflexes<br />
with longer latencies and polysynaptic pathways,<br />
which are subject to strong suprasegmental influence,<br />
are often altered due to a change in the<br />
excitability of the interneuronal pool.<br />
Patients with Parkinson’s disease often show an<br />
enhanced excitability of brainstem interneurons that<br />
leads to a rapid recovery of the blink reflex responses.<br />
55 Similar abnormalities have been described<br />
in the excitability recovery curve of the<br />
MIR 29 (Fig. 10).<br />
In Huntington’s disease, R2 shows an increased<br />
latency and enhanced habituation. 2,16,39,69 In contrast,<br />
the MIR, including recovery curves of SP1 and<br />
SP2, is normal. 16,29<br />
Eyelid Movement Disorders. Eyelid kinematics are<br />
best investigated using electromagnetic recordings.<br />
17,19,40 Furthermore, synchronous EMG recording<br />
from the levator palpebrae and the orbicularis<br />
oculi muscles provides valuable information on possible<br />
disturbances of the reciprocal activity between<br />
these two muscles in various eyelid movement abnormalities.<br />
5<br />
Blepharospasm. Blepharospasm is a focal dystonia<br />
of the eyelids 68 characterized by tremulous, phasic,<br />
or clonic discharges in the orbicularis oculi. The<br />
antagonistic activity between the orbicularis oculi<br />
and the levator palpebrae muscles is disturbed in<br />
some patients, and a minority of patients also have<br />
involuntary levator palpebrae inhibition (vide infra).<br />
Although in some patients with blepharospasm, the<br />
R2 response is prolonged, 12 the reflex data are usually<br />
normal. 33,35 Patients with blepharospasm have<br />
abnormal enhancement of brainstem interneuronal<br />
excitability, as shown by recovery curves of the R2<br />
response (Fig. 8), similar to that found in patients<br />
with parkinsonism. 3,12,29,93 However, the pathophysiology<br />
underlying such abnormality may be different<br />
in the two disorders. In a group of 33 patients with<br />
involuntary eyelid closure, Aramideh et al. 3 showed<br />
that recovery of R2 was enhanced in all patients with<br />
pure blepharospasm. The exact pathophysiology of<br />
dystonia is unknown (see Berardelli et al. 13 for a<br />
review).<br />
Apraxia of Eyelid Opening. Patients with apraxia<br />
of eyelid opening, also known as involuntary levator<br />
palpebrae inhibition, have difficulty in initiating the<br />
act of lid opening on command. 15,44 Many patients<br />
also exhibit an inability to keep the eyelids open for<br />
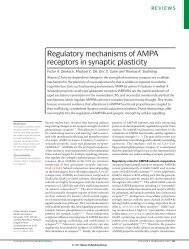
FIGURE 12. An EMG recording in a patient with involuntary levator<br />
palpebrae inhibition (apraxia of eyelid opening) and blepharospasm.<br />
(A) The patient shows involuntary inhibition periods<br />
(IIPs) of the LP muscle, causing drooping of the eyelids and<br />
periods of suppression of LP activity resulting in inability to open<br />
the eyelids voluntarily on the command “open eyes.” (B) Dense<br />
burst of phasic discharges during spasms of the OO muscle are<br />
accompanied by inhibition of LP activity (Aramideh et al. 8 ).<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 27
a long period of time (Fig. 12). Apraxia of eyelid<br />
opening may accompany blepharospasm. Synchronous<br />
