FITNESS ASSESSMENT HEALTH HISTORY FORM
FITNESS ASSESSMENT HEALTH HISTORY FORM
FITNESS ASSESSMENT HEALTH HISTORY FORM

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
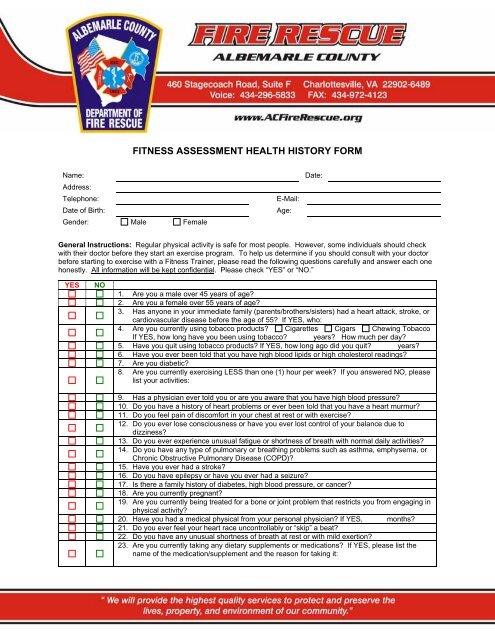
<strong>FITNESS</strong> <strong>ASSESSMENT</strong> <strong>HEALTH</strong> <strong>HISTORY</strong> <strong>FORM</strong><br />
Name:<br />
Address:<br />
Telephone:<br />
Date of Birth:<br />
Gender: Male Female<br />
E-Mail:<br />
Age:<br />
Date:<br />
General Instructions: Regular physical activity is safe for most people. However, some individuals should check<br />
with their doctor before they start an exercise program. To help us determine if you should consult with your doctor<br />
before starting to exercise with a Fitness Trainer, please read the following questions carefully and answer each one<br />
honestly. All information will be kept confidential. Please check “YES” or “NO.”<br />
YES<br />
NO<br />
1. Are you a male over 45 years of age<br />
2. Are you a female over 55 years of age<br />
3. Has anyone in your immediate family (parents/brothers/sisters) had a heart attack, stroke, or<br />
cardiovascular disease before the age of 55 If YES, who:<br />
4. Are you currently using tobacco products Cigarettes Cigars Chewing Tobacco<br />
If YES, how long have you been using tobacco years How much per day<br />
5. Have you quit using tobacco products If YES, how long ago did you quit years<br />
6. Have you ever been told that you have high blood lipids or high cholesterol readings<br />
7. Are you diabetic<br />
8. Are you currently exercising LESS than one (1) hour per week If you answered NO, please<br />
list your activities:<br />
9. Has a physician ever told you or are you aware that you have high blood pressure<br />
10. Do you have a history of heart problems or ever been told that you have a heart murmur<br />
11. Do you feel pain of discomfort in your chest at rest or with exercise<br />
12. Do you ever lose consciousness or have you ever lost control of your balance due to<br />
dizziness<br />
13. Do you ever experience unusual fatigue or shortness of breath with normal daily activities<br />
14. Do you have any type of pulmonary or breathing problems such as asthma, emphysema, or<br />
Chronic Obstructive Pulmonary Disease (COPD)<br />
15. Have you ever had a stroke<br />
16. Do you have epilepsy or have you ever had a seizure<br />
17. Is there a family history of diabetes, high blood pressure, or cancer<br />
18. Are you currently pregnant<br />
19. Are you currently being treated for a bone or joint problem that restricts you from engaging in<br />
physical activity<br />
20. Have you had a medical physical from your personal physician If YES, months<br />
21. Do you ever feel your heart race uncontrollably or “skip” a beat<br />
22. Do you have any unusual shortness of breath at rest or with mild exertion<br />
23. Are you currently taking any dietary supplements or medications If YES, please list the<br />
name of the medication/supplement and the reason for taking it:
<strong>FITNESS</strong> <strong>ASSESSMENT</strong> <strong>HEALTH</strong> <strong>HISTORY</strong> <strong>FORM</strong><br />
Page 2<br />
Are you an active firefighter and/or EMS provider Yes No<br />
When was your last fire department physical/medical exam<br />
Emergency Contact Name:<br />
Relationship:<br />
Telephone:<br />
<strong>FITNESS</strong> TRAINER USE ONLY<br />
Resting Heart Rate: I. II. III.<br />
Resting Blood Pressure: I. II. III.<br />
Weight: kg Target Exercise Heart Rate (85% MHR):<br />
Cleared to Exercise NO YES<br />
Date Physician Release Received:<br />
• If client answered YES to two or more questions of the questionnaire.<br />
• If first heart rate >110bpm and/or blood pressure > 160/100 mmHg, have client rest for five<br />
(5) minutes and reassess. If unchanged, refer to physician and delay/reschedule assessment.<br />
Signature:<br />
Date:<br />
Fitness Trainer (please print):<br />
Fitness Trainer Signature: