400N Enrollment Form - Dental Alternatives Insurance Services Inc
400N Enrollment Form - Dental Alternatives Insurance Services Inc
400N Enrollment Form - Dental Alternatives Insurance Services Inc

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
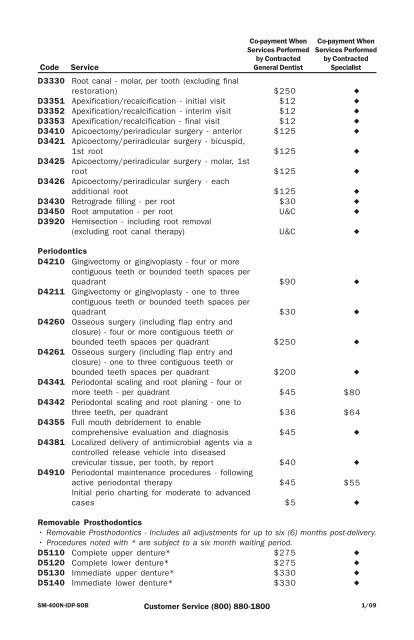
Code<br />
D3330<br />
D3351<br />
D3352<br />
D3353<br />
D3410<br />
D3421<br />
D3425<br />
D3426<br />
D3430<br />
D3450<br />
D3920<br />
Service<br />
Root canal - molar, per tooth (excluding final<br />
restoration)<br />
Apexification/recalcification - initial visit<br />
Apexification/recalcification - interim visit<br />
Apexification/recalcification - final visit<br />
Apicoectomy/periradicular surgery - anterior<br />
Apicoectomy/periradicular surgery - bicuspid,<br />
1st root<br />
Apicoectomy/periradicular surgery - molar, 1st<br />
root<br />
Apicoectomy/periradicular surgery - each<br />
additional root<br />
Retrograde filling - per root<br />
Root amputation - per root<br />
Hemisection - including root removal<br />
(excluding root canal therapy)<br />
Periodontics<br />
D4210 Gingivectomy or gingivoplasty - four or more<br />
contiguous teeth or bounded teeth spaces per<br />
quadrant<br />
D4211 Gingivectomy or gingivoplasty - one to three<br />
contiguous teeth or bounded teeth spaces per<br />
quadrant<br />
D4260 Osseous surgery (including flap entry and<br />
closure) - four or more contiguous teeth or<br />
bounded teeth spaces per quadrant<br />
D4261 Osseous surgery (including flap entry and<br />
closure) - one to three contiguous teeth or<br />
bounded teeth spaces per quadrant<br />
D4341 Periodontal scaling and root planing - four or<br />
more teeth - per quadrant<br />
D4342 Periodontal scaling and root planing - one to<br />
three teeth, per quadrant<br />
D4355 Full mouth debridement to enable<br />
comprehensive evaluation and diagnosis<br />
D4381 Localized delivery of antimicrobial agents via a<br />
controlled release vehicle into diseased<br />
crevicular tissue, per tooth, by report<br />
D4910 Periodontal maintenance procedures - following<br />
active periodontal therapy<br />
Initial perio charting for moderate to advanced<br />
cases<br />
Co-payment When<br />
<strong>Services</strong> Performed<br />
by Contracted<br />
General Dentist<br />
$250<br />
$12<br />
$12<br />
$12<br />
$125<br />
$125<br />
$125<br />
$125<br />
$30<br />
U&C<br />
• Procedures noted with * are subject to a six month waiting period.<br />
D5110<br />
D5120<br />
D5130<br />
D5140<br />
Complete upper denture*<br />
Complete lower denture*<br />
Immediate upper denture*<br />
Immediate lower denture*<br />
$275<br />
$275<br />
$330<br />
$330<br />
SM-<strong>400N</strong>-IDP-SOB Customer Service (800) 880-1800<br />
1/09<br />
U&C<br />
$90<br />
$30<br />
$250<br />
$200<br />
$45<br />
$36<br />
$45<br />
$40<br />
$45<br />
$5<br />
Co-payment When<br />
<strong>Services</strong> Performed<br />
by Contracted<br />
Specialist<br />
•<br />
•<br />
•<br />
•<br />
•<br />
•<br />
•<br />
•<br />
•<br />
•<br />
•<br />
$80<br />
•<br />
•<br />
•<br />
•<br />
$64<br />
•<br />
•<br />
$55<br />
•<br />
Removable Prosthodontics<br />
• Removable Prosthodontics - <strong>Inc</strong>ludes all adjustments for up to six (6) months post-delivery.<br />
•<br />
•<br />
•