Remicade Order Form - Florida Health Care Plans
Remicade Order Form - Florida Health Care Plans
Remicade Order Form - Florida Health Care Plans

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
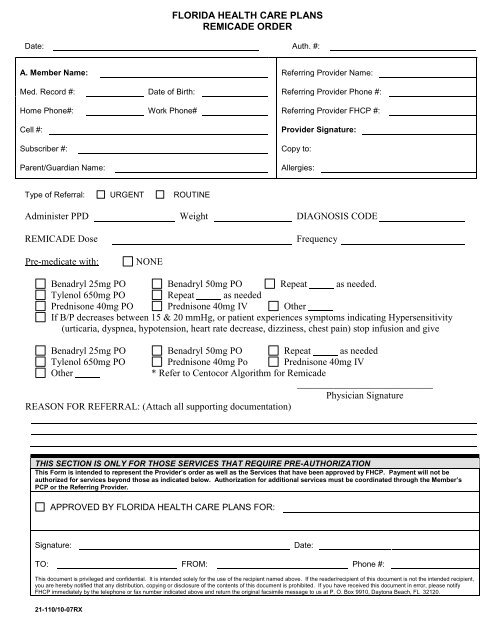
FLORIDA HEALTH CARE PLANS<br />
REMICADE ORDER<br />
Date: Auth. #:<br />
A. Member Name: Referring Provider Name:<br />
Med. Record #: Date of Birth: Referring Provider Phone #:<br />
Home Phone#: Work Phone# Referring Provider FHCP #:<br />
Cell #:<br />
Subscriber #:<br />
Parent/Guardian Name:<br />
Provider Signature:<br />
Copy to:<br />
Allergies:<br />
Type of Referral: URGENT ROUTINE<br />
Administer PPD Weight DIAGNOSIS CODE<br />
REMICADE Dose<br />
Frequency<br />
Pre-medicate with:<br />
NONE<br />
Benadryl 25mg PO Benadryl 50mg PO Repeat as needed.<br />
Tylenol 650mg PO Repeat as needed<br />
Prednisone 40mg PO Prednisone 40mg IV Other<br />
If B/P decreases between 15 & 20 mmHg, or patient experiences symptoms indicating Hypersensitivity<br />
(urticaria, dyspnea, hypotension, heart rate decrease, dizziness, chest pain) stop infusion and give<br />
Benadryl 25mg PO Benadryl 50mg PO Repeat as needed<br />
Tylenol 650mg PO Prednisone 40mg Po Prednisone 40mg IV<br />
Other<br />
* Refer to Centocor Algorithm for <strong>Remicade</strong><br />
____________________________<br />
Physician Signature<br />
REASON FOR REFERRAL: (Attach all supporting documentation)<br />
THIS SECTION IS ONLY FOR THOSE SERVICES THAT REQUIRE PRE-AUTHORIZATION<br />
This <strong>Form</strong> is intended to represent the Provider’s order as well as the Services that have been approved by FHCP. Payment will not be<br />
authorized for services beyond those as indicated below. Authorization for additional services must be coordinated through the Member’s<br />
PCP or the Referring Provider.<br />
APPROVED BY FLORIDA HEALTH CARE PLANS FOR:<br />
Signature:<br />
Date:<br />
TO: FROM: Phone #:<br />
This document is privileged and confidential. It is intended solely for the use of the recipient named above. If the reader/recipient of this document is not the intended recipient,<br />
you are hereby notified that any distribution, copying or disclosure of the contents of this document is prohibited. If you have received this document in error, please notify<br />
FHCP immediately by the telephone or fax number indicated above and return the original facsimile message to us at P. O. Box 9910, Daytona Beach, FL 32120.<br />
21-110/10-07RX
PROCEDURE FOR ORDERING REMICADE<br />
<strong>Remicade</strong> is a monoclonal antibody agent known to be effective in the treatment of Crohn’s Disease and Rheumatoid<br />
Arthritis, Ulcerative Colitis, Ankylosing Spondylitis, and Psoriatic Arthritis.<br />
Approval for treatment of Crohn’s Disease is based on failure of both an anti-inflammatory agent (5-ASA compounds,<br />
sulfasalazine, Dipentum, Pentasa, Asacol & Rowasa) and an immunosuppressant (purinethol, azothioprine,<br />
methotrexate). Intermittent steroids and antibiotics used to manage exacerbations and maintain remission are not<br />
sufficient to satisfy immunosuppressant and anti-inflammatory trials.<br />
Approval for treatment of Ulcerative Colitis is based on history of moderate to severe ulcerative colitis in patients who<br />
have contraindications to or have failed both therapeutically effective doses of Aminosalicilates (sulfasalizine 4-<br />
6g/day, mesalamine 2-4.8g/day, balsalazide 6.75g/day, olsalazine 1.5-3g/day), and an Immunomodulator (6-<br />
mercaptopurine or azothioprine) or continuous corticosteroid. Approved injections will be covered at weeks 0,2,6, and<br />
then every 8 weeks at the labeled dosage (5mg/kg).<br />
Approval for treatment of rheumatoid arthritis (RA), And Psoriatic Arthritis is based on failure of Humira (2 nd in line<br />
to Enbrel failures). Note: <strong>Remicade</strong> is only indicated for treatment of RA in combination with methotrexate.<br />
PROCEDURE:<br />
• <strong>Order</strong>ing physician will send completed <strong>Remicade</strong> order (form 21-110) and supporting documentation to the<br />
FHCP Referral Department<br />
• <strong>Order</strong> must include dose of REMICADE, frequency, Pre-medication order and orders to follow if reaction to<br />
infusion<br />
• Documentation of PPD within one year or order for PPD before first treatment.<br />
• If approved, Referral Department will notify physician office and send signed form to FHCP Infusion Clinic:<br />
‣ Daytona Facility<br />
‣ Orange City Facility<br />
‣ Palm Coast Facility<br />
‣ Edgewater Facility<br />
• Infusion Clinic will call patient to set up appointment for PPD<br />
• Infusion Clinic Nurse will place and read PPD, and assess for any s / s infection<br />
• If patient has a previous positive PPD, order chest x-ray with copy to Infusion Clinic<br />
• Infusion nurse will assess for signs and symptoms of TB and document on nurse assessment and <strong>Remicade</strong><br />
order form<br />
• Infusion Clinic Nurse will send order for <strong>Remicade</strong> to Pharmacy<br />
• Clinic will schedule patient for appointment for <strong>Remicade</strong> infusion<br />
• Medicare patients will pick up medication at Pharmacy and bring with him/her to appointment at Infusion<br />
Clinic, all other members <strong>Remicade</strong> will be shipped to infusion clinic.<br />
• <strong>Order</strong>ing physician will provide patient with information and educational materials<br />
21-110/10-07RX