executive summary - The Alliance
executive summary - The Alliance
executive summary - The Alliance

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
A<br />
EXECUTIVE SUMMARY<br />
ACA UPDATE: RETURN OR EXCHANGE<br />
AUGUST 21, 2013<br />
Employers have much to do – and much to monitor – as Affordable Care Act (ACA) deadlines draw near and state and<br />
federal governments prepare to launch insurance exchanges.<br />
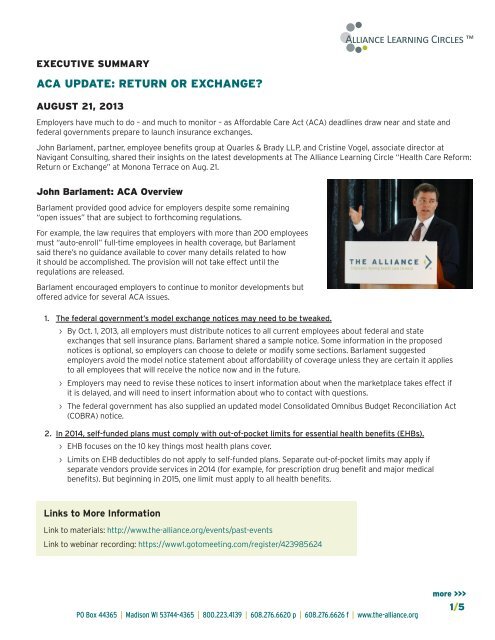
John Barlament, partner, employee benefits group at Quarles & Brady LLP, and Cristine Vogel, associate director at<br />
Navigant Consulting, shared their insights on the latest developments at <strong>The</strong> <strong>Alliance</strong> Learning Circle “Health Care Reform:<br />
Return or Exchange” at Monona Terrace on Aug. 21.<br />
John Barlament: ACA Overview<br />
Barlament provided good advice for employers despite some remaining<br />
“open issues” that are subject to forthcoming regulations.<br />
For example, the law requires that employers with more than 200 employees<br />
must “auto-enroll” full-time employees in health coverage, but Barlament<br />
said there’s no guidance available to cover many details related to how<br />
it should be accomplished. <strong>The</strong> provision will not take effect until the<br />
regulations are released.<br />
Barlament encouraged employers to continue to monitor developments but<br />
offered advice for several ACA issues.<br />
1. <strong>The</strong> federal government’s model exchange notices may need to be tweaked.<br />
››<br />
By Oct. 1, 2013, all employers must distribute notices to all current employees about federal and state<br />
exchanges that sell insurance plans. Barlament shared a sample notice. Some information in the proposed<br />
notices is optional, so employers can choose to delete or modify some sections. Barlament suggested<br />
employers avoid the model notice statement about affordability of coverage unless they are certain it applies<br />
to all employees that will receive the notice now and in the future.<br />
››<br />
Employers may need to revise these notices to insert information about when the marketplace takes effect if<br />
it is delayed, and will need to insert information about who to contact with questions.<br />
››<br />
<strong>The</strong> federal government has also supplied an updated model Consolidated Omnibus Budget Reconciliation Act<br />
(COBRA) notice.<br />
2. In 2014, self-funded plans must comply with out-of-pocket limits for essential health benefits (EHBs).<br />
››<br />
EHB focuses on the 10 key things most health plans cover.<br />
››<br />
Limits on EHB deductibles do not apply to self-funded plans. Separate out-of-pocket limits may apply if<br />
separate vendors provide services in 2014 (for example, for prescription drug benefit and major medical<br />
benefits). But beginning in 2015, one limit must apply to all health benefits.<br />
Links to More Information<br />
Link to materials: http://www.the-alliance.org/events/past-events<br />
Link to webinar recording: https://www1.gotomeeting.com/register/423985624<br />
PO Box 44365 | Madison WI 53744-4365 | 800.223.4139 | 608.276.6620 p | 608.276.6626 f | www.the-alliance.org<br />
more >>><br />
1/5
John Barlament: Open Issues Abound, continued:<br />
3. Employers should put into writing as soon as possible which definition of the EHB will be used<br />
by their health benefits.<br />
››<br />
Self-funded plans are not required to cover EHBs, but if they do then they must not subject them to annual<br />
and lifetime limits.<br />
››<br />
EHB regulations allow employers to use any available benchmark option, such as a specific state’s EHB.<br />
››<br />
Since EHB definitions vary from state to state, employers should pick the definition that best matches<br />
their plan.<br />
››<br />
Beginning in 2014, there are limits on out-of-pocket maximums for EHBs.<br />
4. Be aware of changes related to the Summary of Benefits and Coverage (SBC), fees and provider<br />
non-discrimination rules.<br />
››<br />
<strong>The</strong> government has tweaked SBC rules and provided an updated SBC template online.<br />
››<br />
Form 720 has been developed to allow employers to report their Patient-Centered Outcomes Research<br />
Institute (PCORI) fee of $1 per covered life.<br />
››<br />
Self-funded employers must also pay a reinsurance fee of $63 per covered life that will probably be due at the<br />
