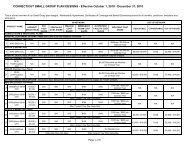
Housecall Newsletter - ConnectiCare
Housecall Newsletter - ConnectiCare
Housecall Newsletter - ConnectiCare

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ight to appeal<br />
IF YOU’RE NOT SATISFIED<br />
You have the right to appeal a decision if we do not provide coverage for a treatment or service.<br />
There may be times when you do not agree with a<br />
decision that we make about “Medical Necessity.”<br />
This is important because if a service is not considered<br />
Medically Necessary, we will not pre-authorize it or<br />
provide coverage for it. As a result, your plan will not<br />
pay for the service at the highest level of benefits, or<br />
your plan may not pay for the service at all.<br />
If you do not agree with our decision, you have the<br />
right to request an appeal.<br />
YOUR MEDICAL-NECESSITY APPEAL WILL<br />
RECEIVE INDEPENDENT REVIEW<br />
We will forward your appeal to an independent review<br />
organization. A board-certified physician will review<br />
the case. The physician will be a specialist in the field<br />
related to the condition in the appeal. He or she will not<br />
have been involved in the original decision, and will not<br />
be a <strong>ConnectiCare</strong> employee.<br />
If you’re not satisfied with the review decision, there<br />
is another step. You may be eligible for an external<br />
review. This is provided through the state in which your<br />
insurance plan was issued or through an independent<br />
review organization for self-funded plans. When we<br />
send you the review decision, we’ll provide information<br />
in writing about how to pursue an external review.<br />
WHAT IS THE DEFINITION OF<br />
‘MEDICALLY NECESSARY’<br />
“Medically Necessary” means health services that a<br />
health care practitioner, exercising prudent clinical<br />
judgment, would provide to a patient for the purpose of<br />
preventing, evaluating, diagnosing or treating an illness,<br />
injury, disease or its symptoms, and that are:<br />
• In accordance with generally accepted standards<br />
of medical practice<br />
• Clinically appropriate, in terms of type, frequency,<br />
extent, site and duration considered effective for<br />
the patient’s illness, injury or disease, and<br />
• Not primarily for the convenience of the patient,<br />
physician or other health care provider; and not<br />
more costly than an alternative service or sequence<br />
of services at least as likely to produce equivalent<br />
therapeutic or diagnostic results as to the diagnosis<br />
or treatment of that patient’s illness, injury or disease.<br />
We use medical protocols<br />
developed from national<br />
standards with input from<br />
local physicians, including<br />
specialists, to establish<br />
our guidelines for<br />
what is considered<br />
Medically Necessary.<br />
PEACE OF MIND FOR EVERY WOMAN<br />
Your coverage under Women’s Health and Cancer Rights Act<br />
Do you know that your plan provides benefits for mastectomy-related services, as required by the Women’s<br />
Health and Cancer Rights Act of 1998 Covered benefits include all stages of reconstruction and surgery to<br />
achieve symmetry between the breasts, prostheses, and complications resulting from a mastectomy, including<br />
lymphedema. These services offer peace of mind for any woman with breast cancer who chooses to have a<br />
mastectomy. For more information, contact your benefits administrator or go to the U.S. Department of Labor<br />
website at www.dol.gov and enter “WHCRA” in the search field.