Original Contributions of Latin-Ameri- cans to Anesthesia
Original Contributions of Latin-Ameri- cans to Anesthesia
Original Contributions of Latin-Ameri- cans to Anesthesia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
A H A<br />
VOLUME 20, NUMBER 2<br />
<strong>Original</strong> <strong>Contributions</strong> <strong>of</strong> <strong>Latin</strong>-<strong>Ameri</strong><strong>cans</strong><br />
<strong>to</strong> <strong>Anesthesia</strong><br />
By J. An<strong>to</strong>nio Aldrete, M.D., M.S.<br />
Clinical Pr<strong>of</strong>essor, Department <strong>of</strong> Anesthesiology, University <strong>of</strong> South Florida,<br />
Tampa, FL and Aldrete Pain Care Center, Chipley, FL<br />
and<br />
Carlos P. Parsloe, M.D.<br />
Former President World Federation <strong>of</strong> Societies <strong>of</strong> Anesthesiologists,<br />
Hospital Samaritano, São Paulo, Brasil<br />
APRIL, 2002<br />
Most Chapters in text books <strong>of</strong> <strong>Anesthesia</strong><br />
dealing with the his<strong>to</strong>ry <strong>of</strong> this<br />
specialty include the same events <strong>to</strong>ld in a<br />
different manner with certain emphasis on<br />
certain regions <strong>of</strong> the world, the country on<br />
which language the book is written and/<br />
or the special subject <strong>of</strong> interest <strong>to</strong> the author.<br />
Since most books in <strong>Anesthesia</strong> have<br />
been written in the English language, by<br />
English speaking authors, there has been<br />
a certain tendency <strong>to</strong> have certain origins<br />
<strong>of</strong> this specialty emphasized; after all the<br />
first anesthetics were given in Georgia and<br />
Massachusetts 1,2 , followed by its application<br />
and ample promotion in the United Kingdom<br />
as John Snow administered ether and<br />
chlor<strong>of</strong>orm within a month. 3<br />
Nevertheless, there is a considerable<br />
number <strong>of</strong> important and original contributions<br />
made by non-English speaking<br />
authors dispersed among the non-English<br />
medical literature that deserves recognition,<br />
debate and consideration as <strong>to</strong> the role they<br />
might have had on the advancement <strong>of</strong> this<br />
our beloved Specialty. With this preamble,<br />
we would like <strong>to</strong> describe some events that<br />
merit acknowledgement not only because<br />
they were innovations at the time, but also<br />
because some <strong>of</strong> them were conducted under<br />
hardship, the participants had limited<br />
economical resources and little technological<br />
support but that also suggests that the<br />
protagonists had a great deal <strong>of</strong> ingenuity,<br />
courage, clear thinking and perseverance.<br />
Specifically, these events were carried on by<br />
colleagues from <strong>Latin</strong> <strong>Ameri</strong>can countries,<br />
most <strong>of</strong> their deeds were published in nonindexed<br />
journals and therefore many <strong>of</strong><br />
them were forgotten or ignored.<br />
First Anesthetics in a War<br />
An important his<strong>to</strong>rical event needs mentioning<br />
as a point <strong>of</strong> clarification since prior<br />
<strong>to</strong> its finding it was thought that the first<br />
anesthetic in a war conflict was administered<br />
in the Crimean War in 1854. 4 Nevertheless,<br />
his<strong>to</strong>rical data revealed otherwise. When<br />
WGT Mor<strong>to</strong>n administered in Bos<strong>to</strong>n the<br />
first public ether anesthetic on Oc<strong>to</strong>ber 16,<br />
1846 1 , the United States and the Republic<br />
<strong>of</strong> Mexico were engaged in a war initiated<br />
about seven months earlier by the separation<br />
<strong>of</strong> Texas from the latter and its recent<br />
admission as a State in<strong>to</strong> the former. Soon<br />
thereafter Mor<strong>to</strong>n <strong>of</strong>fered <strong>to</strong> train military<br />
surgeons on etherisation. On the other hand,<br />
once the news <strong>of</strong> the first successful ether<br />
application was known, a military surgeon<br />
in semiretirement in New Orleans, Dr. Edward<br />
H. Bar<strong>to</strong>n (Figure 1) proposed <strong>to</strong> the<br />
War Department the possible application <strong>of</strong><br />
ether in the battle field and requested full<br />
reinstatement; by December President Polk<br />
had approved the request so Bar<strong>to</strong>n would<br />
receive instruction on the use <strong>of</strong> Letheon and<br />
could then administer it <strong>to</strong> injured soldiers.<br />
Since the land campaign commanded by<br />
General Zachary Taylor, through Texas, and<br />
northern Mexico appeared <strong>to</strong> be slow and<br />
costly in supplies and casualties as demonstrated<br />
from the fierce battles <strong>of</strong> Palo Al<strong>to</strong>,<br />
Resaca de la Palma, Buena Vista (Angostura)<br />
and Monterrey, President Polk and the War<br />
Department agreed that General Winfield<br />
Scott would initiate what appeared <strong>to</strong> be a<br />
shorter campaign by landing in Vera Cruz<br />
and advancing <strong>to</strong>ward the capital.<br />
On February <strong>of</strong> 1847, Bar<strong>to</strong>n was sent by<br />
Figure 1: Military surgeon Edward H.<br />
Bar<strong>to</strong>n commissioned by the U.S. War<br />
Department <strong>to</strong> use Letheon on injured soldiers<br />
undergoing surgery.<br />
way <strong>of</strong> La Havana, <strong>to</strong> join the fleet blockading<br />
the central part <strong>of</strong> the Mexican Gulf<br />
under Scott’s command. On early March,<br />
the first <strong>Ameri</strong>can troops landed south <strong>of</strong><br />
the port and entered Vera Cruz after running<br />
in<strong>to</strong> mild resistance. In the process <strong>of</strong><br />
disembarking, a German porter recently<br />
recruited, was accidentally shot in his legs<br />
when a musket discharged spontaneously<br />
while he was unloading a wagon. After attempts<br />
<strong>to</strong> save the porter’s legs failed,<br />
Continued on page 4
2 BULLETIN OF ANESTHESIA HISTORY<br />
<strong>Anesthesia</strong> Foundation<br />
Book/Multimedia Education Award<br />
The <strong>Anesthesia</strong> Foundation announces the Book/Multimedia Education Award <strong>to</strong> be presented 2003 at the <strong>Ameri</strong>can Society<br />
<strong>of</strong> Anesthesiologists Annual Meeting.<br />
This prestigious award will be awarded tri-yearly for excellence and innovation in books or multimedia with significant impact<br />
on the science and practice <strong>of</strong> anesthesiology, critical care, or pain medicine. Multiple authors are eligible with the stipend being<br />
divided between the first and senior authors.<br />
The award is $10,000, plus expenses for winners and guests <strong>to</strong> attend the Academy <strong>of</strong> Anesthesiology 2004 Spring meeting in<br />
Vic<strong>to</strong>ria Island, Canada.<br />
Deadline for receipt <strong>of</strong> contributions is November 15, 2002.<br />
For further information and specific criterion please contact:<br />
Doris K. Cope, M.D.<br />
UPMC St. Margaret Pain Medicine Center<br />
200 Delafield Avenue, Suite 2070<br />
Pittsburgh, PA 15215<br />
412-784-5343 (phone)<br />
412-784-5350 (fax)<br />
<strong>Anesthesia</strong> His<strong>to</strong>ry Association<br />
Sixth Annual Resident Essay Contest<br />
The <strong>Anesthesia</strong> His<strong>to</strong>ry Association (AHA) sponsors an annual Resident Essay Contest with the prize presented at<br />
the ASA Annual Meeting.<br />
A 1,500-3,000-word essay related <strong>to</strong> the his<strong>to</strong>ry <strong>of</strong> anesthesia, pain management or critical care should be submitted <strong>to</strong>:<br />
William D. Hammonds, M.D., M.P.H.<br />
Chair, AHA Resident Essay Contest<br />
University <strong>of</strong> Iowa<br />
School <strong>of</strong> Medicine<br />
Dept. <strong>of</strong> <strong>Anesthesia</strong><br />
200 Hawkins Drive, 6 JCP<br />
Iowa City, IA 52242-1079<br />
U.S.A.<br />
The entrant must have written the essay either during his/her residency or within one year <strong>of</strong> completion <strong>of</strong> residency.<br />
Residents/Fellows in any nation are eligible, but the essay MUST be submitted in English. All submissions<br />
must be typewritten.<br />
An honorarium <strong>of</strong> $500.00 and a certificate will be awarded at the AHA’s annual dinner meeting at the ASA.<br />
The award-winning residents will be invited <strong>to</strong> present their essays in person at the annual spring meeting <strong>of</strong> the<br />
AHA and their work will be published in the Bulletin <strong>of</strong> <strong>Anesthesia</strong> His<strong>to</strong>ry.<br />
All entries must be received on or before August 15, 2002.
BULLETIN OF ANESTHESIA HISTORY 3<br />
Letter <strong>to</strong> the Edi<strong>to</strong>r<br />
Dear Dr. Cope:<br />
Recently I received from a friend anesthesiologist, a donation for the Museum<br />
<strong>of</strong> the His<strong>to</strong>ry <strong>of</strong> Anesthesiology <strong>of</strong> Puer<strong>to</strong> Rico and the Caribbean two interesting<br />
articles:<br />
1. A Squibb ether can (see pho<strong>to</strong>). Used many years ago for administering open<br />
drop ether anesthesia. It is unopened and still full <strong>of</strong> ether.<br />
2) An interesting device I had not seen before or read about. It looks and could<br />
be a precursor <strong>of</strong> the presently used LMA Device.<br />
Perhaps the pho<strong>to</strong> enclosed if published in the Newsletter requesting readers <strong>to</strong><br />
send any information or reference they might have concerning its inven<strong>to</strong>r and use<br />
might be obtained from them.<br />
Looking forward <strong>to</strong> meeting you again, with my best wishes.<br />
Cordially yours,<br />
Miguel Colon-Morales, M.D.<br />
Bulletin <strong>of</strong> <strong>Anesthesia</strong> His<strong>to</strong>ry (ISSN 1522-<br />
8649) is published four times a year as a joint<br />
effort <strong>of</strong> the <strong>Anesthesia</strong> His<strong>to</strong>ry Association and<br />
the Wood-Library Museum <strong>of</strong> Anesthesiology.<br />
The Bulletin was published as <strong>Anesthesia</strong> His<strong>to</strong>ry<br />
Association Newsletter through Vol. 13, No. 3,<br />
July 1995.<br />
The Bulletin, formerly indexed in Histline, is<br />
now indexed in several databases maintained by<br />
the U.S. National Library <strong>of</strong> Medicine as follows:<br />
1. Monographs: Old citations <strong>to</strong> his<strong>to</strong>rical<br />
monographs (including books, audiovisuals,<br />
serials, book chapters, and meeting papers) are<br />
now in LOCATORplus (http://loca<strong>to</strong>rplus.gov),<br />
NLM’s web-based online public access catalog,<br />
where they may be searched separately from now<br />
on, along with newly created citations.<br />
2. Journal Articles: Old citations <strong>to</strong> journals<br />
have been moved <strong>to</strong> PubMed (http://www.<br />
ncbi.nlm.nih.gov/PubMed), NLM’s web-based<br />
retrieval system, where they may be searched<br />
separately along with newly created citations.<br />
3. Integrated His<strong>to</strong>ry Searches: NLM has online<br />
citations <strong>to</strong> both types <strong>of</strong> his<strong>to</strong>rical literature<br />
-- journal articles as well as monographs -- again<br />
accessible through a single search location, The<br />
Gateway (http://gateway.nlm.nih.gov).<br />
C.R. Stephen, MD, Senior Edi<strong>to</strong>r<br />
Doris K. Cope, MD, Edi<strong>to</strong>r<br />
Donald Ca<strong>to</strong>n, MD, Associate Edi<strong>to</strong>r<br />
A.J. Wright, MLS, Associate Edi<strong>to</strong>r<br />
Fred Spielman, MD, Associate Edi<strong>to</strong>r<br />
Douglas Bacon, MD, Associate Edi<strong>to</strong>r<br />
Peter McDermott, MD, Book Review Edi<strong>to</strong>r<br />
Deborah Bloomberg, Edi<strong>to</strong>rial Staff<br />
Edi<strong>to</strong>rial, Reprint, and Circulation matters<br />
should be addressed <strong>to</strong>:<br />
Edi<strong>to</strong>r<br />
Bulletin <strong>of</strong> <strong>Anesthesia</strong> His<strong>to</strong>ry<br />
200 Delafield Avenue, Suite 2070<br />
Pittsburgh, PA 15215 U.S.A.<br />
Telephone (412) 784-5343<br />
Fax (412) 784-5350<br />
bloombergdj@anes.upmc.edu<br />
Manuscripts may be submitted on disk using<br />
Word for Windows or other PC text program.<br />
Please save files in RICH TEXT FORMAT (.rtf)<br />
if possible and submit a hard copy prin<strong>to</strong>ut in<br />
addition <strong>to</strong> the disk. All illustrations/pho<strong>to</strong>s<br />
MUST be submitted as original hard copy, not<br />
electronically. Pho<strong>to</strong>graphs should be original<br />
glossy prints, NOT pho<strong>to</strong>copies, laser prints or<br />
slides. Pho<strong>to</strong>copies <strong>of</strong> line drawings or other<br />
artwork are NOT acceptable for publication.