end of 2014 or beginning of 2015.<br />
››<br />
Rules that forbid “discriminating” against licensed providers are subject to interpretation. An example is<br />
failing to cover massages from a licensed massage therapist but covering them when delivered by a physical<br />
therapist. Barlament urged employers to review their health plans to find these situations and address them.<br />
››<br />
A rule requiring coverage of clinical trials for “covered individuals” is unclear.<br />
5. Review insurance plans to make sure waiting periods meet the rules.<br />
››<br />
A waiting period of exactly 90 days is used for eligible employees; three months is not acceptable as a<br />
substitute. Coverage must begin on the 91st day.<br />
››<br />
<strong>The</strong> “hours of service” eligibility requirement is capped at 1,200 hours.<br />
6. Be aware of new wellness plan rules.<br />
››<br />
Regulations issued June 3, 2013, contain significant changes.<br />
››<br />
Incentives or disincentives worth 30 percent of the annual total cost of individual premiums can be offered,<br />
which increases to 50 percent if it relates to tobacco usage.<br />
››<br />
Rules differ based on whether a health-contingent wellness plan is built on participation, such as a walking<br />
program, or on outcomes, such as lowering cholesterol. Be prepared to offer a reasonable alternative to<br />
outcome-based wellness program requirements so all employees can earn the incentive.<br />
7. Health reform regulations impact Health Insurance Portability and Accountability Act (HIPAA) rules intended<br />
to safeguard “protected health information” about individual’s health and health claims.<br />
››<br />
Make sure agreements with vendors and other business associates comply with HIPAA rules.<br />
››<br />
Employers must certify by year-end that they comply with HIPAA rules.<br />
››<br />
If a breach occurs, follow the new rules to notify authorities. Document any type of breach where protected<br />
information leaves the organization.<br />
››<br />
Update policies and procedures; the notice of privacy rights; and agreements with business associates to<br />
follow the latest rules for maintaining and sharing information.<br />
PO Box 44365 | Madison WI 53744-4365 | 800.223.4139 | 608.276.6620 p | 608.276.6626 f | www.the-alliance.org<br />
more >>><br />
2/5
John Barlament: Open Issues Abound, continued:<br />
8. <strong>The</strong> U.S. Supreme Court’s “Windsor” decision that overturned the<br />
Defense of Marriage Act on June 26, 2013, offers new rights to<br />
same-sex couples.<br />
››<br />
Federal law now defers to state law to recognize which<br />
individuals are in a “marriage” and who is a “spouse.” Samesex<br />
marriages are recognized in 12 states and the District of<br />
Columbia.<br />
››<br />
<strong>The</strong>re is still some confusion about which state laws apply in<br />
specific situations and whether employers in specific situations<br />
are required to offer benefits to same-sex couples.<br />
››<br />
Expect additional lawsuits and guidance to provide more<br />
information. Barlament predicted that a “liberal interpretation of<br />
who is married” could emerge.<br />
››<br />
Employers may need to adjust how they handle taxes, COBRA notices and other benefits.<br />
››<br />
Employers can prepare by reviewing their plan’s definition of a spouse or domestic partner;<br />
selecting a clear definition of a spouse; updating plan documents; and working with vendors to<br />
implement changes.<br />
Cristine Vogel: Exchanges Are An Emerging Insurance Marketplace<br />
Recognizing Same-Sex Marriage<br />
Same-sex marriages are recognized in:<br />
California<br />
Connecticut<br />
Delaware<br />
District of Columbia<br />
Iowa<br />
Maryland<br />
Maine<br />
Last-minute scrambling is the way Cristine Vogel describes state and federal insurance exchanges that will serve as<br />
“Marketplaces” for individuals and small employers under the ACA. Vogel said there’s still “an awful lot of rearranging”<br />
taking place in the individual and the Small Business Health Options Program (SHOP) Marketplaces, otherwise known as<br />
the public exchanges.<br />
Purchasers will have private insurance options both “inside” and “outside”<br />
the state and federal Marketplaces, but subsidies will only be available from<br />
