Optical Coherence Tomography OCT: Retinal Layers Retinal OCT ...
Optical Coherence Tomography OCT: Retinal Layers Retinal OCT ...
Optical Coherence Tomography OCT: Retinal Layers Retinal OCT ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
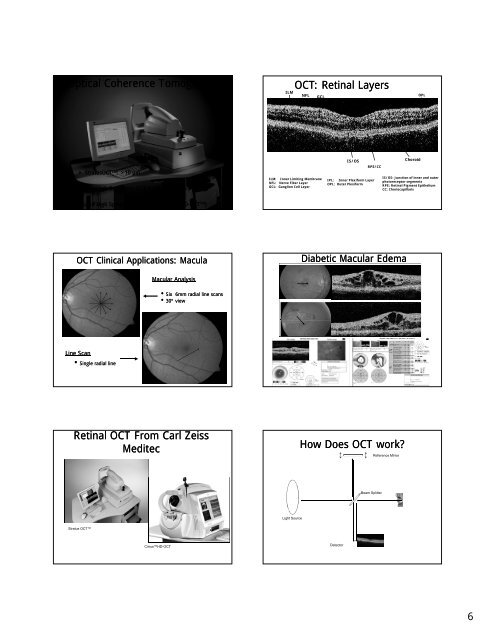
<strong>Optical</strong> <strong>Coherence</strong> <strong>Tomography</strong><br />
ILM<br />
<strong>OCT</strong>: <strong>Retinal</strong> <strong>Layers</strong><br />
NFL GCL<br />
IPL<br />
OPL<br />
• Stratus<strong>OCT</strong> TM : >10 µm<br />
• Ultra High Resolution <strong>OCT</strong> (UHR-<strong>OCT</strong><br />
TM ): >5 µm<br />
ILM: Inner Limiting Membrane<br />
NFL: Nerve Fiber Layer<br />
GCL: Ganglion Cell Layer<br />
IS/OS<br />
RPE/CC<br />
IPL: Inner Plexiform Layer<br />
OPL: Outer Plexiform<br />
Choroid<br />
IS/OS: Junction of inner and outer<br />
photoreceptor segments<br />
RPE: <strong>Retinal</strong> Pigment Epithelium<br />
CC: Choriocapillaris<br />
• Ultra High Speed Spectral Domain <strong>OCT</strong> (SD-<strong>OCT</strong><br />
TM<br />
TM )<br />
<strong>OCT</strong> Clinical Applications: Macula<br />
Diabetic Macular Edema<br />
Macular Analysis<br />
• Six 6mm radial line scans<br />
• 30º view<br />
Line Scan<br />
• Single radial line<br />
<strong>Retinal</strong> <strong>OCT</strong> From Carl Zeiss<br />
Meditec<br />
How Does <strong>OCT</strong> work<br />
Reference Mirror<br />
Beam Splitter<br />
Light Source<br />
Stratus <strong>OCT</strong><br />
CirrusHD-<strong>OCT</strong><br />
Detector<br />
6
Time Domain <strong>OCT</strong> &<br />
Spectral Domain <strong>OCT</strong><br />
Time Domain and Spectral Domain<br />
Stratus <strong>OCT</strong><br />
Healthy Retina<br />
Healthy Retina<br />
Stratus <strong>OCT</strong> high-resolution line scan and the Cirrus HD-<strong>OCT</strong> scan<br />
reveal details of retinal structure<br />
AF – Diabetic Retinopathy<br />
Compare the Image<br />
Time<br />
Domain<br />
Spectral<br />
Domain<br />
Multiple Viewing Modes<br />
7
Diabetic Retinopathy<br />
Vision Loss From Diabetes<br />
• Leading cause of new blindness in the<br />
working age population<br />
• Leading cause of ESRD<br />
• Leading cause of LEA<br />
• Trimorbidities<br />
– Hyperglycemia<br />
–Hypertension<br />
– Dyslipidemia<br />
• Vitreous Hemorrhage<br />
• Traction <strong>Retinal</strong> Detachment<br />
•DME<br />
•NVI/NVG<br />
Case Studies - Patient EM<br />
THE ALL TOO<br />
COMMON SCENARIO<br />
PATIENT EM<br />
• 59-year-old African-American American male<br />
• Type 2 DM x 11 yrs<br />
• LEE: 1.5 yr<br />
• Pt complaint “having trouble seeing”<br />
• PMHx:<br />
– Uncontrolled HTN<br />
– + proteinuria<br />
– Last HbA1c = 11.1%<br />
• Meds: insulin, antihypertensive<br />
• VA 20/30 OU<br />
Patient EM Hemoglobin A1c<br />
Patient EM<br />
14<br />
12<br />
10<br />
8<br />
HbA1C (%)<br />
6<br />
4<br />
2<br />
0<br />
13.5<br />
12.5<br />
11.4<br />
10.1<br />
1997 2000 2003 2007<br />
• Cholesterol levels within normal limits<br />
• Elevated triglycerides and LDL levels<br />
• GFR - 50 [Albumin/Creatine level =<br />
231.6 µg/mg (Normal: 0 - 20 µg/mg)]<br />
Normal: 4.0 – 6.0%<br />
8
Estimated GFR<br />
Estimated Creatinine Clearance =<br />
(140 - age)<br />
Weight (kg)<br />
X X<br />
0.85 (if<br />
Serum Cr 72<br />
female)<br />
GFR of