4 BULLETIN OF ANESTHESIA HISTORY<br />
<strong>Contributions</strong>. . .Continued from page 1<br />
it was decided <strong>to</strong> amputate both. It was<br />
reported that in spite <strong>of</strong> the surgeon’s skills<br />
and expediency, the porter screamed, cried<br />
and swore throughout the first amputation<br />
so the second was postponed. On the next<br />
day, the 29th <strong>of</strong> March, Bar<strong>to</strong>n assisted by<br />
military surgeons Drs. Harney, Porter and<br />
Laub, proceeded <strong>to</strong> administer the first anesthetic<br />
in a war according <strong>to</strong> the technique<br />
he had been instructed on with an inhaler<br />
similar <strong>to</strong> the one Mor<strong>to</strong>n used in Bos<strong>to</strong>n six<br />
months earlier. It was noted that the porter<br />
slept through the whole operation, “without<br />
moving one muscle” under the effects <strong>of</strong><br />
Letheon and woke up cheerful and without<br />
a complaint at the end <strong>of</strong> it. 5<br />
John Porter wrote a treatise on military<br />
medicine 6 at the end <strong>of</strong> the war, since he<br />
apparently acquired more experience with<br />
ether during the remaining <strong>of</strong> the War his<br />
comments were not encouraging since he<br />
stated that anesthesia was dangerous and<br />
unnecessary in injured soldiers who were<br />
expected <strong>to</strong> <strong>to</strong>lerate the pain and suffering <strong>of</strong><br />
these brief procedures. He reported several<br />
near lethal experiences in injured hypovolemic<br />
soldiers probably from overdose as<br />
ether would vaporize more readily in warm<br />
Vera Cruz in the Spring and in the Summer<br />
<strong>of</strong> 1847 in the Mexican altiplano at 7400<br />
feet high, than at sea level in Bos<strong>to</strong>n, in the<br />
Winter <strong>of</strong> 1846. 5<br />
Scott’s army moved westward <strong>to</strong> the next<br />
largest city, Xalapa where General An<strong>to</strong>nio<br />
Lopez de Santanna, by then the Mexican<br />
president, had fortified two promon<strong>to</strong>ries<br />
that dominated the road where the troops<br />
had <strong>to</strong> go through. On one, Cerro Gordo,<br />
seven gun batteries were in place <strong>to</strong> bombard<br />
the approaching invading army. At<br />
night an <strong>Ameri</strong>can battalion led by captain<br />
Robert E. Lee, commander <strong>of</strong> engineers,<br />
circumvented the promon<strong>to</strong>ries and climbed<br />
Cerro Gordo rushing the batteries and turning<br />
them against the Mexican army camped<br />
before Xalapa. A fierce battle followed in<br />
which lieutenant George B. McCleland and<br />
captain P.G.T. Beauregard distinguished<br />
themselves in action (Figure 2). Eventually<br />
the <strong>Ameri</strong>can forces entered Xalapa on April<br />
18. Porter described that nearly a dozen <strong>of</strong><br />
injured soldiers had surgical procedures<br />
under letheon.<br />
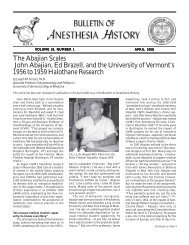
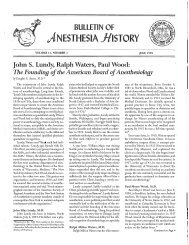
Of interest was the finding <strong>of</strong> a daguerreotype<br />
published in the Xalapa’s newspaper<br />
showing the Mexican military surgeon Pedro<br />
Van der Linden about <strong>to</strong> start a leg amputation<br />
in a Mexican soldier that appears<br />
asleep, while the group is taken prisoner<br />
as bayonets (supposedly in the hands <strong>of</strong><br />
<strong>Ameri</strong>can soldiers) guard them, implying<br />
Figure 2: Civil War leaders <strong>to</strong> be, Captain Robert E. Lee, St. George B. McCleland<br />
and Captain P.G.T. Beauregard distinguished themselves at the battle <strong>of</strong> Cerro<br />
Gordo.<br />
that Van der Linden, a bright young surgeon<br />
<strong>of</strong> Dutch descent had administered ether<br />
<strong>to</strong> the soldier about <strong>to</strong> be operated 7 (Figure<br />
3). He eventually was freed and rejoined<br />
the Mexican army caring for soldiers in the<br />
battles <strong>of</strong> Padierna , Molino del Rey and<br />
Chapultepec along with other distinguished<br />
physicians such as Jose Pablo Martinez<br />
del Rio y Miguel Jimenez who apparently<br />
also gave ether inhalation for amputations.<br />
Whether they obtained the ether from their<br />
<strong>Ameri</strong>can counterparts or they had it send<br />
from abroad, is not known, but Martinez<br />
del Rio (Figure 4) later on claimed that he<br />
had received bottles <strong>of</strong> ether and chlor<strong>of</strong>orm<br />
from the United Kingdom and had trained<br />
other military doc<strong>to</strong>rs <strong>to</strong> administer it with<br />
a handkerchief 8,9 ; though this fact has not<br />
been confirmed.<br />
Important Anesthetic Experiences in<br />
the XIX Century<br />
Initially, advances were prevalent in two<br />
countries, whether this was due <strong>to</strong> daring<br />
physicians willing <strong>to</strong> undertake new approaches<br />
or simply that the events were duly<br />
recorded either in newspapers or medical<br />
publications. Specifically in Brazil two adventurous<br />
surgical interventions presented<br />
challenges far out <strong>of</strong> the ordinary anesthetic<br />
techniques <strong>to</strong> facilitate the performance <strong>of</strong><br />
these unusual operations.<br />
In 1866, Pacifico Pereira 10 , a surgeon in<br />
Bahia, excised a sublingual osteoma <strong>of</strong> the<br />
mandible using ether applied <strong>to</strong>pically over<br />
the mucosa producing local frosting and<br />
vasoconstriction.<br />
No<strong>to</strong>riety <strong>to</strong> medical advances came<br />
about, this time when the parents <strong>of</strong> xyphopagous<br />
sisters asked the distinguished<br />
surgeon <strong>of</strong> the times Alvaro Ramos, <strong>to</strong><br />
separate them (Figure 5). Realizing that<br />
this was a major undertaking, Dr. Ramos<br />
requested four “narcotiza-dores” as those<br />
Figure 3: Daguerreotype <strong>of</strong> an amputation just completed on an<br />
apparently asleep injured Mexican soldier. Mexican Military Surgeon<br />
Pedro Van der Linden faces the camera and bayonets <strong>of</strong> <strong>Ameri</strong>can<br />
soldiers about <strong>to</strong> take him and his assistants prisoner.
Figure 4: Dr. Jose Pablo Martinez del Rio<br />
who joined the Mexican forces when hostilities<br />
broke, claimed <strong>to</strong> have received ether and<br />
chlor<strong>of</strong>orm from abroad in early 1847.<br />
experienced on anesthesia were called in<br />
similarity <strong>to</strong> the German term “narcosis”<br />
attributed for anesthesia. In 1899 Rosalina<br />
and Maria underwent chlor<strong>of</strong>orm anesthesia<br />
for the operation. Drs. Miguel Cou<strong>to</strong> and<br />
An<strong>to</strong>nio Leal anesthetized Rosalina, while<br />
Drs. Fajardo and Miguel Pereira <strong>to</strong>ok care<br />
<strong>of</strong> Maria. 11<br />
Recognizing the importance <strong>to</strong> keep<br />
a record <strong>of</strong> changes <strong>of</strong> vital signs during<br />
surgery and anesthesia, a form <strong>of</strong> anesthetic<br />
record was first used in 1903 at the Hospital<br />
da Santa Casa da Misericordia in Rio de<br />
Janeiro on a patient by the name <strong>of</strong> Cristina<br />
da Costa Rezende who received a general<br />
anesthetic with sulphuric ether; there was<br />
no mention <strong>of</strong> who was the surgeon, nor<br />
who the “narcotizer” was, but it did indicate<br />
that the operation had lasted one hour and<br />
13 minutes. 11<br />
The other country where records have<br />
been available was Colombia. Interesting<br />
findings related <strong>to</strong> resuscitative events seem<br />
<strong>to</strong> predate others reported. Records show<br />
that D. Restrepo <strong>of</strong> Medellin, Colombia in<br />
1882 performed the first mouth <strong>to</strong> mouth<br />
respiration on a patient anesthetized with<br />
chlor<strong>of</strong>orm that had s<strong>to</strong>pped breathing, then<br />
proceeded <strong>to</strong> introduce a rubber catheter in<br />
the trachea, alternating mouth <strong>to</strong> tube respirations<br />
with bilateral external compression<br />
<strong>of</strong> the ribs, sternum and epigastrium. 12 The<br />
patient recovered.<br />
In 1891 a senior medical student Teodoro<br />
Castrillon 13 from Bogotá measured the barometric<br />
pressure in Bogotá and estimated the<br />
partial pressure <strong>of</strong> oxygen, noticing that the<br />
former was only 540 mmHg and the latter<br />
108 mmHg; he then proceeded <strong>to</strong> write his<br />
thesis entitled “<strong>Anesthesia</strong> in Altitude”<br />
determining that anesthetics such as ether<br />
and chlor<strong>of</strong>orm should be given with oxygen<br />
or air flow in cities like Bogotá located at<br />
nearly 8000 feet high (2700 m). Later on,<br />
once graduated, Castrillon also described<br />
a case in which he was able <strong>to</strong> electrically<br />
stimulate the phrenic nerves in a patient<br />
that had become apneic under anesthesia<br />
with chlor<strong>of</strong>orm for a “supracondilear”<br />
amputation. The patient breathed during<br />
the apneic period and woke up as the<br />
depth <strong>of</strong> anesthesia was lightened, again<br />
with complete recovery. Also a well-known<br />
anesthetist from Medellin, Luis F. Bernal 12<br />
proposed <strong>to</strong> set up a pro<strong>to</strong>col with the following<br />
steps in case <strong>of</strong> cardiac arrest during<br />
anesthesia:<br />
a) Cease <strong>to</strong> administer the anesthetic<br />
b) Place the patient in a Trendelenburg<br />
position<br />
Figure 5: The xyphopagous sisters Rosalina<br />
and Maria separated in Rio de Janeiro by<br />
surgeon Alvaro Ramos who requested four<br />
“narcotizers” on March 30, 1899 in Sao<br />
Paulo, Brazil: Drs. F. Fajardo and Miguel<br />
Pereira anesthetized Maria and Drs Miguel<br />
Cou<strong>to</strong> and An<strong>to</strong>nio Leao Rosalina with<br />
chlor<strong>of</strong>orm.<br />
c) Reinitiate breathing through a rubber<br />
tube placed in the trachea,<br />
7-10/min<br />
d) Open the left chest and massage<br />
the left ventricle<br />
e) Eliminate the secretions from the<br />
airway<br />
BULLETIN OF ANESTHESIA HISTORY 5<br />
f) Inject stimulants, like caffeine<br />
g) Administer saline solution intravenously.<br />
Undoubtedly this was an advanced pro<strong>to</strong>col<br />
for 1900.<br />
The Birth <strong>of</strong> Intravenous <strong>Anesthesia</strong> by<br />
Infusion<br />
Watching the perilous inductions <strong>of</strong><br />
ether or chlor<strong>of</strong>orm anesthesia in the teaching<br />
hospital “Hospital Juarez”, Miguel<br />
Garcia Marin, a 3 rd year medical student at<br />
the National University <strong>of</strong> Mexico figured<br />
that there had <strong>to</strong> be a better way. He set<br />
up <strong>to</strong> find it. Intravenous administration<br />
<strong>of</strong> fluids was being discussed as possible<br />
treatment for dehydration from diarrheas,<br />
so metal needles were available. He figured<br />
that alcohol, perhaps one <strong>of</strong> the oldest fluids<br />
that put people <strong>to</strong> sleep, could be used<br />
as a drug <strong>to</strong> produce anesthesia so surgery<br />
could be performed. In his own home he<br />
set up a small animal labora<strong>to</strong>ry and began<br />
<strong>to</strong> administer intravenous infusions, using<br />
needles connected <strong>to</strong> a rubber IV tubing<br />
coming from a bifurcated “Y” one attached<br />
<strong>to</strong> a bottle containing 50% alcohol diluted<br />
in 25% glucose and the other 5% dextrose<br />