needle EMG recording from the levator palpebrae<br />
and the orbicularis oculi muscles reveals involuntary<br />
inhibition of the levator palpebrae muscle<br />
activity causing inability to keep the eyelids open or<br />
to reopen them after involuntary closure of the lids. 5<br />
The blink-reflex–excitability recovery curve is normal<br />
in these patients. 3<br />
Orbicularis Oculi Motor Persistence. Involuntary<br />
levator palpebrae inhibition should be differentiated<br />
from “motor persistence of the orbicularis oculi”<br />
muscle. 4,7 Following voluntary closure of the eyelids<br />
on command (Fig. 13), the patients with the latter<br />
abnormality are also unable to open the lids on command.<br />
However, needle EMG recording shows that<br />
these patients are unable to suppress the activity of<br />
the orbicularis oculi muscle. 7<br />
FIGURE 13. Orbicularis oculi motor persistence. The EMG recording<br />
shows that after voluntary closure of the eyelid and upon<br />
the command to “open eyes,” patient is unable to suppress the<br />
contraction of the OO. After about 1 s, the density of the bursts of<br />
action potentials in the orbicularis gradually begins to diminish<br />
and is accompanied by an increase in intensity and frequency of<br />
the discharges in the LP. The eyelid opens when the orbicularis<br />
muscle activity is almost completely inhibited (at open arrow)<br />
(Aramideh et al. 7 ).<br />
REFERENCES<br />
1. Accornero N, Berardelli A, Bini G, Cruccu G, Manfredi M.<br />
Corneal reflex elicited by electrical stimulation of the human<br />
cornea. Neurology 1980;30:782–785.<br />
2. Agostino R, Berardelli A, Cruccu G, Pauletti G, Stocchi F,<br />
Manfredi M. Correlation between facial involuntary movements<br />
and abnormalities of blink and corneal reflexes in<br />
Huntington’s chorea. J Neurol Neurosurg Psychiatry 1988;<br />
3:281–289.<br />
3. Aramideh M, Eekhof JLA, Bour LJ, Koelman JHTM, Speelman<br />
JD, Ongerboer de Visser BW. Electromyography and<br />
blink reflex recovery in involuntary eyelid closure: a comparative<br />
study. J Neurol Neurosurg Psychiatry 1995;58:<br />
692–698.<br />
4. Aramideh M, Koelman JHTM, Speelman JD, Ongerboer de<br />
Visser BW. Eyelid movement disorders and electromyography.<br />
Lancet 2001;357:805–806.<br />
5. Aramideh M, Ongerboer de Visser BW, Devriese PP, Bour<br />
LJ, Speelman JD. Electromyographic features of levator palpebrae<br />
superioris and orbicularis oculi muscles in blepharospasm.<br />
Brain 1994;117:27–38.<br />
6. Aramideh M, Ongerboer de Visser BW, Koelman JHTM, Majoie<br />
CB, Holstege G. The late blink reflex abnormality due to<br />
lesions of the lateral tegmental field. Brain 1997;120:<br />
1685–1692.<br />
7. Aramideh M, Ongerboer de Visser BW, Koelman JHTM,<br />
Speelman JD. Motor persistence of orbicularis oculi muscle<br />
in eyelid opening disorders. Neurology 1995;45:897–902.<br />
8. Aramideh M, Valls-Solé J, Cruccu G, Ongerboer de Visser<br />
BW. Cranial nerves and brain stem reflexes: electrodiagnostic<br />
techniques, physiology and normative data. In: Brown<br />
WF, Bolton CF, Aminoff MJ, editors. Neuromuscular function<br />
and disease. Philadephia: WB Saunders; 2002. p<br />
433–454.<br />
9. Auger RG, McManis PG. Trigeminal sensory neuropathy associated<br />
with decreased oral sensation and impairment of<br />
