Working Paper No. 6 - Health Policy Project
Working Paper No. 6 - Health Policy Project
Working Paper No. 6 - Health Policy Project

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Results<br />
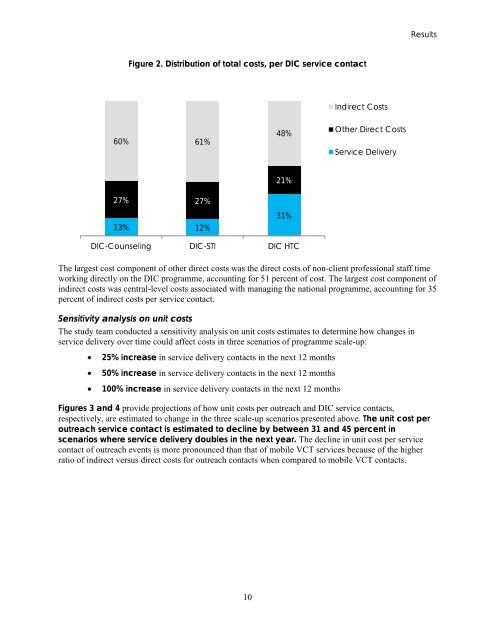
Figure 2. Distribution of total costs, per DIC service contact<br />
Indirect Costs<br />
60% 61%<br />
48%<br />
Other Direct Costs<br />
Service Delivery<br />
27% 27%<br />
13% 12%<br />
21%<br />
31%<br />
DIC-Counseling DIC-STI DIC HTC<br />
The largest cost component of other direct costs was the direct costs of non-client professional staff time<br />
working directly on the DIC programme, accounting for 51 percent of cost. The largest cost component of<br />
indirect costs was central-level costs associated with managing the national programme, accounting for 35<br />
percent of indirect costs per service contact.<br />
Sensitivity analysis on unit costs<br />
The study team conducted a sensitivity analysis on unit costs estimates to determine how changes in<br />
service delivery over time could affect costs in three scenarios of programme scale-up:<br />
• 25% increase in service delivery contacts in the next 12 months<br />
• 50% increase in service delivery contacts in the next 12 months<br />
• 100% increase in service delivery contacts in the next 12 months<br />
Figures 3 and 4 provide projections of how unit costs per outreach and DIC service contacts,<br />
respectively, are estimated to change in the three scale-up scenarios presented above. The unit cost per<br />
outreach service contact is estimated to decline by between 31 and 45 percent in<br />
scenarios where service delivery doubles in the next year. The decline in unit cost per service<br />
contact of outreach events is more pronounced than that of mobile VCT services because of the higher<br />
ratio of indirect versus direct costs for outreach contacts when compared to mobile VCT contacts.<br />
10