in distilled water (Figure 6). Early in the<br />
experiments he noted hematuria, which<br />
subsided when he diluted the ethanol in<br />
25% dextrose. He established pro<strong>to</strong>cols <strong>to</strong><br />
administer different rates in<strong>to</strong> 90 doves, 17<br />
hens, 72 dogs, 8 turkeys and eventually two<br />
monkeys ( Figure 7) while measuring vital<br />
signs, urine output and any other event. 14<br />
He determined the required flow rates <strong>to</strong><br />
produce sedation, light anesthesia and pr<strong>of</strong>ound<br />
level <strong>of</strong> anesthesia. Eventually when<br />
Garcia Marin was on the fifth (last) year <strong>of</strong><br />
medical school, through the recommendation<br />
<strong>of</strong> one <strong>of</strong> his pr<strong>of</strong>essors Dr. Ulrich and<br />
his uncle who was a representative in the<br />
Mexican Congress, he was allowed <strong>to</strong> give<br />
a demonstration on a volunteer, but only a<br />
prisoner from the Lecumberri Penitenciary,<br />
who had a death sentence, was willing. With<br />
the promise <strong>of</strong> an indult if he survived, he<br />
agreed <strong>to</strong> undergo the test with IV alcohol.<br />
The young student demonstrated his abilities<br />
and the judge let the surviving prisoner<br />
go free.<br />
Next, Garcia Marin went on <strong>to</strong> give 53<br />
anesthetics for major surgical procedures<br />
(Figure 8) while studying the effects <strong>of</strong> IV<br />
alcohol on renal and hepatic functions as<br />
well as on the vital signs. 15 Moreover, by<br />
securing an intravenous line <strong>to</strong> administer<br />
Continued on next page
6 BULLETIN OF ANESTHESIA HISTORY<br />
<strong>Contributions</strong>. . .Continued from page 5<br />
Figure 6: Schematic representation <strong>of</strong> the IV pole with two<br />
bottles connected <strong>to</strong> a bifurcated “Y” line and in<strong>to</strong> a single<br />
rubber tubing, a s<strong>to</strong>pcock attached <strong>to</strong> the needle for infusion<br />
<strong>of</strong> alcohol by Garcia Marin.<br />
the alcohol, it became evident that it was<br />
helpful <strong>to</strong> administer intravenous fluids and<br />
<strong>to</strong> have rapid access <strong>to</strong> the circulation for the<br />
administration <strong>of</strong> resuscitative medications.<br />
From his initial experience he learned the<br />
value <strong>of</strong> giving atropine and morphine IM<br />
as premedication that made the induction<br />
smoother; he also determined the dose <strong>of</strong><br />
indifference <strong>to</strong> be1 ml/kg and <strong>to</strong> achieve<br />
anesthesia patients usually required 2 <strong>to</strong> 3<br />
ml/kg. From the observations in animals he<br />
determined the lethal dose <strong>to</strong> be 5 <strong>to</strong> 6 ml/<br />
kg <strong>of</strong> the above noted solution. For patients<br />
he mixed 40ml <strong>of</strong> 96 pro<strong>of</strong> alcohol in 40ml<br />
<strong>of</strong> 25% dextrose in water, alternating with<br />
the flow <strong>of</strong> the other bottle that contained<br />
5% dextrose in water.<br />
Through his influential uncle the recent<br />
graduate received a government grant <strong>to</strong><br />
travel abroad. He chose <strong>to</strong> go <strong>to</strong> London and<br />
Paris where he demonstrated his technique,<br />
most <strong>of</strong> the time successfully. Eventually<br />
the young physician returned <strong>to</strong> Mexico in<br />
1931 <strong>to</strong> find his technique in the midst <strong>of</strong> a<br />
bitter controversy. 16 A few months after receiving<br />
a medal <strong>of</strong> praise from the Mexican<br />
Congress, Luis Garcia Marin found himself<br />
in the midst <strong>of</strong> a turbulent debate, which<br />
ended with one <strong>of</strong> the least wise decision<br />
that the Mexican Academy <strong>of</strong> Surgery has<br />
ever handed down which banned Intravenous<br />
<strong>Anesthesia</strong> with Alcohol because<br />
it produced thrombophlebitis. Although<br />
alcohol at the concentrations used by Garcia<br />
Marin has the potential <strong>to</strong> produce irritation<br />
<strong>of</strong> the veins endothelium, one can not<br />
help but <strong>to</strong> think, what a waste <strong>of</strong> talent;<br />
if he would have been encouraged <strong>to</strong> learn<br />
other anesthesia techniques or <strong>to</strong> improve<br />
his approach, instead <strong>of</strong> running him out <strong>of</strong><br />
<strong>to</strong>wn, his experience acquired before the age<br />
<strong>of</strong> 33 years could have been<br />
very valuable as intravenous<br />
anesthesia with thiopental<br />
and other agents was about<br />
<strong>to</strong> be introduced.<br />
Peridural <strong>Anesthesia</strong><br />
Next, a phase <strong>of</strong> fascination<br />
with regional anesthesia,<br />
more specifically with<br />
peridural anesthesia as it is<br />
called in most <strong>of</strong> the Spanish<br />
speaking countries based<br />
on the fact that the so called<br />
epidural space surrounds the<br />
dural sac brought about a<br />
series <strong>of</strong> observations on this<br />
anesthetic technique. The<br />
most recognized contribu<strong>to</strong>r<br />
was Alber<strong>to</strong> Gutierrez (Figure<br />
9), an accomplished surgeon<br />
Figure 7: Table listing the experiments done in<br />
animals by Miguel Garcia Marin in 1928 who<br />
administered IV alcohol <strong>to</strong> 90 doves, 17 hens, 8<br />
turkeys, 72 dogs. The concentration <strong>of</strong> alcohol<br />
used, the dosages, mixtures with hyper<strong>to</strong>nic<br />
(25%) glucose are shown. The number <strong>of</strong> deaths<br />
and unsatisfac<strong>to</strong>ry anesthetics are depicted, as<br />
well as the numbers <strong>of</strong> dogs in whom observation<br />
on respiration, circulation and renal function<br />
were made.<br />
from Buenos Aires, who taught Ana<strong>to</strong>my<br />
at the University; as many other surgeons<br />
like Bier, Matas, Crile, etc. let their curiosity<br />
lead them <strong>to</strong> the obvious mystery over<br />
which they frequently had <strong>to</strong> depend on<br />
others, pain and anesthesia. In his earlier<br />
pr<strong>of</strong>essional years as a surgeon along with<br />
surgical themes, he wrote on approaches <strong>to</strong><br />
the brachial plexus, “splanchnic anesthesia”,<br />
local anesthesia for biliary surgery,<br />
and ablation <strong>of</strong> the II and III divisions <strong>of</strong><br />
the trigeminal nerve, calcaneous spurs and<br />
local anesthesia for abdominal surgery. In<br />
the early 1930’s he began <strong>to</strong> give anesthesia<br />
for his own operations following Pages and<br />
Dogliotti’s technique. 17,18<br />
Realizing that sometimes the “loss <strong>of</strong><br />
resistance approach” was misleading or<br />
not easy <strong>to</strong> locate precisely where the epidural<br />
space (ES) was he decided <strong>to</strong> look for<br />
another method. Based on his expertise in<br />
ana<strong>to</strong>my he explored the precise<br />
identification <strong>of</strong> the negative<br />
pressure in the epidural<br />
compartment. By introducing<br />
the needle tip very slowly, he<br />
punctured first the peridural<br />
space, injected about 4/5 <strong>of</strong><br />
the dose and then continued<br />
<strong>to</strong> advance the needle in<strong>to</strong> the<br />
subarachnoid space where he<br />
injected the remaining 1/5.<br />
He then reversed the order,<br />
injecting in<strong>to</strong> the intrathecal<br />
space first, and then gradually<br />
withdrew the needle until the<br />
flow <strong>of</strong> CSF s<strong>to</strong>pped, there he<br />
injected the respective dosage<br />
<strong>of</strong> anesthetic. So he developed<br />
a precise skill <strong>to</strong> identify one or<br />
the other space at will. Then<br />
conceived the idea <strong>of</strong> advancing<br />
the needle with a drop hanging<br />
from the hub through the ligamentum<br />
flavum and watching<br />
it get “sucked” as the peridural<br />
space was entered. 20<br />
So the “hanging drop”<br />
method was created (Figure<br />
10) and in a way the Combined<br />
Spinal-Epidural technique<br />
with one needle was also designed.<br />
Even <strong>to</strong>day, many<br />
colleagues consider it <strong>to</strong> be<br />
the safest approach <strong>to</strong> identify<br />
the ES, although it requires<br />
precision and skill. Gradually<br />
his interest shifted <strong>to</strong>ward anesthesia,<br />
though he continued<br />
<strong>to</strong> have a busy surgical practice,<br />
Gutierrez went on <strong>to</strong> report<br />
large series <strong>of</strong> cases <strong>to</strong>taling<br />
over 12000 epidural anesthetics
Figure 8: Specimen <strong>of</strong> a hip desarticulation performed by<br />
Dr. E. Ulrich under general anesthesia with intravenous<br />
alcohol administered by Miguel Garcia Marin.<br />
that he himself performed 21 and operated on<br />
most <strong>of</strong> the patients, <strong>to</strong>o. In the process,<br />
he compared different local anesthetics,<br />
though he preferred procaine 2%. He also<br />
measured the negative pressure in the ES,<br />
Figure 9: Dr.Alber<strong>to</strong> Gutierrez, a surgeon<br />
intrigued by epidural anesthesia conducted<br />
numerous observations on the <strong>to</strong>pic and<br />
founded the first anesthesia journal in <strong>Latin</strong><br />
<strong>Ameri</strong>ca (1939).<br />
as well as the difference at the thoracic and<br />
lumbar levels and determined the distance<br />
from the skin <strong>to</strong> the point at which the<br />
ligamentum flavum was penetrated in over<br />
2000 cases noting than in 90% <strong>of</strong> patients it<br />
was shorter than 6 cm. Other observations<br />
made by Gutierrez included the gradual<br />
progression <strong>of</strong> the onset <strong>of</strong> sensory and mo<strong>to</strong>r<br />
blockade, as well as the demonstration<br />
that epidurally injected procaine was found<br />
in the subarachnoid space 2 <strong>to</strong> 4 hours later.<br />
He also developed a simple but effective<br />
device (Figure 11) <strong>to</strong> accomplish infiltration<br />
<strong>of</strong> local anesthetics, rapidly, for major<br />
surgery. 22 With other collabora<strong>to</strong>rs,<br />
he founded the first<br />
anesthesia journal in <strong>Latin</strong><br />
<strong>Ameri</strong>ca; the Revista Argentina<br />
de Anestesia y Analgesia<br />
which has been published<br />
since 1939, until <strong>to</strong>day with<br />
the new title <strong>of</strong> Revista Argentina<br />
de Anestesiologia. It<br />
is worth mentioning that the<br />
first issue had abstracts <strong>of</strong> the<br />
articles published in English,<br />
German, French and Italian<br />
languages with international<br />
edi<strong>to</strong>rs and plenty <strong>of</strong> advertisements.<br />
In his edi<strong>to</strong>rial<br />
Pr<strong>of</strong>essor Alber<strong>to</strong> Gutierrez 23 addressed the<br />
ever-present issue “On the relationship between<br />
the anesthesiologist and the surgeon”;<br />
he remained edi<strong>to</strong>r <strong>of</strong> the Revista until his<br />
death in 1945.<br />
Several <strong>of</strong> Gutierrez disciples <strong>to</strong>ok <strong>to</strong><br />
epidural anesthesia and increased its popularity<br />
in South <strong>Ameri</strong>ca. One, Vicente Ruiz<br />
also worked in the Spanish Hospital and was<br />
a ”hanging drop “ fan 24 ; in 1939 he wrote a<br />
report <strong>of</strong> 3,826 cases performed by himself<br />