the masseter inhibitory reflex. Neurology 1990;40:759–763.<br />
10. Benedek L, Von Angyal L. Ueber die Palmomentalen und<br />
corneomentalen Reflexe. Z Neurol Psychiat 1941;172:<br />
632–638.<br />
11. Berardelli A, Cruccu G, Manfredi M, Rothwell JC, Day BL,<br />
Marsden CD. The corneal reflex and R2 component of the<br />
blink reflex. Neurology 1985;35:797–801.<br />
12. Berardelli A, Rothwell JC, Day BL, Marsden CD. Pathophysiology<br />
of blepharospasm and oromandibular dystonia. Brain<br />
1985;108:593–609.<br />
13. Berardelli A, Rothwell JC, Hallett M, Thompson PD, Manfredi<br />
M, Marsden CD. Pathophysiology of primary dystonia.<br />
Brain 1998;121:1195–1212.<br />
14. Boelhouwer AJW, Brunia CHM. Blink reflexes and the state<br />
of arousal. J Neurol Neurosurg Psychiatry 1977;40:58–63.<br />
15. Boghen D. Apraxia of lid opening: a review. Neurology 1997;<br />
48:1491–1503.<br />
16. Bollen E, Arts R, Roos R, van der Velde EA, Buruma OJ.<br />
Brainstem reflexes and brainstem auditory evoked responses<br />
28 Brainstem Reflexes MUSCLE & NERVE July 2002
in Huntington’s chorea. J Neurol Neurosurg Psychiatry<br />
1986;49:313–315.<br />
17. Bour LJ, Aramideh M, Ongerboer de Visser BW. Neurophysiological<br />
aspects of eye and eyelid movements during<br />
blinking in man. J Neurophysiol 2000;83:166–176.<br />
18. Brown P, Rothwell JC, Thompson PD, Britton TC, Day BL,<br />
Marsden CD. New observations on the normal auditory<br />
startle reflex in man. Brain 1991;11:1891–1902.<br />
19. Collewijn H, Van Der Steen J, Steinman RM. Human eye<br />
movements associated with blinks and prolonged eyelid closure.<br />
J Neurophysiol 1985;54:11–27.<br />
20. Cruccu G, Agostino R, Berardelli A, Manfredi M. Excitability<br />
of the corneal reflex in man. Neurosci Lett 1986;63:320–324.<br />
21. Cruccu G, Agostino R, Inghilleri M, Innocenti P, Romaniello<br />
A, Manfredi M. Mandibular nerve involvement in diabetic<br />
polyneuropathy and chronic inflammatory demyelinating<br />
polyneuropathy. Muscle Nerve 1998;21:1673–1679.<br />
22. Cruccu G, Agostino R, Inghilleri M, Manfredi M, Ongerboer<br />
de Visser BW. The masseter inhibitory reflex is evoked by<br />
innocuous stimuli and mediated by A beta afferent fibers.<br />
Exp Brain Res 1989;77:447–450.<br />
23. Cruccu G, Fornarelli M, Manfredi M. Impairment of masticatory<br />
function in hemiplegia. Neurology 1988;38:301–306.<br />
24. Cruccu G, Frisardi G, Pauletti G, Romaniello A, Manfredi M.<br />
Excitability of the central masticatory pathways in patients<br />
with painful temporomandibular disorders. Pain 1997;73:<br />
447–454.<br />
25. Cruccu G, Inghilleri M, Fraioli B, Guidetti B, Manfredi M.<br />
Neurophysiological assessment of trigeminal function after<br />
surgery for trigeminal neuralgia. Neurology 1987;37:<br />
631–638.<br />
26. Cruccu G, Leandri M, Feliciani M, Manfredi M. Idiopathic<br />
and symptomatic trigeminal pain. J Neurol Neurosurg Psychiatry<br />
1990;53: 1034–1042.<br />
27. Cruccu G, Leandri MG, Ferracuti S, Manfredi M. Corneal<br />
reflex responses to mechanical and electrical stimuli in<br />
coma and narcotic analgesia in humans. Neurosci Lett 1997;<br />
222:33–36.<br />
28. Cruccu G, Ongerboer de Visser BW. The jaw reflexes. In:<br />
Deuschl G, Eisen A, editors. Recommendations for the practice<br />
of clinical neurophysiology: guidlines of the International<br />
Federation of Clinical Neurophysiology. Amsterdam:<br />
Elsevier Science; 1999. p 243–247.<br />
29. Cruccu G, Pauletti G, Agostino R, Berardelli A, Manfredi M.<br />
Masseter inhibitory reflex in movement disorders. Huntington’s<br />
chorea, Parkinson’s disease, dystonia, and unilateral<br />
masticatory spasm. Electroenceph Clin Neurophysiol 1991;<br />
81:24–30.<br />
30. Davis M, Gendelman DS, Tischler MD, Gendelman PM. A<br />
primary acoustic startle circuit: lesion and stimulation studies.<br />
J Neurosci 1982;2:791–805.<br />
31. Dehen H, Bathien N, Cambier J. The palmomental reflex.<br />
An electrophysiological study. Eur Neurol 1975;13:395–404.<br />
32. Dengler R, Rechl F, Struppler A. Recruitment of single units<br />
in human blink reflex. Neurosci Lett 1982;34:301–305.<br />
33. Deuschl G, Goddemeier C. Spontaneous and reflex activity<br />
of facial muscles in dystonia, Parkinson’s disease and in normal<br />
subjects. J Neurol Neurosurg Psychiatry 1998;64:<br />
320–324.<br />
34. De Watteville A. Note on the jaw-jerk, or masseteric tendon<br />
reaction, in health and disease. Brain 1886;8:518–519.<br />
35. Eekhof JLA, Aramideh M, Bour LJ, Hilgevoord AAJ, Speelman<br />
JD, Ongerboer de Visser BW. Blink reflex recovery<br />
curves in blepharospasm, torticollis spasmodica and hemifacial<br />
spasm. Muscle Nerve 1996;19:10–15.<br />
36. Eekhof JLA, Aramideh M, Speelman JD, Devriese PP, Ongerboer<br />
de Visser BW. Blink reflexes and lateral spreading in<br />
patients with synkinesia after Bell’s palsy and in hemifacial<br />
spasm. Eur J Neurol 2000;43:141–146.<br />
37. Ellrich J, Hopf HC, Treede RD. Nociceptive masseter inhibitory<br />
reflexes evoked by laser radiant heat and electrical<br />
stimuli. Brain Res 1997;764:214–220.<br />
38. Esteban A. A neurophysiological approach to brainstem reflexes.<br />
Blink reflex. Neurophysiol Clin 1999;29:7–38.<br />
39. Esteban A, Gimenez-Roldan S. Blink reflex in Huntington’s<br />
chorea and Parkinson’s disease. Acta Neurol Scand 1975;52:<br />
145–157.<br />
40. Evinger C, Shaw MD, Peck CK, Manning KA, Baker R. Blinking<br />
and associated eye movements in humans, guinea pigs<br />
and rabbits. J Neurophysiol 1984;52:323–339.<br />
41. Ferguson IT. Electrical study of jaw and orbicularis oculi<br />
reflexes after trigeminal nerve surgery. J Neurol Neurosurg<br />
Psychiatry 1978;41:819–823.<br />
42. Fisher MA, Shahani B, Young RR. Assessing segmental excitability<br />
after acute rostral lesions: II. The blink reflex. Neurology<br />
1979;29:45–50.<br />
43. Godeaux E, Desmedt JE. Exteroceptive suppression and motor<br />
control of the masseter and temporalis muscles in normal<br />
man. Brain Res 1975;85:447–458.<br />
44. Goldstein JE, Cogan DG. Apraxia of lid opening. Arch Ophthalmol<br />
1965;73:155–159.<br />
45. Goodwill CJ, O’Tuama L. Electromyographic recording of<br />
the jaw reflex in multiple sclerosis. J Neurol Neurosurg Psychiatry<br />
1969;32:6–10.<br />
46. Goor C, Ongerboer de Visser BW. Jaw and blink reflexes in<br />
trigeminal nerve lesions. Neurology 1976;26:95–97.<br />
47. Guberman A. Clinical significance of the corneomandibular<br />
reflex. Arch Neurol 1982,39:1368–1372.<br />
