Wellness Reimbursement Form - Unity Health Insurance
Wellness Reimbursement Form - Unity Health Insurance
Wellness Reimbursement Form - Unity Health Insurance

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
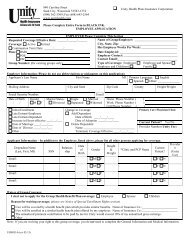
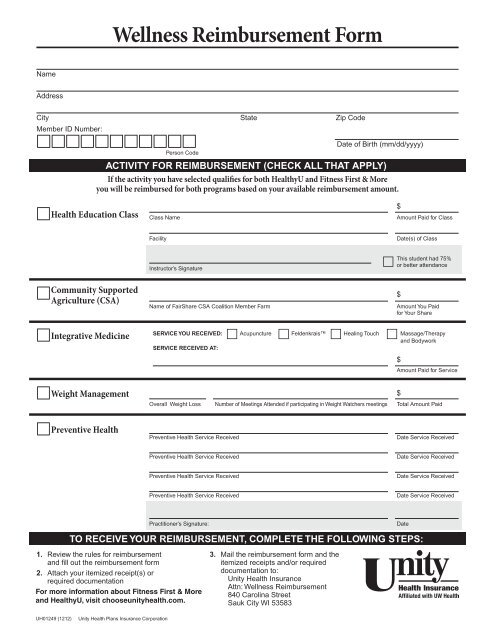
<strong>Wellness</strong> <strong>Reimbursement</strong> <strong>Form</strong><br />
Name<br />
Address<br />
City State Zip Code<br />
Member ID Number:<br />
<br />
Person Code<br />
Date of Birth (mm/dd/yyyy)<br />
ACTIVITY FOR REIMBURSEMENT (CHECK ALL THAT APPLY)<br />
If the activity you have selected qualifies for both <strong>Health</strong>yU and Fitness First & More<br />
you will be reimbursed for both programs based on your available reimbursement amount.<br />
<strong>Health</strong> Education Class<br />
Class Name<br />
$<br />
Amount Paid for Class<br />
Facility<br />
Date(s) of Class<br />
Community Supported<br />
Agriculture (CSA)<br />
Instructor’s Signature<br />
Name of FairShare CSA Coalition Member Farm<br />
<br />
This student had 75%<br />
or better attendance<br />
$<br />
Amount You Paid<br />
for Your Share<br />
Integrative Medicine<br />
SERVICE YOU RECEIVED: Acupuncture Feldenkrais Healing Touch Massage/Therapy<br />
and Bodywork<br />
SERVICE RECEIVED AT:<br />
$<br />
Amount Paid for Service<br />
Weight Management<br />
Overall Weight Loss Number of Meetings Attended if participating in Weight Watchers meetings Total Amount Paid<br />
$<br />
Preventive <strong>Health</strong><br />
Preventive <strong>Health</strong> Service Received<br />
Date Service Received<br />
Preventive <strong>Health</strong> Service Received<br />
Date Service Received<br />
Preventive <strong>Health</strong> Service Received<br />
Date Service Received<br />
Preventive <strong>Health</strong> Service Received<br />
Date Service Received<br />
Practitioner’s Signature:<br />
TO RECEIVE YOUR REIMBURSEMENT, COMPLETE THE FOLLOWING STEPS:<br />
1. Review the rules for reimbursement<br />
and fill out the reimbursement form<br />
2. Attach your itemized receipt(s) or<br />
required documentation<br />
For more information about Fitness First & More<br />
and <strong>Health</strong>yU, visit chooseunityhealth.com.<br />
3. Mail the reimbursement form and the<br />
itemized receipts and/or required<br />
documentation to:<br />
<strong>Unity</strong> <strong>Health</strong> <strong>Insurance</strong><br />
Attn: <strong>Wellness</strong> <strong>Reimbursement</strong><br />
840 Carolina Street<br />
Sauk City WI 53583<br />
Date<br />
UH01249 (1212)<br />
<strong>Unity</strong> <strong>Health</strong> Plans <strong>Insurance</strong> Corporation
RULES FOR REIMBURSEMENT<br />
<strong>Health</strong> Education Classes<br />
Classes must be held at one of <strong>Unity</strong>’s participating hospitals<br />
or clinics or other approved vendors and fall into one of the<br />
following categories:<br />
• Pregnancy and parenting<br />
• Nutrition<br />
• Weight management<br />
• Special activities, e.g. yoga and Pilates<br />
• CPR and First Aid<br />
• Stress and Anxiety Management (e.g. mindfulness and<br />
meditation)<br />
• Tobacco use cessation<br />
You may also receive reimbursement for membership in the<br />
Children & Adults with Attention-Deficit/Hyperactivity Disorder<br />
(CHADD®) program.<br />
Requirements for reimbursement:<br />
• Attend 75% of the classes of an approved program or if<br />
purchased an unlimited pass you must attend at least 10 classes<br />
in one month<br />
• Be a <strong>Unity</strong> member at the completion of the class<br />
• Complete the <strong>Wellness</strong> <strong>Reimbursement</strong> <strong>Form</strong> and have the<br />
instructor sign it<br />
• Mail the completed reimbursement form to <strong>Unity</strong> upon finishing<br />
the class<br />
* For the CHADD® program you will also need to submit the pre and post surveys as well<br />
as a copy of the welcome letter from CHADD®.<br />
Community Supported Agriculture (CSA)<br />
<strong>Reimbursement</strong> Requirements<br />
• Purchase a produce share from a FairShare CSA Coalition<br />
member farm<br />