that was published in the journal Minnesota<br />
Medicine. 25 Other anesthetists became<br />
enchanted with the technique; Ontaneda 26<br />
in 1933,also from Buenos Aires, measured<br />
more exactly the negative pressure in the<br />
epidural space using an aneroid manometer<br />
determining a range from –3 cm H20 distally<br />
<strong>to</strong> –9 cm H2O at the mid-thoracic spine.<br />
Murillo Braga from São Paulo, Brazil 11<br />
noted that the first sign <strong>of</strong> the onset <strong>of</strong><br />
epidural anesthesia was fasciculation <strong>of</strong><br />
the latissimus dorsi muscle<br />
occurring 2 <strong>to</strong> 3 minutes after<br />
the injection <strong>of</strong> the anesthetic<br />
which were attributed <strong>to</strong> the<br />
cold fluid injected in<strong>to</strong> the<br />
epidural compartment.<br />
A fascinating description <strong>of</strong><br />
a balloon adapted <strong>to</strong> a threeway<br />
s<strong>to</strong>pcock and connected<br />
<strong>to</strong> the hub <strong>of</strong> the needle was<br />
described by De Souza 27 from<br />
Rio de Janeiro in 1943. Thus,<br />
preceding the McIn<strong>to</strong>sh balloon<br />
by about 7 years. 28 The<br />
balloon was supposed <strong>to</strong> deflate<br />
immediately upon entry<br />
<strong>of</strong> the needle’s bevel in<strong>to</strong> the<br />
ES.<br />
With the same pursuit,<br />
Almeida (11) from Sao Paulo in 1945 adapted<br />
a tight rubber band <strong>to</strong> the plunger <strong>of</strong> the<br />
syringe that contained saline solution; the<br />
plunger was advanced promptly as the tip<br />
<strong>of</strong> the needle entered the peridural compartment.<br />
Another surgeon from the same city,<br />
BULLETIN OF ANESTHESIA HISTORY 7<br />
Figure 10: The hanging drop method designed<br />
by Gutierrez on his own needle that allowed it<br />
<strong>to</strong> be advanced gradually with the thumb and<br />
the index finger <strong>of</strong> both hands.<br />
Edmundo Vasconcelos ( 29) reported in 1944<br />
a large series <strong>of</strong> thoracic operations including<br />
esophagec<strong>to</strong>mies, pneumonec<strong>to</strong>mies,<br />
lobec<strong>to</strong>mies and thoracoplasties mostly for<br />
patients with tuberculosis, under thoracic<br />
epidural anesthesia.<br />
As the complexity <strong>of</strong> the operations<br />
demanded longer periods <strong>of</strong> anesthesia,<br />
Lemmon 30 designed the continuous spinal<br />
anesthesia using a malleable needle that<br />
required special mattresses <strong>to</strong> accommodate<br />
it. Miguel Martinez Curbelo from La<br />
Havana, Cuba, in 1945 first introduced a<br />
ureteral catheter in<strong>to</strong> the lumbar ES for<br />
prolonged operations with repeated dosing<br />
with procaine. Eventually he was invited<br />
by Lundy <strong>to</strong> the Mayo Clinic in Rochester<br />
MN where he was able <strong>to</strong> demonstrate his<br />
method culminating with a publication in<br />
<strong>Anesthesia</strong> and Analgesia in 1949. 31<br />
Figure 11: Apparatus designed by Gutierrez <strong>to</strong> load and<br />
reload rapidly a syringe for infiltration or nerve block<br />
anesthesia.<br />
With the ever present desire <strong>to</strong> find<br />
easier approaches <strong>to</strong> identify the ES, Juan<br />
Nesi 32 from Buenos Aires and later in Caracas<br />
described the technique <strong>of</strong> the “bubble<br />
in the syringe” in 1958. He noted that the<br />
Continued on next page
8 BULLETIN OF ANESTHESIA HISTORY<br />
<strong>Contributions</strong>. . .Continued from page 7<br />
shape <strong>of</strong> a small bubble in a syringe containing<br />
fluid will change its shape when pressure<br />
is exerted on the plunger and the tip <strong>of</strong> the<br />
needle is in the ligamentum flavum, but the<br />
fluid will leave the syringe without changing<br />
the shape <strong>of</strong> the bubble as soon as the bevel<br />
was in the ES (Figure 12). Bus<strong>to</strong>s 33 , also<br />
from Buenos Aires, in 1964 described the<br />
“sign <strong>of</strong> the foam” <strong>to</strong> the joint return <strong>of</strong> bubbles<br />
and fluid appearing at the hub <strong>of</strong> the<br />
needle when the bevel was in the ES, after<br />
the fluid in the loss <strong>of</strong> resistance syringe had<br />
been injected. Plaza Quijada 34 from Caracas,<br />
in 1967 reproduced the same sign <strong>of</strong> the<br />
foam but coming through the proximal end<br />
<strong>of</strong> the catheter that had been placed in the<br />
ES after the test dose was given. That same<br />
year, Ricardo Sanchez and co-workers 35 from<br />
the IMSS in Mexico observed the direction<br />
taken by lumbar epidural catheters when<br />
advanced 20 cms cephalad. Injecting a small<br />
amount <strong>of</strong> contrast media, they noted that<br />
48% followed a cephalad direction, 33%<br />
curled up, 12% bent over and went caudad<br />
and the remaining 6% left the spinal canal<br />
through one <strong>of</strong> the lateral foramen. These<br />
observations confirmed the unwritten rule<br />
<strong>of</strong> not inserting catheters more than 4 cm<br />
otherwise no one can predict where they will<br />
end up. Llerena 36 also from Mexico City in<br />
1969, ingeniously described an alternative <strong>to</strong><br />
identify the ES without a syringe by inserting,<br />
in<strong>to</strong> the hub <strong>of</strong> a needle the distal tip <strong>of</strong><br />
an intravenous fluid line, curled in<strong>to</strong> a role<br />
and fixed with a plastic tie so as <strong>to</strong> leave<br />
the proximal end vertically upward. Partly<br />
filled with saline, the tip was attached <strong>to</strong> the<br />
hub, the needle is advanced gradually and<br />
the column <strong>of</strong> saline fell as soon as the tip<br />
<strong>of</strong> the needle entered the ES.<br />
In the absence <strong>of</strong> a “glucostix strip”, Andrade-Marcano<br />
37 from Maracay, Venezuela<br />
in 1969 suggested <strong>to</strong> aspirate with a syringe<br />
whatever fluid came out <strong>of</strong> the needle and<br />
inject it intradermically; if it produced<br />
numbness it was local anesthetic, if not, it<br />
most likely was CSF. The same author 38 in<br />
1972 measured the changes in ES pressure<br />
that occurred with changes <strong>of</strong> position (sitting<br />
up, supine, flexion and extension <strong>of</strong> the<br />
spine). In 1971, Castaños y Sagarnaga 39 from<br />
La Paz, Bolivia, auscultated, recorded and<br />
amplified the click heard at the moment <strong>of</strong><br />
penetration <strong>of</strong> the ligamentum flavum as a<br />
needle entered the ES. Anibal Galindo et<br />
al 40 , then in Bogotá, in 1975 correlated the<br />
derma<strong>to</strong>mal onset <strong>of</strong> epidural anesthesia<br />
with the diameter <strong>of</strong> the corresponding<br />
sacral nerve root, demonstrating that the<br />
thickest root S1 had the longest onset.<br />
In the late 50s, Jose Usubiaga a young,<br />
Figure 12: Schematic representation <strong>of</strong> the sign <strong>of</strong> the<br />
“bubble” in a syringe method <strong>to</strong> find the epidural space<br />
described by Juan Nesi.<br />
brilliant anesthesiologist from Buenos Aires<br />
assembled a group <strong>of</strong> investiga<strong>to</strong>rs that<br />
conducted a variety <strong>of</strong> remarkable clinical<br />
studies including the treatment <strong>of</strong> postdural<br />
puncture headache with large volumes <strong>of</strong><br />
epidural saline 41 , quantified the transfer<br />
<strong>of</strong> local anesthetics across the placenta 42<br />
and from the peridural <strong>to</strong> the intrathecal<br />
space 43 ; Wikinski, Usubiaga and Morales<br />
also described the mechanism for the appearance<br />
<strong>of</strong> convulsions from excessive<br />
dosages <strong>of</strong> local anesthetics in man. 44 With<br />
great interest on regional anesthesia Jose<br />
also wrote the most extensive review <strong>of</strong> the<br />
complications <strong>of</strong> epidural anesthesia 45 as a<br />
warning for improvement in the technique.<br />
Regional <strong>Anesthesia</strong><br />
In the meantime other advances were<br />
taking place in other aspects <strong>of</strong> Regional<br />
<strong>Anesthesia</strong>. In 1931, the same Miguel<br />
Martinez Curbelo 46 in la Havana performed<br />
a series <strong>of</strong> supraclavicular blocks <strong>of</strong> the<br />
brachial plexus, with patients in the sitting<br />
position (Figure 13); in this position, the<br />
shoulder drops making the nerve trunks<br />
more superficial and the lung more distant,<br />
allowing easier access <strong>to</strong> the perineurovascular<br />
sheath. In 1939 Alfonso Albanes 47<br />
from Rosario, Argentina treated a number<br />
<strong>of</strong> patients that had shoulder<br />
arthritis with repeated blocks<br />
<strong>of</strong> the cervicothoracic sympathetic<br />
ganglion. Ber<strong>to</strong>la 48<br />
modified the interpleural block<br />
for biliary surgery, injecting the<br />
local anesthetic in the thoracic<br />
paravertebral compartment<br />
demonstrating the parallel continuity<br />
<strong>of</strong> the retrocostal space<br />
along the spine using a radio<br />
opaque resin <strong>to</strong> demonstrate it<br />
(Figure 14).<br />
Though Bier’s technique <strong>of</strong><br />
intravenous regional anesthesia<br />
(IVA) 49 was introduced in<br />
1908, after a certain period <strong>of</strong><br />
popularity it had fallen in<strong>to</strong> inertia, until<br />
1945 when Luis Garcia Herreros, a Mexican<br />
Military physician reported 104 cases<br />
<strong>of</strong> upper and lower extremity blocks using<br />
procaine and tetracaine without apparent<br />
complications. 50 Enzo Mourigan Canale 51<br />
from Montevideo in 1946 described 55<br />
cases treated with 0.5% procaine and in<br />
1954, Flavio Kroeff Pires from Por<strong>to</strong> Alegre,<br />
Brazil proposed <strong>to</strong> re-inflate and deflate the<br />
cuff repeatedly <strong>to</strong> prevent complications at<br />
the end <strong>of</strong> the procedure 52 preceding the<br />
usually quoted publication in English. 53<br />
Zerkinatti 54 in 1972 proposed the use <strong>of</strong> a<br />
double cuff <strong>to</strong> prevent the pain from the one<br />
single <strong>to</strong>urniquet. Subsequently, Almiro Dos<br />
Reies from São Paulo studied extensively<br />
this technique, describing the effects <strong>of</strong><br />
ischemia and the pharmacokinetics and<br />
pharmacodynamics <strong>of</strong> several local anesthetics<br />
55 ; he also published a comprehensive<br />
monograph on IRA 56 followed by another on<br />
the proper use <strong>of</strong> limb <strong>to</strong>urniquets and their<br />
possible complications. 57 The first application<br />
<strong>of</strong> epidural blood patch was reported<br />
by Gormley 58 in three patients that had<br />
developed post dural puncture headache<br />
in 1960. Soon thereafter, Edgar Martinez<br />
Aguirre 59 from Caracas reported a series <strong>of</strong><br />
100 patients that developed<br />
this complication with high<br />
rate <strong>of</strong> success. Spiegel from<br />
Rio de Janeiro 60 , Baquero y<br />
Vasquez from Mexico City 61<br />
and Fortuna from San<strong>to</strong>s 62<br />
published their experience<br />
with caudal anesthesia in<br />
children in the 60’s; Estela<br />
Melman and her group 63 published<br />
a large series <strong>of</strong> epidural<br />
and regional blocks in infants<br />
Figure 13: Supraclavicular<br />
brachial plexus block on a sitting<br />
patient by Miguel Martinez<br />
Curbelo.