48. Guiot G. Valeur localisaterice et pronostique du reflexe corneo-pterygoidien.<br />
Le phenomene de la diduction lente du<br />
maxillaire. Sem Hopital Paris 1946;22:1368–1396.<br />
49. Hoffman P, Tonnies JF. Nachweis des vollig konstanten<br />
verkommens des Zungen-Kiefer-Reflexes bei Menschen.<br />
Pflugers Archiv 1948;250:103–108.<br />
50. Holstege G, Tan J, van Ham JJ, Graveland GA. Anatomical<br />
observations on the afferent projections to the retractor bulb<br />
motoneuronal cell group and other pathways possibly related<br />
to the blink reflex in the cat. Brain Res 1986;374:<br />
321–334.<br />
51. Hori A, Yasuhara A, Naito H, Yasuhara M. Blink reflex elicited<br />
by auditory stimulation in the rabbit. J Neurol Sci 1986;<br />
76:49–59.<br />
52. Hufschmidt HJ, Spuler H. Mono- and polysynaptic reflexes<br />
of the trigeminal muscles in human sclerosis. J Neurol Neurosurg<br />
Psychiatry 1962;25:332–335.<br />
53. Karpukhina MV, Gokin AP, Limanskii YP. Activation of pontine<br />
and bulbar reticulo-spinal neurons in the cat by somatosensory<br />
stimuli of different modalities. Neurophysiology<br />
1986;18:329–336.<br />
54. Kimura J. Conduction abnormalities of the facial and trigeminal<br />
nerves in polyneuropathy. Muscle Nerve 1982;5:<br />
149–144.<br />
55. Kimura J. Disorder of interneurons in parkinsonism. The<br />
orbicularis oculi reflex to paired stimuli. Brain 1973;96:<br />
87–96.<br />
56. Kimura J. Electrical elicited blink reflex in diagnosis of multiple<br />
sclerosis. Review of 260 patients over a seven-year period.<br />
Brain 1975;98:413–426.<br />
57. Kimura J, Daube J, Burke D, Hallett M, Cruccu G, Ongerboer<br />
de Visser BW, Yanagisawa N, Shimamura M, Rothwell J.<br />
Human reflexes and late responses. Report of an IFCN committee.<br />
Electroencephalogr Clin Neurophysiol 1994;90:<br />
393–403.<br />
58. Kimura J, Lyon LW. Orbicularis oculi reflex in Wallenberg<br />
syndrome: alteration of the late reflex by lesion of the spinal<br />
tract and nucleus of the trigeminal nerve. J Neurol Neurosurg<br />
Psychiatry 1972;35:228–233.<br />
59. Kimura J, Powers JM, Van Allen MW. Reflex response of<br />
orbicularis oculi muscles to supraorbital nerve stimulation.<br />
Study in normal subjects and in peripheral facial paresis.<br />
Arch Neurol 1969;21:193–199.<br />
Brainstem Reflexes MUSCLE & NERVE July 2002 29
60. Kimura J, Rodnitzky RL, Van Allen MW. Electrodiagnostic<br />
study of trigeminal nerve. Orbicularis oculi reflex and masseter<br />
reflex in trigeminal neuralgia, paratrigeminal syndrome,<br />
and other lesions of the trigeminal nerve. Neurology<br />
1970;20:574–583.<br />
61. Kimura J, Wilkinson T, Damasio H, Adams HR Jr, Shivapour<br />
E, Yamada T. Blink reflex in patients with hemispheric cerebrovascular<br />
accident (CVA). J Neurol Sci 1985;67:15–28.<br />
62. Kugelberg E. Facial reflexes. Brain 1952;75:385–396.<br />
63. Leandri M, Favale E. Diagnostic relevance of trigeminal<br />
evoked potentials following infraorbital nerve stimulation. J<br />
Neurosurg 1991;75:244–250.<br />
64. Leandri, M, Parodi CL, Favale E. Early trigeminal evoked<br />
potentials in tumors of the base of the skull and trigeminal<br />
neuralgia. Electroencephalogr Clin Neurophysiol 1988;71:<br />
114–124<br />
65. Lecky BRF, Hughes RAC, Murray NMF. Trigeminal sensory<br />
neuropathy. A study of 22 cases. Brain 1987;110:1463–1485.<br />
66. Lele PP, Wedell G. Sensory nerves of the cornea and cutaneous<br />
sensibility. Exp Neurol 1959;1:334–359.<br />
67. Majoie CBLM, Aramideh M, Hulsmans FJH, Castelijns JA,<br />
van Beek EJR, Ongerboer de Visser BW. Correlation between<br />
electromyographic reflex and MR imaging examinations<br />
of the trigeminal nerve. Am J Neuroradiol 1999;20:<br />
1119–1125.<br />
68. Marsden CD. Blepharospasm-oromandibular dystonia syndrome<br />
(Brueghel’s syndrome): a variant of adult-onset torsion<br />
dystonia J Neurol Neurosurg Psychiatry 1976;39:<br />
1204–1209.<br />
69. McIntyre AK, Robinson RG. Pathway for the jaw jerk in man.<br />
Brain 1959;75:385–396.<br />
70. Miles TS, Turker KS. Decomposition of the human electromyogramme<br />
in an inhibitory reflex. Exp Brain Res 1987;65:<br />
337–342.<br />
71. Miwa H, Imamura N, Kogahara K, Ohori T, Mizuno Y. Somatosensrory<br />
evoked blink response: findings in patients<br />
with Miller Fisher syndrome and in normal subjects. J Neurol<br />
Neurosurg Psychiatry 1995;58:95–99.<br />
72. Miwa H, Nohara C, Hotta M, Shimo Y, Amemiya K. Somatosensory-evoked<br />
blink reflex response: investigation of the<br />
pathophysiological mechanism. Brain 1998;121:281–291.<br />
73. Ongerboer de Visser BW. Afferent limb of the human jaw<br />
reflex: electrophysiologic and anatomic study. Neurology<br />
1982;32:536–546.<br />
74. Ongerboer de Visser BW. Anatomical and functional organization<br />
of reflexes involving the trigeminal system in man:<br />
jaw reflex, blink reflex, corneal reflex and exteroceptive suppression.<br />
Adv Neurol 1983;39:729–738.<br />
75. Ongerboer de Visser BW. Comparative study of corneal and<br />
blink reflex latencies in patients with segmental or with central<br />
lesions. Adv Neurol 1983;39:757–772.<br />
76. Ongerboer de Visser BW. Corneal reflex latency in lesions of<br />
the lower postcentral region. Neurology 1981;31:701–707.<br />
77. Ongerboer de Visser BW. The recorded corneo-mandibular<br />
reflex. Electroencephalogr Clin Neurophysiol 1986;63:<br />
25–31.<br />
78. Ongerboer de Visser BW, Cruccu G. Neurophysiologic examination<br />
of the trigeminal, facial, hypoglossal, and spinal<br />
accessory nerves in cranial neuropathies and brainstem disorders.<br />
In: Brown WF, Bolton CF, editors. Clinical electromyography.<br />
Boston: Butterworths; 1993. p 61–92.<br />
79. Ongerboer de Visser BW, Cruccu G, Manfredi M, Koelman<br />
JHTM. Effects of brainstem lesions on the masseter inhibitory<br />
reflex. Functional mechanisms of reflex pathways. Brain<br />
1990;113:781–792.<br />
80. Ongerboer de Visser BW, Goor C. Electromyographic and<br />
reflex study in idiopathic and symptomatic trigeminal neuralgias:<br />
latency of the jaw and blink reflexes. J Neurol Neurosurg<br />
Psychiatry 1974;37:1225–1230.<br />
81. Ongerboer de Visser BW, Goor C. Jaw reflexes and masseteric<br />
electromyograms in mesencephalic and pontine lesions.<br />
An electrophysiologic study. J Neurol Neurosurg Psychiatry<br />
1976;39:90–92.<br />
82. Ongerboer de Visser BW, Kuypers HGJM. Late blink reflex<br />
changes in lateral medullary lesions. An electrophysiological<br />
and neuroanatomical study of Wallenberg’s syndrome. Brain<br />
1978;101:285–94.<br />
83. Ongerboer de Visser BW, Mechelse K, Megens PHA. Corneal<br />
reflex latency in trigeminal nerve lesions. Neurology<br />
1977;27:1164–1167.<br />
84. Ongerboer de Visser BW, Moffie D. Effects of brainstem and<br />
thalamic lesions on the corneal reflex. An electrophysiological<br />
and anatomical study. Brain 1979;102:595–608.<br />
85. Overend W. Preliminary note on a new cranial reflex. Lancet<br />
1896;1:619.<br />
86. Pastor P, Muñoz E, Valldeoriola F. Enhanced blink rate and<br />
involuntary contralateral eye closure in patients with Bell’s<br />
palsy. Muscle Nerve 1998;21:1596.<br />
87. Pennisi E, Cruccu G, Manfredi M, Palladini G. Histometiric<br />
study of myelinated fibers in the human trigeminal nerve. J<br />
Neurol Sci 1991;105:22–28.<br />
88. Selby G. Diseases of the fifth cranial nerve. In: Dyck PJ,<br />
Thomas PK, Lambert EH, Bunge E, editors. Peripheral neuropathy.<br />
Philadelphia: WB Saunders; 1984. p 1224–1265.<br />
89. Shahani BT. The human blink reflex. J Neurol Neurosurg<br />
Psychiatry 1970;33:792–800.<br />
90. Shahani BT, Young RR. Human orbicularis oculi reflexes.<br />
Neurology 1972;22:149–154.<br />
91. Syed NA, Delgado A, Sandbrink F, Schulman AE, Hallett M,<br />
Floeter MK. Blink reflex recovery in facial weakness. An electrophysiological<br />
study of adaptive changes. Neurology 1999;<br />
52:834–838.<br />
92. Tavy DL, van Woerkom TCAM, Bots GTAM, Endtz LJ. Persistence<br />
of the blink reflex to sudden illumination in a comatose<br />
patient. Arch Neurol 1984;42:323–324.<br />
93. Tolosa E, Montserrat L, Bayes A. Blink reflex studies in focal<br />
dystonias. Enhanced excitability of brainstem interneurones<br />
in cranial dystonia and spasmodic torticollis. Mov Disord<br />
1988;3:61–69.<br />
94. Valls-Solé J, Cammarota A, Alvarez R, Hallett M. Orbicularis<br />
oculi responses to stimulation of nerve afferents from upper<br />
and lower limbs in normal humans. Neurosci Lett 1994;650:<br />
313–316.<br />
95. Valls-SoléJ, Graus F, Font J, Pou A, Tolosa ES. Normal proprioceptive<br />
trigeminal afferents in patients with Sjogren’s<br />
syndrome and sensory neuropathy. Ann Neurol 1990;28:<br />
786–790.<br />
96. VanderWerf F, Aramideh M, Ongerboer de Visser BW, Baljet<br />
B, Speelman JD, Otto JA. A retrograde double fluorescent<br />
tracing study of the levator palpebrae superioris muscle in<br />
the cynomolgous monkey. Exp Brain Res 1997;113:174–179.<br />
97. Weiskrantz L, Wanington EK, Sanders MD, Marshall J. Visual<br />
capacity in the hemianoptic field following a restricted occipital<br />
ablation. Brain 1974;97:700–728.<br />
98. Wieser ST, Muller-Fahlbusch H. Ueber nociceptive reflexe<br />
des gesichtes. Dtsch Z Nervenheilk 1962;183:530–543.<br />
99. Wilkins DE, Hallett M, Wess MM. Audiogenic startle reflex of<br />
man and its relationship to startle syndromes: a review. Brain<br />
1986;109:561–573.<br />
100. Yates SK, Brown WF. Light-stimulus–evoked blink reflex:<br />
methods, normal values, reaction to other blink reflexes,<br />
and observation in multiple sclerosis. Neurology 1981;32:<br />
272–281.<br />
101. Yates SK, Brown WF. The human jaw-jerk: electrophysiologic<br />
methods to measure the latency, normal values, and changes<br />
in multiple sclerosis. Neurology 1981;31:632–634.<br />
30 Brainstem Reflexes MUSCLE & NERVE July 2002