• Be a <strong>Unity</strong> member on the date of purchase<br />
• Complete the <strong>Wellness</strong> <strong>Reimbursement</strong> <strong>Form</strong><br />
• Mail the completed reimbursement form and one of the<br />
following proofs of payment to <strong>Unity</strong> in the same calendar<br />
year it was purchased:<br />
– Itemized receipt from the farm<br />
– Copy of an email from the farm acknowledging your<br />
purchase (must include the amount you paid for your share<br />
and date of purchase). Please Note: e date the email was<br />
sent to you does not constitute the date of purchase.<br />
– A copy of your canceled check or credit card receipt<br />
(If you are splitting a produce share, be sure your name is<br />
included on the proof of payment. Also, indicate the amount you<br />
paid for your portion of the share on the reimbursement form.)<br />
Please Note: If you have completed your health risk assessment<br />
and/or biometric measurements (through a <strong>Unity</strong> screening or<br />
by submitting a biometric exception form), this information will<br />
automatically be updated by <strong>Unity</strong>. You don’t need to complete<br />
this form for either the HRA or biometrics portions of the<br />
<strong>Health</strong>yU program.<br />
Integrative Medicine <strong>Reimbursement</strong> Requirements:<br />
• Receive one of the following eligible integrative medicine services:<br />
– Acupuncture<br />
– Feldenkrais<br />
– Healing Touch<br />
– Massage erapy and Bodywork<br />
• Receive the service from an eligible provider<br />
– UW <strong>Health</strong> Integrative Medicine<br />
– <strong>Unity</strong> Fitness First Participating <strong>Health</strong> Club<br />
– <strong>Unity</strong> <strong>Health</strong> First Vendor listed under Massage erapy,<br />
Acupuncture and Spa Services<br />
• Be a <strong>Unity</strong> member on the date of service<br />
• Complete the <strong>Wellness</strong> <strong>Reimbursement</strong> <strong>Form</strong><br />
• Mail the completed reimbursement form and your itemized<br />
receipt to <strong>Unity</strong> upon receiving the service. e itemized receipt<br />
must include your name, the provider’s name, address, telephone<br />
number, license number, description of service received, date of<br />
service and the amount paid. Tips and gratuities are not<br />
reimbursable.<br />
Weight Management <strong>Reimbursement</strong> Requirements<br />
• Participate in Weight Watchers® meetings or Weight Watchers®<br />
online for three consecutive months or participate in all<br />
Diet-Free® meetings<br />
• Be a <strong>Unity</strong> member at the completion of your participation<br />
• Complete the <strong>Wellness</strong> <strong>Reimbursement</strong> <strong>Form</strong><br />
• Mail the completed reimbursement form, a copy of your<br />
personal weight tracker (if participating in Weight Watchers®)<br />
or receipt of payment (if participating in Diet-Free) to <strong>Unity</strong><br />
Preventive <strong>Health</strong> Screenings <strong>Reimbursement</strong> Requirements<br />
is form only needs to be completed if you received the required<br />
preventive service from a non-participating provider.<br />
• Receive a required preventive health screening based on the<br />
chart below<br />
• Complete the <strong>Wellness</strong> <strong>Reimbursement</strong> <strong>Form</strong> and have your<br />
practitioner sign and date it<br />
• Mail the completed reimbursement form to <strong>Unity</strong><br />
Female<br />
Male<br />
18-20 21-25 26-44 45-49 50-64 65+ 18-34 35-44 45-49 50-64 65+<br />
Biometrics X X X X X X X X X X X<br />
Chlamydia Screening X X<br />
Colorectal Cancer<br />
Screening<br />
X X X X<br />
Dental Exam X X X X X X X X X X X<br />
Eye Exam X X X X X X X X X X X<br />
Flu Vaccination X X X X X X X X X X X<br />
Mammogram X X<br />
Office Visit with Primary<br />
Care Provider<br />
X X X X X X X X X X X<br />
Pap Test X X X X X<br />
Pneumonia Vaccination X X<br />
Minimum Number<br />
Needed to<br />
Complete Challenge<br />
4 4 3 3 3 3 3 3 3 3 3<br />
Minimum number of preventive screenings are based on your age as of January 1.