and children in 1975 though they seldom<br />
receive recognition in pediatric regional<br />
anesthesia reviews. 64<br />
Since then this technique has been used<br />
in millions <strong>of</strong> patients.<br />
In 1989 Jorge Barrios-Alarcon et al 65 ,<br />
from São Paulo, Brazil proposed the alternative<br />
use <strong>of</strong> dextran 40 for the treatment<br />
<strong>of</strong> PDPH with a similar rate <strong>of</strong> success<br />
and without the potential hazards <strong>of</strong> the<br />
injection <strong>of</strong> au<strong>to</strong>logous blood in <strong>to</strong> the ES.<br />
Castaños et al 66 also showed that hemodilution<br />
and epidural anesthesia would reduce<br />
the blood viscosity and increased the PaO2<br />
<strong>of</strong> patients having hema<strong>to</strong>crit levels above<br />
70% in La Paz, Bolivia, at 14,000 feet high.<br />
Alber<strong>to</strong> Torrieri from Buenos Aires et<br />
Figure 14: Multiple paravertebral nerve block approached<br />
retrocostally <strong>to</strong> allow cholecystec<strong>to</strong>my and biliary surgery.<br />
al 67 described the first single-double lumen<br />
needle (Figure 15) used <strong>to</strong> provide Combined<br />
spinal-epidural anesthesia <strong>to</strong> patients<br />
undergoing major orthopedic procedures.<br />
Ricardo Plancarte et al 68 from Mexico City<br />
demonstrated in 1989, the feasibility and<br />
effectiveness <strong>of</strong> performing the superior<br />
hypogastric plexus block for the treatment<br />
<strong>of</strong> severe chronic pelvic pain. A year later,<br />
the same group 69 described the approach <strong>to</strong><br />
block the ganglion <strong>of</strong> Whar<strong>to</strong>n (impar) for<br />
the treatment <strong>of</strong> intractable perineal pain.<br />
Other related contributions have explained<br />
unilateral epidural blocks by the misplacement<br />
<strong>of</strong> catheters 70 and the application <strong>of</strong><br />
peridural anesthesia in Bernard-Horner<br />
syndrome. 71<br />
Other <strong>Contributions</strong><br />
Luis Agote 72 described in Buenos Aires<br />
the technique <strong>of</strong> clotting prevention by a<br />
precisely titrated dosification <strong>of</strong> Na citrate<br />
facilitating the development <strong>of</strong> blood banking<br />
making blood transfusions available<br />
<strong>to</strong> every one that needed them. On what<br />
appears <strong>to</strong> be the premier recommendation<br />
for moment <strong>to</strong> moment moni<strong>to</strong>ring <strong>of</strong><br />
patients under anesthesia, the picturesque<br />
and flamboyant Juan Marin from Bogotá<br />
Colombia, in 1934 insisted that the precordial<br />
stethoscope should be used <strong>to</strong> listen<br />
continuously <strong>to</strong> the heart and lung sounds<br />
<strong>of</strong> pediatric patients undergoing anesthesia<br />
so “cardiac arrhythmias and cardiac arrest<br />
can be identified as they happen.” 73<br />
Jose C. Delorme assembled the first<br />
anesthesia machine built in Argentina that<br />
included vaporizers for ether, chlor<strong>of</strong>orm<br />
and ethyl chloride and tanks for oxygen and<br />
CO2 as well as a soda lime absorber used for<br />
the first time in the Italian Hospital in Buenos<br />
Aires in late 1934. 74 Later on, Kentaro<br />
Takaoka 75 from São Paulo, Brazil designed<br />
the portable Takaoka ventila<strong>to</strong>r that could<br />
be held in one hand; it was used extensively<br />
as anesthesiologists went from<br />
clinic <strong>to</strong> clinic <strong>to</strong> give anesthetics,<br />
for resuscitation and<br />
even prolonged mechanical<br />
ventilation. The same author<br />
developed an universal ventila<strong>to</strong>r<br />
that could be used for all<br />
inhalation anesthetics available<br />
in 1965 76 and a breathing<br />
anesthetic circuit that could<br />
be used for children and<br />
adults in 1968 77 predating the<br />
Bain 78 circle by over a decade.<br />
The Takaoka family has expanded<br />
as manufacturer <strong>of</strong><br />
equipment from incuba<strong>to</strong>rs,<br />
<strong>to</strong> ventila<strong>to</strong>rs, <strong>to</strong> anesthetic<br />
machines and everything else<br />
in between providing reliable equipment,<br />
instruction and maintenance, at reasonable<br />
cost for nearly 50 years.<br />
In 1949, Aranes and Blusque Castellanos<br />
added intermittent boluses <strong>of</strong> thiopental and<br />
meperidine <strong>to</strong> an intravenous infusion <strong>of</strong><br />
procaine 79 creating another attempt <strong>to</strong> <strong>to</strong>tal<br />
intravenous anesthesia. This work was presented<br />
at the 1 st <strong>Latin</strong> <strong>Ameri</strong>can Congress<br />
Figure 15: Distal portion <strong>of</strong> the Torrieri-Aldrete double<br />
lumen needle for Combined Spinal-Epidural <strong>Anesthesia</strong><br />
(1984).<br />
BULLETIN OF ANESTHESIA HISTORY 9<br />
<strong>of</strong> Anesthesiology in Buenos Aires, at what<br />
turned out <strong>to</strong> be the first true international<br />
congress in Anesthesiology preceding the<br />
Paris International Congress held in 1951.<br />
Two novel ideas were proposed at that meeting<br />
a “consultation room” and a “recovery<br />
room.” Later on Wikinski et al 80 studied the<br />
pharmacokinetics and pharmacodynamics<br />
<strong>of</strong> procaine IV and related them <strong>to</strong> the levels<br />
<strong>of</strong> anesthesia obtained. This technique<br />
became very popular in Argentina and other<br />
South <strong>Ameri</strong>can countries where millions<br />
<strong>of</strong> anesthetics were administered with<br />
“Procaine a la Argentine,” until the 1980s<br />
when fluorinated hydrocarbon anesthetics<br />
were introduced. It is worth mentioning that<br />
only one case <strong>of</strong> malignant hyperthermia<br />
was reported during this period. R. Caldero-<br />
Barcia and his associates 81 in the Hospital de<br />
Clinicas in Montevideo studied the physiology<br />
<strong>of</strong> uterine contractions by cannulating<br />
the uterine cavity and vessels <strong>of</strong> mothers in<br />
labor. They also observed the effects <strong>of</strong> regional<br />
anesthesia and magnesium sulfate on<br />
uterine contractility as well as on maternal<br />
and neonatal vital signs (Figure 16).<br />
The Postanesthetic Recovery Score first<br />
proposed in 1970 82 , in its original form or<br />
in one <strong>of</strong> its modifications has become the<br />
standard <strong>of</strong> care in nearly all <strong>of</strong> the <strong>Ameri</strong>can<br />
continent and other countries in establishing<br />
the physical condition <strong>of</strong> patients<br />
recovering from anesthesia and surgery as<br />
well as their discharge eligibility.<br />
Preoccupation with the prevention <strong>of</strong> the<br />
undesirable effects from ketamine, as well<br />
as unconventional indications have motivated<br />
a number <strong>of</strong> investigations. Albin<br />
et al 83 prevented the psychogenic disturbances<br />
with tetrahy-droamiquidinic acid<br />
(THA), while Martinez Aguirre claimed <strong>to</strong><br />
reverse them with 4-aminopiridine 84 ; the<br />
same group 85 demonstrated that ketamine<br />
produced adequate analgesia and muscle<br />
relaxation when used with<br />
the technique <strong>of</strong> regional IV<br />
anesthesia and Jose Islas et<br />
al 86 demonstrated the central<br />
analgesic effects <strong>of</strong> ketamine<br />
when administered by the<br />
epidural route <strong>to</strong> patients in<br />
the pos<strong>to</strong>perative period.<br />
On a similar vein, A. Oswaldo<br />
Auad 87 , from Buenos<br />
Aires, showed in 1985 that<br />
epidural clonidine potentiated<br />
morphine analgesia in<br />
the treatment <strong>of</strong> patients with<br />
recalcitrant chronic pain.<br />
Del Castillo and Katz described<br />
the location and expanded<br />
the understanding <strong>of</strong><br />
Continued on next page
10 BULLETIN OF ANESTHESIA HISTORY<br />
<strong>Contributions</strong>. . .Continued from page 9<br />
Figure 16: Moni<strong>to</strong>r tracing <strong>of</strong> the effects <strong>of</strong> 2 gm <strong>of</strong> MgSO4<br />
on intrauterine pressure, intensity and frequency <strong>of</strong> contraction<br />
and on arterial blood pressure obtained by Caldero Barcia<br />
(circa 1958).<br />
the acetylcholine recep<strong>to</strong>rs 88 , Usubiaga et<br />
al 89 described the interaction <strong>of</strong> neuromuscular<br />
relaxants drugs and local anesthetic<br />
agents in 1965. First Galindo 90 in 1974, then<br />
Kennedy and Galindo 91 suggested the concept<br />
<strong>of</strong> presensitiz-ation with non-depolarizing<br />
agents before giving succinyl-cholina<br />
and later and later Kelly and collabora<strong>to</strong>rs 92,<br />
93<br />
confirmed some <strong>of</strong> their interactions<br />
with inhalation and intravenous anesthetic<br />
agents.<br />
Undoubtedly there are other contributions<br />
from <strong>Latin</strong> <strong>Ameri</strong>can physicians <strong>to</strong><br />
<strong>Anesthesia</strong>, but for the reasons already mentioned<br />
they might not have been recorded<br />
or by being published in obscure periodicals<br />
or because the authors were not properly<br />
listed, they remained unknown. Our intent<br />
has been <strong>to</strong> include those aportations that<br />
<strong>to</strong> our knowledge could be documented and<br />
that in our understanding, were innovative<br />
at the time <strong>of</strong> publication or presentation<br />
at meetings. If any has been omitted, it was<br />
certainly not intentional, though we accept<br />
responsibility for the data; it is also feasible,<br />
as it has occurred for centuries that the same<br />
innovation might have been presented prior<br />
or simultaneously by another author. Our<br />
anticipated apologies for such not purposed<br />
oversight. This is a recognized hazard and a<br />
challenge in his<strong>to</strong>ry <strong>of</strong> Medicine research.<br />
So we recognize that this data is subject <strong>to</strong><br />
corrections and changes as more is known<br />
about these fascinating and exciting times<br />
in <strong>Anesthesia</strong>. May this manuscript be a<br />
stimulating curiosity for future generations<br />
<strong>of</strong> anesthesiologists interested <strong>to</strong> search for<br />
their roots since finding about our past allows<br />
us <strong>to</strong> learn more about ourselves. We<br />
hope that this review may also serve as an<br />
inspiration for those with new ideas, willing<br />
<strong>to</strong> apply them for the benefit <strong>of</strong> all patients.<br />
References 1. Bigelow HJ: Insensitivity<br />
during surgical operations<br />
produced by inhalation. Bos<strong>to</strong>n<br />
Med Surg J 1846, 35:309-317.<br />
2. Sykes WS: Essays on<br />
the first hundred years <strong>of</strong><br />
anaesthesia. R.H. Ellis (ed),<br />
Edinburgh; E S Livings<strong>to</strong>ne,<br />
Ltd 1961, vol 1.<br />
3. Snow J: On the inhalation<br />
<strong>of</strong> chlor<strong>of</strong>orm and ether.<br />
Lancet 1848, I:177-180.<br />
4. Pirog<strong>of</strong>f, Nikolai Ivanovich<br />
in Foundations <strong>of</strong> Anesthesiology<br />
A. Faulconer Jr and<br />
T.E. Keys (eds) C.C. Thomas,<br />
Springfield 1965: pp. ;725-727.<br />
5. Aldrete JA, Marron GA,<br />
Wright AJ: The first administration<br />
<strong>of</strong> anesthesia in military<br />
surgery. On occasion <strong>of</strong> the<br />
Mexican-<strong>Ameri</strong>can War. Anesthesiology<br />
1984, 61:585-588.<br />
6. Porter J: Surgical notes<br />
on the Mexican War. Amer J <strong>of</strong><br />
Med Sci 1852, vol 23.<br />
7. Alcantara-Herrera J: Anotaciones his<strong>to</strong>ricas<br />
con motivo del primer centenario de anesthesia por<br />
el éter y clor<strong>of</strong>ormo. Medicina 1946, 26.<br />
8. Fernandez del Castillo F: ¿Cuando y por quilen<br />
se aplicó por primera vez en Mexico la anestesia por<br />
inhalación Gaceta Medica, Mexico 1947:58:265.<br />
9. Panorama Histórico de la Medicina en México.<br />
(1. a ed.). México: Edi<strong>to</strong>rial Talleres de la Nación<br />
1985:2.<br />
10. Pereira P: Reseçsão de tumor mandibular.<br />
Gaceta Médica da Bahía, 1866.<br />
11. Meira DG: Origens e evolução da anestesiologia<br />
brasileira. Gráfica Edi<strong>to</strong>ra da Arte Moderno,<br />
Río de Janeiro, 1981.<br />
12. Alvarez T: Anotaciones para una his<strong>to</strong>ria de la<br />
Anestesia y Reanimación in Colombia. Universidad<br />
de Antioquia, Medellin, 1984.<br />
13. Castrillón T: Contribución al estudio de la<br />
anestesia en las alturas. Contraindicacion del clor<strong>of</strong>ormo<br />
