MMR/Meningitis Form (PDF)
MMR/Meningitis Form (PDF)
MMR/Meningitis Form (PDF)

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
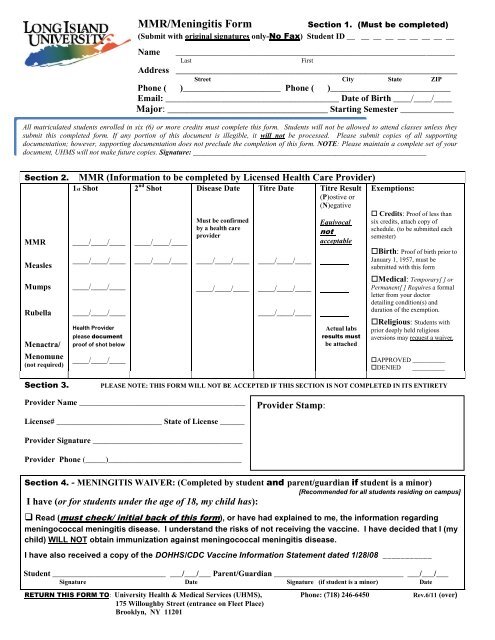
<strong>MMR</strong>/<strong>Meningitis</strong> <strong>Form</strong><br />
Section 1. (Must be completed)<br />
(Submit with original signatures only-No Fax) Student ID __ __ __ __ __ __ __ __ __<br />
Name _____________________________________________________________________<br />
Last<br />
First<br />
Address __________________________________________________________<br />
Street City State ZIP<br />
Phone ( )______________________ Phone ( )___________________________<br />
Email: _______________________________________ Date of Birth ____/____/____<br />
Major: _________________________________ Starting Semester ____________<br />
All matriculated students enrolled in six (6) or more credits must complete this form. Students will not be allowed to attend classes unless they<br />
submit this completed form. If any portion of this document is illegible, it will not be processed. Please submit copies of all supporting<br />
documentation; however, supporting documentation does not preclude the completion of this form. NOTE: Please maintain a complete set of your<br />
document, UHMS will not make future copies. Signature: ________________________________________________________________<br />
Section 2. <strong>MMR</strong> (Information to be completed by Licensed Health Care Provider)<br />
1st Shot 2 nd Shot Disease Date Titre Date Titre Result<br />
(P)ostive or<br />
(N)egative<br />
<strong>MMR</strong> ____/____/____ ____/____/____<br />
Measles<br />
Must be confirmed<br />
by a health care<br />
provider<br />
____/____/____ ____/____/____ ____/____/____ ____/____/____<br />
Mumps ____/____/____ ____/____/____ ____/____/____<br />
Rubella ____/____/____ ____/____/____<br />
Menactra/<br />
Menomune<br />
(not required)<br />
Health Provider<br />
please document<br />
proof of shot below<br />
____/____/____<br />
Equivocal<br />
not<br />
acceptable<br />
Actual labs<br />
results must<br />
be attached<br />
Exemptions:<br />
Credits: Proof of less than<br />
six credits, attach copy of<br />
schedule. (to be submitted each<br />
semester)<br />
Birth: Proof of birth prior to<br />
January 1, 1957, must be<br />
submitted with this form<br />
Medical: Temporary[ ] or<br />
Permanent[ ] Requires a formal<br />
letter from your doctor<br />
detailing condition(s) and<br />
duration of the exemption.<br />
Religious: Students with<br />
prior deeply held religious<br />
aversions may request a waiver.<br />
APPROVED __________<br />
DENIED __________<br />
Section 3.<br />
PLEASE NOTE: THIS FORM WILL NOT BE ACCEPTED IF THIS SECTION IS NOT COMPLETED IN ITS ENTIRETY<br />
Provider Name _________________________________________<br />
License# __________________________ State of License ______<br />
Provider Stamp:<br />
Provider Signature _____________________________________<br />
Provider Phone (_____)_________________________________<br />
Section 4. - MENINGITIS WAIVER: (Completed by student and parent/guardian if student is a minor)<br />
[Recommended for all students residing on campus]<br />
I have (or for students under the age of 18, my child has):<br />
Read (must check/ initial back of this form), or have had explained to me, the information regarding<br />
meningococcal meningitis disease. I understand the risks of not receiving the vaccine. I have decided that I (my<br />
child) WILL NOT obtain immunization against meningococcal meningitis disease.<br />
I have also received a copy of the DOHHS/CDC Vaccine Information Statement dated 1/28/08 ___________<br />
Student ____________________________ ___/___/___ Parent/Guardian ________________________________ ___/___/___<br />
Signature Date Signature (if student is a minor) Date<br />
RETURN THIS FORM TO: University Health & Medical Services (UHMS), Phone: (718) 246-6450 Rev.6/11 (over)<br />
175 Willoughby Street (entrance on Fleet Place)<br />
Brooklyn, NY 11201
Section One: This section is to be filled our completely by the student. Your student identification number (SID) is required in order to process your<br />
information; no other defining information will be accepted. The demographic information is used for filing purposes and future communications,<br />
please print neatly. We require a local address, telephone number and an active email address. NOTE: Only three attempts will be made to inform<br />
you of missing information before a hold is placed on your account, which may prevent registration or continued access to classes.<br />
Section Two: <strong>MMR</strong> Requirements<br />
Section Four: MENINGOCOCCAL MENINGITIS Requirements<br />
(To be completed by a Licensed Health Care Provider)<br />
N.Y.S. Public Health Law 2165 requires college students enrolled for six<br />
or more chargeable credits to show proof of immunization against<br />
Measles, Mumps, and Rubella. Students born prior to January 1, 1957<br />
are exempt from this requirement.<br />
On July 22, 2003, Governor Pataki signed New York State Public Health<br />
Law (NYS PHL) §2167 requiring institutions, including colleges and<br />
universities, to distribute information about meningococcal disease and<br />
vaccination to all students meeting the enrollment criteria, whether they<br />
live on or off campus. This law is effective as of August 15, 2003.<br />