en la altiplanicie de Bogotá (tesis pr<strong>of</strong>essional).<br />
Universidad de Santa Fé, Bogotá, Colombia, 1891.<br />
14. Aldrete JA, Aldrete-Velasco J: The use <strong>of</strong><br />
alcohol for anesthesia by Miguel Garcia Marin. In<br />
Anaesthesia Essays on its His<strong>to</strong>ry: J Rupreth, JD<br />
Van Lieburg, JA Lee and W. Erdman (eds) Springer<br />
Verlag, Berlin-Heidelberg, 1985:pp79-87.<br />
15. García Marín M: Anestesia con alcol intravenoso.<br />
Tesis Pr<strong>of</strong>essional, Universidad Nacional<br />
Autónoma de México, 1929.<br />
16. Aldrete JA: Una contribución original: Anestesia<br />
por alcol endovenoso por Miguel García-Marín.<br />
Rev. Mex. Anestesiol 1985, 8:169-174.<br />
17. Gutiérrez A. Anestesia metamérica epidural.<br />
Rev Cirugía Buenos Aires 1932, 1:665-685.<br />
18. Gutiérrez A, Lopez-Rubido M: Resultados<br />
obtenidos con la anesthesia peridural. Rev Cirugía<br />
Buenos Aires 1933, 12:93-101.<br />
19. Gutiérrez A: Anestesia extradural. Revista<br />
de Cirugía de Buenos Aires 1939, 16:52-58.<br />
20. Gutiérrez A: Valor de la aspiración líquida en<br />
el espacio peridural en la anestesia peridural. Revista<br />
de Cirugía de Buenos Aires 1933, 12:225-230.<br />
21. Gutiérrez A. Anestesia Peridural. Congreso de<br />
la Asociación Argentina de Cirugia. Nov. 14, 1938,<br />
Buenos Aires, Argentina.<br />
22. Gutiérrez A: La anestesia local en cirugia del<br />
abdomen. Tesis, Amorrurta 1932.<br />
23. Gutiérrez A: Sobré la relación entre el anestesiologo<br />
y el cirujano. Revista Argentina de Anestesia<br />
y Analgesia 1939, 1:5.<br />
24. Ruiz V: La anestesia peridural de Pagés en<br />
Ginecologia. Rev Med <strong>Latin</strong>o Amer 1935, 20:509-517.<br />
25. Ruiz V. Pagés Peridural anesthesia. A report <strong>of</strong><br />
3826 cases. Minnesota Med 1939, 22:363-368.<br />
26. Ontaneda LE: Tensión del espacio epidural.<br />
Su importancia práctica en la anestesia epidural<br />
metamérica. Rev Argent Circ 1933, 12:588-597.<br />
27. De Souza E: Punção extradural; tecnica de<br />
un novo sinal. Rev. Bra. Circ 1943, 12:120.<br />
28. Macin<strong>to</strong>sh RR: Extradural space indica<strong>to</strong>r.<br />
Anaesthesia 1950, 5:98-100.<br />
29. Vasconcelos E: Thoracic operations with<br />
epidural anesthesia. Dis Chest 1944, 10:471-473.<br />
30. Lemmon WT: A method <strong>of</strong> continuous spinal<br />
anesthesia. A preliminary report. Am Surg 1940,<br />
111:141-144.<br />
31. Martinez-Curbelo M: Continuous peridural<br />
segmental anesthesia by means <strong>of</strong> a ureteral catheter.<br />
Anesth Analg 1949, 28:1-4.<br />
32. Andrade Marcano D: Anestesia peridural, in<br />
Tex<strong>to</strong> de Anestesiologia Teórico-Práctica, JA Aldrete<br />
(ed). Salvat Mexicana de Ediciones, S.A. de C.V.<br />
Mexico City: Vol I, p. 675-756.1, 1986.<br />
33. Bus<strong>to</strong>s F: El signo de la burbuja o de la<br />
espuma en la anestesia peridural. Rev Argent Anest<br />
1964, 24:147-150.<br />
34. Plaza-Quijada RJ: Proposición de un signo<br />
para identificar la colocación correcta de un catéter<br />
en el espacio peridural. Rev Venez Anest 1967,<br />
2:57-62.<br />
35. Sanchez R, Acuña L, Rocha F: An analysis <strong>of</strong><br />
the radiological visualization <strong>of</strong> the catheters placed<br />
in the epidural space. Brit J Anesth 1967, 49:485-490.<br />
36. Llerena M: Un recurso más para localizar el<br />
espacio extradural. Rev Mex Anest 1969, 18:353-354.<br />
37. Andrade Marcano D: Bibliografia Anestesica<br />
Venezolana. Actas del VIII Congreso <strong>Latin</strong>oamericano<br />
y II Venezolano de Anestesiologia, 1966,<br />
2:393-413.<br />
38. Andrade Marcano D, Gutierrez H, Espinal<br />
M: Regis<strong>to</strong> y modernas interpretaciones de la presion<br />
negativa del espacio peridural. Mem Congreso<br />
Venezolano Anest., p. 148-154, 1972.<br />
39. Castaños C, Sagarnaga A: Sinal acustico para<br />
identificação da espacio extradural. Rev Bras Anest<br />
1971, 21:886-889.<br />
40. Galindo A, Hernandez J, Benavides O, et al:<br />
Quality <strong>of</strong> spinal extradural anesthesia: The influence<br />
<strong>of</strong> spinal nerve root diameter. Br J Anaesth<br />
1975, 47:41-47.<br />
41. Usubiaga JE, Usubiaga LE, Brea L: Effect<br />
<strong>of</strong> saline injections on epidural and subarachnoid<br />
space pressures and relation <strong>to</strong> post spinal anesthesia<br />
headache. Anesth Analg 1967, 46:293-296.<br />
42. Usubiaga JE, Wikinski JA, Usubiaga LE:<br />
Passage <strong>of</strong> procaine and paramino benzoic acid<br />
across the human placenta. Am J Obstet Gynecol<br />
1968, 100:918-921.<br />
43. Usubiaga JE, Wikinski JA, Wikinski A, et<br />
al: Transfer <strong>of</strong> local anesthetics <strong>to</strong> the subarachnoid<br />
space and mechanisms <strong>of</strong> epidural block. Anesthesiology<br />
1964, 25:752-759.<br />
44. Wikinski JA, Usubiaga JE, Morales RL<br />
et al: Mechanism <strong>of</strong> convulsions elicited by local<br />
anesthetic agents. I local anesthetic depression <strong>of</strong><br />
electrically induced seizures in man. Anesth Analg,<br />
1970, 49:504-508.<br />
45. Usubiaga JE: Neurologic complications after<br />
epidural anesthesia. Anesthesiol Clin 1977, 1:1-123.<br />
46. Martínez Curbelo M: Nueva técnica de<br />
la anestesia del plexo braquial: Ventajas de esta<br />
anestesia regional en cliníca or<strong>to</strong>pédica. Rev Med<br />
Cubana 1933.<br />
47. Albanes A. Periartritis – escapulo humeral.<br />
Tratamien<strong>to</strong> por las anestesias del simpatico cervico<strong>to</strong>racico.<br />
Dia Medico 1939:1.<br />
48. Ber<strong>to</strong>la V: Anestesia de la vesícula biliar y de<br />
las vías biliares. Rev Arg Anest Analg 1939, 1:18-40.<br />
49. Bier A: Ueber einen neuen Weg Localanaesthesie<br />
und den gliedmasse zu erzeugen. Verbr Dtch<br />
Ges Chir 1908, 37:204-208.<br />
50. Garcia Herreros L: Regional <strong>Anesthesia</strong> by<br />
the intravenous route. Anesthesiology 1946, 7:558-560.<br />
51. Pernin A y Vega DE: His<strong>to</strong>ria de la anestesia<br />
en el Uruguray, 1981.<br />
52. Pires FK: me<strong>to</strong>do de “Bier” para anestesia<br />
regional dos membros (diversos). Rev Bras Anest<br />
1954, 4:21-24.
BULLETIN OF ANESTHESIA HISTORY 11<br />
53. Holmes CM: Intravenous regional analgesia:<br />
a useful method <strong>of</strong> producing analgesia <strong>of</strong> the limbs.<br />
Lancet 1963, 1:245-247.<br />
54. Zerkinatti PV: Anestesia venosa regional:<br />
confeção simples do duplo mangui<strong>to</strong>. Rev Bras Anest<br />
1972, 22:238-240.<br />
55. Reis Júnior A dos: Anestesia venosa regional:<br />
latencia e analgesia pos-isquemica. Estudio comparativo<br />
utilizando bupivacaina, etidocaina, lidocaína e<br />
prilocaina. Rev Bras Anest 1975, 25:558-586.<br />
56. Reis Júnior A dos: Anestesia Regional Intravenosa.<br />
Atheneua, São Paulo, 1996.<br />
57. Reis Júnior A dos: Dessangramen<strong>to</strong> e Garroteamen<strong>to</strong><br />
de Membros Com Finalidade Cirúrgica.<br />
Atheneu, São Paulo, 1998.<br />
58. Gormley JB. Treatment <strong>of</strong> postspinal headache.<br />
Anesthesiology 1960, 21:565-566.<br />
59. Martinez Aguirre, E: La inyección peridural<br />
de sangre como tratamien<strong>to</strong> de la cefalea post punción<br />
lumbar. Pub Centro Medico de Caracas 1963,<br />
2:81-83.<br />
60. Spiegel P: Caudal anestesia in pediatric<br />
surgery. Anesth Analg 1962, 41:218-221.<br />
61. Baquero PO, Vásquez OF: Anestesia caudal<br />
en pediatría. Rev Mexicana de Anestesiología 1965,<br />
244:101-117.<br />
62. Fortuna A: Caudal Analgesia in Pediatric<br />
Surgery. Brit J Anaesth 1967, 39:165-170.<br />
63. Melman E, Peñuelas JA, Marrufo JE: Regional<br />
anesthesia in children. Anesth Analg 1975,<br />
54:387-398.<br />
64. Dalens BJ, Monnet JP, Harmand Y: Pediatric<br />
Regional <strong>Anesthesia</strong>. CRC Press Boca Ra<strong>to</strong>n, Florida<br />
1990: pp 352-374.<br />
65. Barrios-Alarcon J, Aldrete JA: Relief <strong>of</strong> postdural<br />
puncture headaches with epidural dextran-40.<br />
A preliminary report. Reg Anest 1989, 14:78-80.<br />
66. Castaños CC, Aldrete JA: Hemodilution in<br />
surgical patients with hema<strong>to</strong>crit over 70%. Phillip<br />
J. Anesth 1982, 6:30-34.<br />
67. Torrieri A, Aldrete JA: The T-A epidural<br />
spinal needle (Letter). Acta Anaesthesiol Belg 1988,<br />
39:65-66.<br />
68. Plancarte R, Amezcua C, Patt RB, Aldrete JA:<br />
Superior hypogastric plexus block for pelvic cancer<br />
pain. Anesthesiology 1990, 73:236-239.<br />
69. Plancarte R, Amezcua C, Patt RB, Lema<br />
MW: Prescaral blockade <strong>of</strong> de ganglion <strong>of</strong> Walther.<br />
Anesthesiology 1990, 73:A751.<br />
70. Usubiaga JE, Dos Reis Jr A, Usubiaga L:<br />
Epidural Misplacement <strong>of</strong> Catheters and Mechanisms<br />
<strong>of</strong> Unilateral Blockade. Anesthesiology 1970,<br />
32(2):158-161.<br />
71. Dos Reis Júnior A, Loreno AV, Slitka Filho J:<br />
Anestesia Peridural e Síndrome de Claude-Bernard-<br />
Horner. Rev Bras Anest 1977, 27(4):413-424.<br />
72. Casais de Corne AE, Ferandez FA, Lardies-<br />
Gonzalez J: Panorama His<strong>to</strong>rico de la Medicina Argentina.<br />
Todo es His<strong>to</strong>ria, Buenos Aires 1977, pp.130.<br />
73. Herrera Pontón J: His<strong>to</strong>ria de la anestesia en<br />
Colombia. Rev Col Anes 1974, 2:155-161.<br />
74. Venturini AH, Fuentes OA: His<strong>to</strong>ria de la<br />
Anestesiologia en la Republica Argentina. Rev. Arg.<br />
Anes 1979, 37:139-154.<br />
75. Takaoka K: Respirador au<strong>to</strong>mático de<br />
Takaoka. Rev Bras Anest 1964, 14:380-386.<br />
76. Takaoka K: Vaporizador Universal de<br />
Takaoka. Rev Bras Anest 1965, 15:18-24.<br />
77. Takaoka K: Novo circui<strong>to</strong> avalvular e com<br />
circulacao de gases (Miscelanea). Rev Bras Anest<br />
1968, 18:478.<br />
78. Bain JA, Spoerel WE: A streamlined anaesthetic<br />
system. Can Anaesth Soc J 1972: 19:26-428.<br />
79. Aranes GM, Bluske Castellanos L: Breves cousideraciones<br />
sobre la anestesia con pen<strong>to</strong>tal sódico y<br />
procaina. II Congreso Argentino y I <strong>Latin</strong>oamericano<br />
de Anestesiol Oct 1949.<br />
80. Wikinski JA, Wikinski RL, Ceraso OL, Arlia<br />
R, Torrieri A: General anesthesia with intravenous<br />
procaine. In Aldrete JA, Stanley TH (eds.): Trends in<br />
intravenous anesthesia. Year Book Medical Publishers,<br />
Chicago, p. 189-215, 1980.<br />
81. Caldero-Barcia R, Posseiro JJ: Physiology<br />
<strong>of</strong> uterine contraction. Clin Obstet Gynecol 1960,<br />
3:386-399.<br />
82. Aldrete JA, Kroulik D: A postanesthetic<br />
recovery score. Anesth Analg 1970, 49:924-934.<br />
83. Albin MS, Martinez Aguirre E, Albin RL:<br />
Tetrahydroamine (THA) modifications <strong>of</strong> postanesthetic<br />
emergence responses and anesthesia sleep<br />
times after ketamine HCL in the human. Proc. VI<br />
European Congress <strong>of</strong> Anaesthesiology. Amsterdam:<br />
Excerpta Medic 1974, 347:147-149.<br />
84. Martinez Aguirre E: 4 aminopyridine antagonism<br />
<strong>of</strong> ketamine-diazepam anaesthesia in children.<br />
7th World Congress <strong>of</strong> Anaesthesiology. Excerpta<br />
Medica 1980, p 416.<br />
85. Martinez Aguirre E, Wikinski J: Regional<br />
intravenous ketamine induced depression <strong>of</strong> neuromuscular<br />
transmission in man. Acta Anaesth Belg<br />
1979, 30:183-188.<br />
86. Islas JA, As<strong>to</strong>rga J, Loredo M: Epidural<br />
ketamine for control <strong>of</strong> pos<strong>to</strong>perative pain. Anesth<br />
Analg 1985, 64:1161-1162.<br />
87. Auad AO: Clonidina peridural asociada a la<br />
morfina en el tratamien<strong>to</strong> del dolor rebelde. Rev Arg<br />
Anest 1985, 43:27-34.<br />
88. Del Castillo J, Katz B: On the localization <strong>of</strong><br />
acetylcholine recep<strong>to</strong>rs. J Physiol 1955, 128:157-161.<br />
89. Usubiaga JE, et al: Prevention <strong>of</strong> succinylcholine<br />
fasciculation by local anesthetic agents.<br />
Anesthesiology 1965, 26:3-6.<br />
90. Galindo A: Depolarizing neuromuscular<br />
block. J Pharm Exp Ther 1971, 178:339-342.<br />
91. Kennedy R, Galindo A: Comparative sites<br />
<strong>of</strong> action <strong>of</strong> various anaesthetic agents at the mammalian<br />
myoneural junction. Br J Anaesth 1975,<br />
47:533-535.<br />
92. Kelly PJ: Precurazacion: potencia relativa<br />
y periodo de latencia del cloruro de tubocurarina,<br />
triyoduro de galamina y bromuro de pancuronio<br />
sobre la actividad de succinilcolina. Rev Arg Anest<br />
1976, 34:1-8.<br />
93. Kelly PJ, Pavon J, Mileta S, Farias H, Maguiro<br />
G: Interacción de anestesicos inhala<strong>to</strong>rios y endovenosos<br />
con fazadinio: efec<strong>to</strong>s sobre el cronotropismo<br />
cardíaco. Rev Arg Anest 1983, 41:1-6.
12 BULLETIN OF ANESTHESIA HISTORY<br />
From the Literature<br />
by A.J. Wright, M.L.S.<br />
Department <strong>of</strong> Anesthesiology Library, University <strong>of</strong> Alabama at Birmingham<br />
Note: In general, I have not examined articles<br />
that do not include a notation for the number<br />
<strong>of</strong> references, illustrations, etc. I do examine<br />
most books and book chapters. Books can be<br />
listed in this column more than once as new<br />
reviews appear. Older articles are included<br />
as I work through a large backlog <strong>of</strong> materials.<br />
Some listings are not directly related <strong>to</strong><br />
anesthesia, pain or critical care but concern<br />
individuals important in the his<strong>to</strong>ry <strong>of</strong> the<br />
specialty [i.e., Harvey Cushing or William<br />
Halsted]. Non-English articles are so indicated.<br />
Columns for the past several years are available<br />
in the “<strong>Anesthesia</strong> His<strong>to</strong>ry Files” at<br />
http://www.anes.uab.edu/aneshist/aneshist.<br />
htm as “Recent Articles on <strong>Anesthesia</strong> His<strong>to</strong>ry.”<br />
I urge readers <strong>to</strong> send me any citations,<br />
especially those not in English, that I may otherwise<br />
miss!—A.J. Wright ajwright@uab.edu<br />
Books<br />
Barr M. Surgery, Sand and Saigon Tea. An<br />
Australian Army Doc<strong>to</strong>r in Vietnam. Allen and<br />
Unwin, 2001. 252pp. [rev. Boul<strong>to</strong>n TB. Anaesthesia<br />
57: 104, 316, 2002; Gray D. Br J Anaesth<br />
88:464-465, 2002]<br />
Blaufox MD. An Ear <strong>to</strong> the Chest: An Illustrated<br />
His<strong>to</strong>ry <strong>of</strong> the Evolution <strong>of</strong> the Stethoscope.<br />
CRC Press, 2001. 120pp.<br />
Curtis JR, Rubenfeld GD. Managing Death<br />
in the Intensive Care Unit: The Transition from<br />
Cure <strong>to</strong> Comfort. Oxford University Press, 2001.<br />
388pp. [rev. Ware LR. NEJM 346:542, February<br />
14, 2002]<br />
Fenster JM. Ether Day: The Strange Tale <strong>of</strong><br />
<strong>Ameri</strong>ca’s Greatest Medical Discovery and the<br />
Haunted Men Who Made It. New York: Harper<br />
Collins, 2001. 278pp. [rev. Samuels SI. JAMA<br />
286:2877-2878, 2001]<br />
Fink BR, McGoldrick KE, eds. Careers in<br />
Anesthesiology, Au<strong>to</strong>biographical Memoirs, Volume<br />
3. Park Ridge, Ill.: Wood Library-Museum,<br />
1999. 214pp. [rev. Calmes S. Bull Hist Med<br />
75:831-832, 2001]<br />
Fink BR, McGoldrick KE, eds. Careers in<br />
Anesthesiology, Au<strong>to</strong>biographical Memoirs, Volume<br />
4. Park Ridge, Ill.: Wood Library-Museum,<br />
2000. 181pp. [rev. Maltby JR. Can J Anesth<br />
48:1172, 2001; Bailey RJ. Anaesth Intens Care<br />
29:675, 2001]<br />
Hodgson B. In the Arms <strong>of</strong> Morpheus: The<br />
Tragic His<strong>to</strong>ry <strong>of</strong> Laudanum, Morphine, and<br />
Patent Medicines. Firefly, 2001. 160pp. [rev.<br />
Arsenault K. Library Journal January 2002 pp<br />
141, 144]<br />
Owen, Charles A., Jr. A His<strong>to</strong>ry <strong>of</strong> Blood<br />
Coagulation. Mayo Foundation, 2001. 355pp.<br />
[rev. Kwaan HC. JAMA 287:1051-1052, February<br />
27, 2002]<br />
Pain and Suffering in His<strong>to</strong>ry: Narratives <strong>of</strong><br />
Science, Medicine and Culture. Papers Presented<br />
March 13-14, 1998, at the His<strong>to</strong>ry <strong>of</strong> Pain Symposium,<br />
University <strong>of</strong> California, Los Angeles. The<br />
University, 1999<br />
Safar P. Careers in Anesthesiology: An Au<strong>to</strong>biographical<br />
Memoir, Volume 5. Park Ridge, Ill.:<br />
Wood Library-Museum, 2000. 397pp. [rev. Reilly<br />
PF. Anaesth Intens Care 29:675-676, 2001]<br />
Standl T, Goerig M, Schulte am Esch J. 35<br />
Jahre Lehrstuhl fur Anasthesiologie am Universitatsklinikum<br />
Hamburg-Eppendorf. Zur Entwicklung<br />
einer anasthesiologischen Einrichtung.<br />
Hamburg: The Department, 2001. 67pp. Illus.<br />
Trubuhovich RV, Judson JA. Intensive Care<br />
in New Zealand. A His<strong>to</strong>ry <strong>of</strong> the New Zealand<br />
Region <strong>of</strong> ANZICS. privately printed, 2001 ().<br />
150pp. [rev. Winship S, Wang J. Br J Anaesth<br />
87:946, 2001<br />
Wolfe RJ. Tarnished Idol: William T.G.<br />
Mor<strong>to</strong>n and the Introduction <strong>of</strong> Surgical <strong>Anesthesia</strong>.<br />
Norman, 2001. 672pp. [rev. Ca<strong>to</strong>n D.<br />
NEJM 346:70, January 3, 2002; Torpy JM. JAMA<br />
287:1327-1328, March 13, 2002]<br />
Articles and Book Chapters<br />
Ball C, Westhorpe R. Intravneous induction<br />
agents: benzodiazepines. Anaesth Intens Care 30:3,<br />
2002 [cover note; 1 illus., 7 refs.]<br />
Ball C, Westhorpe R. Induction agents:<br />
“Avertin.” Anaesth Intens Care 29:571, 2001 [cover<br />
note; 1 illus., 5 refs.]<br />
Bollet AJ. Civil War Medicine: Challenges and<br />
Triumphs. Galen Press, 2002. [Has some material<br />
on anethesia pp 76-81; blood transfusions pp<br />
185-186; and opium and morphine pp 238-242]<br />
Bracourt H. First intravenous injections:<br />
the infusions <strong>of</strong> the 17th century. Rev Prat<br />
51(14):1519-1523, September 15, 2001 [French]<br />
Brown T. Popular Patents: <strong>Ameri</strong>ca’s First<br />
Inventions from the Airplane <strong>to</strong> the Zipper.<br />
Scarecrow Press, 2000. [Includes Jackson and<br />
Mor<strong>to</strong>n’s patent for anesthesia, pp 27-28; and<br />
two other inventions Jackson tried <strong>to</strong> claim for<br />
himself: Schonbein’s guncot<strong>to</strong>n pp 98-99 and<br />
Morse’s telegraph, pp 176-178]<br />
Buzello TF, van der Schyff SG. Curare in<br />
medicine: in search <strong>of</strong> a disease (a his<strong>to</strong>rical<br />
perspective). Eur J Anaesthesiol 18, suppl 23: 106,<br />
2001 [abstract; 1 table, 8 refs.]<br />
Caponi G. Claude Bernard and the boundaries<br />
<strong>of</strong> experimental physiology. Hist Cienc Saude<br />
Manguinhis 8:375-406, 2001 [Portuguese]<br />
Chaloner EJ, Ham RJ. Amputations at the<br />
London Hospital 1852-1857. J Roy Soc Med<br />
94:409-412, 2001 [Notes results <strong>of</strong> amputations<br />
under ether vs. under chlor<strong>of</strong>orm. 1 chart, 3 tables,<br />
12 refs. Response by Howat DDC. J Roy Soc Med<br />
94:657, 2001]<br />
Charl<strong>to</strong>n E. Patrick David Wall FRS, DM,<br />
FRCP. Honorary member AAGBI, 1925-2001.<br />
Anaesthesia 56:1202, 2001 [Obituary]<br />
Cope DK. Mortality during the first 25 years<br />
<strong>of</strong> general anesthesia in <strong>Ameri</strong>ca: contemporary<br />
outcome studies. Am J Anesthesiol 28:455-460,<br />
2001 [Rep. Bull Anesth Hist 17(3):12-17, 1999; 5<br />
illus., 21 refs.]<br />
Crenner C. Organizational reform and pr<strong>of</strong>essional<br />
dissent in the careers <strong>of</strong> Richard Cabot and<br />
Ernest Amory Codman, 1900-1920. J Hist Med<br />
Allied Sci 56:211-237, 2001<br />
Diaz JH. Call all anesthetists <strong>to</strong> service in<br />
World War II. Anesthesiology 96:776-777, 2001<br />
[Correspondence; response <strong>to</strong> Waisel DB. Anesthesiology<br />
94:907-914, 2001. 2 refs. Waisel DB.<br />
Response. Anesthesiology 96:777, 2002. 1 ref.]<br />
Egger EI II. A brief his<strong>to</strong>ry <strong>of</strong> the origin <strong>of</strong><br />
minimum alveolar concentration (MAC). Anesthesiology<br />
96:238-239, 2002 [Classic Papers Revisted<br />
series; 8 refs.]<br />
Ekiert LJ. The his<strong>to</strong>ry <strong>of</strong> tranquilizing and<br />
sleeping drugs. Arch Hist Filoz Med 63(3-4):126-<br />
128, 2000 [Polish]<br />
50th anniversary volume <strong>of</strong> the Japanese<br />
Journal <strong>of</strong> Anesthesiology. Masui 50 suppl:1-289,<br />
September 2001. [Japanese]<br />
Hanson III CW, Durbin CG Jr, Maccioli GA,<br />
et al. The anesthesiologist in critical care medicine:<br />
past, present and future. Anesthesiology 95:<br />
781-788, 2001 [4 illus., 41 refs.]<br />
Hart GD. Description <strong>of</strong> blood and blood disorders<br />
before the advent <strong>of</strong> labora<strong>to</strong>ry studies. Br<br />
J Haema<strong>to</strong>l 115: 719-728, 2001 [10 illus., 25 refs.]<br />
Hawkes E, Leafty C, Ruth C, Scott R, Sharp L.<br />
Nurse anesthesia: the silent pr<strong>of</strong>ession. Windows<br />
in Time 9(2): 5-6, November 2001<br />
Horvitz LA. Eureka! Scientific Breaththroughs<br />
that Changed the World. Wiley, 2002.<br />
256pp. [includes Joseph Priestley’s isolation <strong>of</strong><br />
oxygen]<br />
Howat DDC. Amputations at the London<br />
Hospital, 1852-1857. J Roy Soc Med 94:657, 2001<br />
[Correspondence. 3 refs. Response <strong>to</strong> Chaloner<br />
EJ. J Roy Soc Med 94:409-412, 2001]<br />
Hyson JM Jr. Man and pain: eternal partners.<br />
J His<strong>to</strong>ry Dent 49(3):115-121, November 2001<br />
[38 refs.]<br />
Jones JT. Brian Francis Horan: edi<strong>to</strong>r 1982-<br />
1988. Anaesth Intens Care 29:461-462, 2001 [Obituary.<br />
Portrait.]<br />
Kiss I. From anaesthesia for neurosurgery <strong>to</strong><br />
neuroanaesthesia. A his<strong>to</strong>rical note. Acta Neurochir<br />
(Wien) 142:1391-1395, 2000 [3 illus., 25 refs.]<br />
Koehler PJ, van de Wiel TWM. Aretaeus on<br />
migraine and headache. J Hist Neurosci 10:253-<br />
261, 2001 [27 refs.]<br />
Kopp VJ. World War II and physician specialization.<br />
Anesthesiology 96:776, 2002 [Correspondence;<br />
response <strong>to</strong> Waisel DB. Anesthesiology<br />
94:907-914, 2001. 10 refs. Waisel DB. Response.<br />
Anesthesiology 96:777, 2002. 1 ref.]<br />
Kotiniemi L, Autio S, Hyrynkangas K. Anaesthetic<br />
his<strong>to</strong>ry <strong>of</strong> a patient: 250 anaesthetics<br />
in 30 years. Anaesthesia 57:207-208, 2002 [correspondence;<br />
3 refs.]<br />
Kuhlen FJ. His<strong>to</strong>ry <strong>of</strong> pain and pain treatment.<br />
Pharm Unserer Zeit 31(!):13-22, 2002<br />
Continued on next page
BULLETIN OF ANESTHESIA HISTORY 13<br />
MedNuggets<br />
by Fred J. Spielman, M.D.<br />
Department <strong>of</strong> Anesthesiology, University <strong>of</strong> North Carolina<br />
An examination <strong>of</strong> the literature on the<br />
subject reveals that a number <strong>of</strong> workers<br />
have come <strong>to</strong> the conclusion that there is<br />
some peculiarity in the physiology <strong>of</strong> the<br />
pregnant woman which renders her unsuitable<br />
for the induction <strong>of</strong> spinal anesthesia.<br />
— F. Barnett Mallinson<br />
British Journal <strong>of</strong> Anaesthesia 16:22,<br />
1938-9<br />
The anesthetist has a useful role in the<br />
diagnosis and treatment <strong>of</strong> coma. Coma is<br />
not unlike surgical anesthesia; in fact anesthesia<br />
is correctly defined as a state <strong>of</strong> coma.<br />
— E.A. Rovenstine<br />
Anesthesiology 6:1, 1945<br />
The more you use it (spinal anesthesia)<br />
the less confidence you have in it.<br />
— Harold Welling<strong>to</strong>n Jones<br />
Annals <strong>of</strong> Surgery 96:85, 1932<br />
The mistake lay in the assumption that<br />
fatalities under anaesthesia must be due <strong>to</strong><br />
excess <strong>of</strong> the anaesthetic. This is an error<br />
which it seems extremely difficult <strong>to</strong> overcome<br />
in the minds <strong>of</strong> surgeons.<br />
—Yandell Henderson<br />
Surgery, Gynecology, Obstetrics 19:386,<br />
1914<br />
Somewhere there is a paradox in the fact<br />
that <strong>to</strong> take out a lung requires more training<br />
and experience and learning and judgment<br />
than it does <strong>to</strong> take away consciousness, yet<br />
the loss <strong>of</strong> consciousness has immeasurably<br />
greater effect on the individual.<br />
— Henry K. Beecher<br />
Surgical Forum 5:679, 1954<br />
The choice <strong>of</strong> anaesthesia and the technique<br />
<strong>of</strong> the actual operations are matters<br />
which must always be largely governed by<br />
personal preference and by local conditions.<br />
— Reginald Payne<br />
British Journal <strong>of</strong> Surgery 27:740, 1939-<br />
40<br />
The surgeon who has not tasted anesthesia<br />
for his surgery under the best possible<br />
auspices has something <strong>to</strong> look forward <strong>to</strong>,<br />
the value <strong>of</strong> which he perhaps does not yet<br />
appreciate. A higher quality in anesthesia<br />
than the present best is surely still <strong>to</strong> be<br />
attained and never before has there been<br />
such active effort in seeking it.<br />
— Ralph T. Knight<br />
Surgery 18:130, 1945<br />
Anesthetics are among the most potent<br />
and dangerous drugs used in the practice <strong>of</strong><br />
medicine; they penetrate <strong>to</strong> every cell and<br />
organ <strong>of</strong> the body and may cause almost instant<br />
or delayed death by their <strong>to</strong>xic effects.<br />
— Frank H. McMechan<br />
Journal <strong>of</strong> the <strong>Ameri</strong>can Medical Association<br />
104:1428, 1935<br />
Today’s widening scope <strong>of</strong> surgery, allowing<br />
help <strong>to</strong> even the poorest <strong>of</strong> “risks”<br />
depends on team-work. The problems are<br />
discussed by all who can bring their special<br />
knowledge in<strong>to</strong> play. The anaesthetist<br />
should not and cannot be missing from<br />
this team and must be as conversant in<br />
present-day medical knowledge as the best<br />
on the team.<br />
— Stanislaw B. Donigiewicz<br />
Canadian Anaesthetists’ Society Journal<br />
5:75, 1958<br />
The first problem for both the anesthetist<br />
and the surgeon <strong>to</strong> work out after the operation<br />
is decided upon, is <strong>to</strong> determine what<br />
anesthetic is <strong>to</strong> be used, in the particular<br />
case at the time. Here the anesthetist should<br />
be consulted and his experience becomes<br />
invaluable <strong>to</strong> the surgeon in making this<br />
determination.<br />
— A.R. DaCosta<br />
Current Researches in <strong>Anesthesia</strong> and<br />
Analgesia 16:18, 1938<br />
The condemnation <strong>of</strong> an agent as the<br />
cause <strong>of</strong> death is still <strong>to</strong>o frequently quoted<br />
as the responsible <strong>of</strong>fender. Such condemnation<br />
<strong>of</strong> agents is unjustified and the responsbilitiy<br />
should be placed upon the person at<br />
the head <strong>of</strong> the table.<br />
— Paul H. Lorhan<br />
The <strong>Ameri</strong>can Surgeon 18:727, 1952<br />
On no account should a practitioner endeavour<br />
<strong>to</strong> administer an anaesthetic whilst<br />
acting as opera<strong>to</strong>r also.<br />
— William W. Mushin<br />
Anaesthesia 9:232, 1954<br />
The leaders <strong>of</strong> medicine and surgery <strong>to</strong>day<br />
realize the seriousness <strong>of</strong> carrying a living<br />
being <strong>to</strong> that level <strong>of</strong> insensibility which,<br />
in many respects, simulates death, and also<br />
recognize that the anesthesia is, in most<br />
instances as important as the operation.<br />
— Sidney Cushing Wiggen<br />
New England Journal <strong>of</strong> Medicine<br />
204:1283, 1931<br />
For the surgeon, then, the question has<br />
come <strong>to</strong> be not “what anesthetic” but “ what<br />
anesthetist”<br />
— Edward M. Livings<strong>to</strong>ne<br />
<strong>Ameri</strong>can Journal <strong>of</strong> Surgery 19:67, 1933<br />
Many other similar types <strong>of</strong> work no<br />
doubt exist in other spheres <strong>of</strong> medicine<br />
where by reason <strong>of</strong> his special knowledge<br />
or technical skill the anaesthetist is the<br />
person best qualified <strong>to</strong> take charge. It is <strong>of</strong><br />
great importance that we should take every<br />
opportunity <strong>to</strong> extend these sections <strong>of</strong> our<br />
specialty as it may well be that before long<br />
our standing in the medical world will be<br />
judged rather by the quality <strong>of</strong> our clinical<br />
work than by our technical skill.<br />
— A.R. Hunter<br />
Anesthesiology 13:108, 1952<br />
Literature. . .Continued from page 12<br />
[German]<br />
Mathews TP. Vietnam vet gives anesthesia his<strong>to</strong>ry<br />
lesson. ASA Newsletter 66(2):37-38, February<br />
2002 [correspondence]<br />
Morell J. Aspirina: 100 anos de publicidad<br />
(1899-1999). BSAHCFC: butlleti de la Societat<br />
d’Amics de la His<strong>to</strong>ria i de la Ciencia Farmaceutica<br />
Catalana 10(26):36, May-August 2001 [Spanish]<br />
Newson AJ. All here are agog with the chlor<strong>of</strong>orm.<br />
Aust NZ J Surg 70:862-869, 2000 [2 illus.,<br />
21 refs.]<br />
Norman J. The British Journal <strong>of</strong> Anaesthesia:<br />
an informal his<strong>to</strong>ry <strong>of</strong> the first 25 years. Br J<br />
Anaesth 88:445-450, 2002<br />
O’Dowd MJ. “<strong>Anesthesia</strong> and analgesia and<br />
the curse <strong>of</strong> Eve. In: The His<strong>to</strong>ry <strong>of</strong> Medications<br />
for Women: Materia medica woman. Parthenon,<br />
2001, pp 275-295 [18 illus., numerous refs.]<br />
Patterson R. Charles Thomas Jackson, MD,<br />
Vesuvius, and the idea <strong>of</strong> surgical anaesthesia. J<br />
Continued on page 16
14 BULLETIN OF ANESTHESIA HISTORY<br />
The Wood Library-Museum Book<br />
Signing at the ASA Annual Meeting<br />
in New Orleans<br />
Oc<strong>to</strong>ber 15, 2001<br />
From left <strong>to</strong> right: Dr. Kathryn McGoldrick,<br />
Dr. John Steinhaus, Dr. Eli Brown, Mrs. Peggy<br />
Fink, Dr. Carlos Parsloe, and Dr. Thomas T.<br />
McGranahan.<br />
Mrs. Peggy Fink au<strong>to</strong>graphs Careers VI for<br />
Dr. William Hammonds.<br />
Dr. Thomas McGranahan and Mrs. Peggy Fink sign<br />
copies <strong>of</strong> Careers VI for Dr. John Neeld and Dr. John<br />
Steinhaus.<br />
Dale C. Smith, Ph.D., 2001 Lewis<br />
H. Wright Memorial Lecturer,<br />
accepts appreciation scroll from Dr.<br />
Kathryn McGoldrick.
BULLETIN OF ANESTHESIA HISTORY 15
16 BULLETIN OF ANESTHESIA HISTORY<br />
Literature. . .Continued from page 13<br />
Med Biog 9:220-225, 2001 [2 illus., 20 refs.]<br />
Pelis K. Blood standards and failed fluids:<br />
clinic, lab, and transfusion solutions in London,<br />
1868-1916. Hist Sci 39:185-213, 2001 [131 refs.]<br />
Plourde G. Claude Bernard, the spinal cord,<br />
and anesthesia. Anesthesiology 95:1542, 2001 [Correspondence;<br />
8 refs.]<br />
Prout G. Seishu Hanaoka. Medifila nos. 42-<br />
43: 44, 2001<br />
Riess KO, Millman-Guller L. MHAUS celebrates<br />
the 20th anniversary <strong>of</strong> its founding. Am<br />
J Anesthesiol 28:461-462, 2001<br />
Shealy CN, Cady RK. His<strong>to</strong>rical perspective<br />
<strong>of</strong> pain management. In: Weiner RS, ed. Pain<br />
Management: A Practical Guide for Clinicians.<br />
6th ed. CRC Press, 2001, pp 9-16 [1 illus., 2 tables,<br />
references, annotated bibliography]<br />
Shephard DAE. John Snow and resuscitation.<br />
Resuscitation 49:3-7, 2001 [3 illus., 16 refs.]<br />
Simpson P, Popat M. “Anaesthesia: his<strong>to</strong>ry and<br />
introduction. In: Understanding Anaesthesia. 4th<br />
ed. Butterworth Heinemann, 2002, pp 1-5<br />
Takeda F. The development <strong>of</strong> use <strong>of</strong> oral<br />
morphine within the last 10 years in Japan. Eur<br />
J Pain 5(a):79-82, December 2001<br />
von Hintzenstern U, Petermann H, Schwarz<br />
W. Early contributions from Erlangen <strong>to</strong> the<br />
theory and practice <strong>of</strong> general anesthsia with<br />
ether and chlor<strong>of</strong>orm. 2. The animal experiments<br />
<strong>of</strong> Ernst von Bibra and Emil Harless. Anaesthesist<br />
50:869-880, 2001 [German; 6 illus., 31 refs. ]<br />
WLM Board <strong>of</strong> Trustees Meeting, Oc<strong>to</strong>ber 15, 2001 in New Orleans. From left <strong>to</strong> right, seated: Dr. Charles<br />
Tandy, Mr. Patrick Sim, Dr. Kathyrn McGoldrick, Dr. Donald Ca<strong>to</strong>n, Dr. Dale Smith, Dr. Jonathan Berman,<br />
and Dr. Doris Cope. From left <strong>to</strong> right, standing: Dr. Elliott Miller, Dr. Selma Calmes, Dr. Douglas Bacon,<br />
Dr. Lydia Conlay, Dr. George Bause, Dr. Jeffrey Cusick, Dr. William Hammonds, Dr. George Sheplock, Dr.<br />
SusanVassallo, Dr. Mary Ellen Warner, and Dr. Adolph Giesecke.<br />
Bulletin <strong>of</strong> <strong>Anesthesia</strong> His<strong>to</strong>ry<br />
Doris K. Cope, M.D., Edi<strong>to</strong>r<br />
200 Delafield Avenue, Suite 2070<br />
Pittsburgh, PA 15215