<strong>MMR</strong> (Combined Live Measles, Mumps, and Rubella<br />
Immunization). The first dose no more than 4 days prior to the first<br />
birthday. The second dose a minimum of 28 days after the first<br />
dose.<br />
Single Live Measles Immunization. The first dose no more than 4<br />
days prior to the first birthday. The second dose a minimum of 28<br />
days after the first dose. Physician statement of Measles disease<br />
(exact date required) is acceptable.<br />
Single Live Mumps Immunization. Dose no more than 4 days prior<br />
to the first birthday. Physician statement of Mumps disease (exact<br />
date required) is acceptable.<br />
Single Live Rubella (German Measles) Immunization. Dose no<br />
more than 4 days prior to the first birthday. Diagnosis of Rubella<br />
(German Measles) is not acceptable as proof of immunity.<br />
<br />
Serologic evidence of immunity (Titre, copy of actual report must<br />
EXEMPTIONS:<br />
be attached) is acceptable for Measles, Mumps, and Rubella.<br />
EQUIVOCAL TITRES ARE NOT ACCEPTABLE.<br />
If you are requesting an exemption, you must provide the requested<br />
proof and/or complete the required form(s).<br />
automatic.<br />
Section Three: Physician Information<br />
Approval is not<br />
Please note this section, must be filled out in its’ entirety, and is only<br />
accepted with original signatures. All the information in this section is<br />
required. <strong>Form</strong>s missing information from this section will not be<br />
accepted.<br />
<br />
<br />
<br />
<br />
<br />
<br />
Provider Name – Must be clearly printed and/or provided on via their<br />
stamp in the allocated area (stamp that cannot be read will be<br />
returned);<br />
License# - Must be clearly printed and/or provided via the doctor’s<br />
stamp;<br />
State of License – Must be provided and clearly printed in the<br />
allocated area;<br />
Provider Signature – No forms will be accepted without a<br />
doctor’s signature matching the license # provided;<br />
Provider Phone - Must be provided and clearly printed in the<br />
allocated area;<br />
Provider Stamp – This is the doctor’s stamp and not the facility, the<br />
stamp should be clearly placed in the space allocated;<br />
Colleges in New York State are required to maintain a record of the<br />
following for each student:<br />
1 A response to receipt of meningococcal disease and vaccine<br />
information signed by the student or student’s parent or guardian.<br />
This must include information on the availability and cost of<br />
meningococcal meningitis vaccine;<br />
AND EITHER<br />
A record of meningococcal meningitis immunization within the past<br />
10 years; OR<br />
<br />
An acknowledgement of meningococcal disease risks and refusal of<br />
meningococcal meningitis immunization signed by the student or<br />
student’s parent or guardian.<br />
MENINGOCOCCAL DISEASE RISKS:<br />
<strong>Meningitis</strong> is rare. However, when it strikes, its flu-like symptoms<br />
make diagnosis difficult. If not treated early, meningitis can lead to<br />
swelling of the fluid surrounding the brain and spinal column as well as<br />
severe and permanent disabilities, such as hearing loss, brain damage,<br />
seizures, limb amputation, and even death.<br />
Cases of meningitis among teens and young adults 15 to 24 years<br />
of age (the age of most college students) have more than doubled since<br />
1991. The disease strikes about 3,000 Americans each year and claims<br />
about 300 lives. Between 100 and 125 meningitis cases occur on college<br />
campuses and as many as 15 students will die from the disease.<br />
In February 2005, the CDC recommended a new vaccine, known as<br />
Menactra for use to prevent meningococcal disease in people 11-55<br />
years of age.<br />
The previously licensed version of this vaccine,<br />
Menomune is still available for this age group, as well as for children 2-<br />
10 years old and adults older than 55 years. Both vaccines are 90%<br />
effective in preventing the 4 kinds of the meningococcus germ (types A,<br />
C, Y, W-135) which cause about 70% of the disease in the United States.<br />
<strong>Meningitis</strong> vaccine is NOW available FREE via University Health &<br />
Medical Services and its partner The Brooklyn Hospital Center. It<br />
should also be available via your private health care provider. Cost<br />
varies along with coverage and range from $80-150.00.<br />
You can also find information about the disease at the New York State<br />
Department of Health Website: http://www.health.state.ny.us/ or the<br />
American College Health Association (ACHA) Website:<br />
WWW.ACHA.ORG.<br />
NOTE: This Section must be filled out by a verifiable licensed provider,<br />
preferably a MD, whose signature, stamp, and license is clearly<br />
documented on the form,<br />
I have read the above information and understand the risk<br />
of not having the vaccine. I have decided not to obtain<br />
immunization against the meningococcal meningitis disease.<br />
__________________________________________________<br />
Signature:<br />
Please note that according to NYS Public Health Law, no institutions shall permit any student to attend the institution in excess of 30 days without<br />
complying with this law. The 30-day period may be extended to 45 days for out-of-state student by completing a request for extension form.