“Qualified Health Plans” approved to sell inside the exchange. That applies<br />
to every state except Vermont, which is aiming for a single payer plan and so<br />
will not have an “outside” market. Each state may also require that insurance<br />
providers offer specific benefits through its EHB, which is used to standardize<br />
health plans within each state so people know which core benefits are covered.<br />
ACA rules apply to both qualified health plans offered inside the SHOP<br />
Marketplace and to plans from outside sources, with the exception of<br />
grandfathered plans that are exempt from certain ACA provisions as long as they<br />
remain unchanged.<br />
1. While exchanges are aiming to begin enrolling individuals on Oct. 1, she “wouldn’t be surprised<br />
if that was delayed.”<br />
››<br />
A short delay would have minimal impact since coverage does not take effect until Jan. 1, 2014.<br />
››<br />
Open enrollment in 2015 will be held Oct. 15 to Dec. 7; special rules will allow people who lose<br />
work-related benefits to apply outside the open enrollment period. Those that enroll by Dec. 15<br />
will have plans that begin on January 1.<br />
Massachusetts<br />
Minnesota<br />
New York<br />
New Hampshire<br />
Rhode Island<br />
Vermont<br />
Washington<br />
PO Box 44365 | Madison WI 53744-4365 | 800.223.4139 | 608.276.6620 p | 608.276.6626 f | www.the-alliance.org<br />
more >>><br />
3/5
Exchanges: An Emerging Insurance Marketplace, continued:<br />
2. SHOP Marketplaces are still in development, including the infrastructures to support them.<br />
››<br />
Eighteen states will have state-based marketplaces. <strong>The</strong> federal government has yet to certify<br />
most of these marketplaces, although many have obtained state-level Department of Insurance<br />
approvals that may be an indicator of their ability to gain federal certification.<br />
››<br />
Seven states have “partnership” marketplaces that will be run with U.S.Department of Health and<br />
Human Services (HHS) oversight and preparation, including Illinois and Iowa.<br />
››<br />
Twenty-six states, including Wisconsin, have federal-facilitated marketplaces, which again have<br />
HHS oversight.<br />
3. An eligibility process determines whether individuals will receive federal subsidies.<br />
››<br />
Eligibility is based on income, whether the individual is incarcerated, whether employer-based<br />
coverage is available and whether the applicant lives within a specific marketplace.<br />
››<br />
Some individuals may be directed into Medicaid. If they are eligible for Medicaid and choose to<br />
instead go to the marketplace, they are ineligible for federal subsidies for coverage.<br />
››<br />
Individuals that are not offered affordable employer coverage will receive a premium tax credit<br />
if their income is between 100 and 400 percent of the federal poverty level. A cost-sharing<br />
reduction is available for people with an income of 100 to 250 percent of the federal poverty level<br />
who are enrolled in a silver plan. Special rules cover individuals with American Indian status.<br />
››<br />
Individuals who are eligible for SHOP-qualified health plans must work for an employer with less<br />
than 50 FTEs.<br />
››<br />
Only individuals who meet certain criteria can<br />
purchase a catastrophic-only insurance plan. <strong>The</strong>se<br />
individuals must be under age 30 and must have<br />
certified that they are exempt from the individual<br />
mandate. <strong>The</strong>se exemptions are granted by the HHS<br />
for religious beliefs or financial hardship and are likely<br />
to be hard to obtain, Vogel said.<br />
4. Actuarial Value (AV) standards will help consumers<br />
compare health plans.<br />
››<br />
Vogel said it’s hard for consumers to shop for<br />
insurance today; AV will make it easier by helping them<br />
truly compare plans.<br />
››<br />
Non-grandfathered individual and small group plans<br />
inside and outside the marketplace must meet specific<br />
AV targets and grouped by “precious metal” category.<br />
››<br />
<strong>The</strong> percentage of total average cost that must be<br />
covered is 60 percent for a bronze plan; 70 percent<br />
for silver; 80 percent for gold; and 90 percent for<br />
platinum.<br />
››<br />
Premium tax credits will be based on each exchange’s<br />
silver plan with the second-lowest cost.<br />
EHB Required Categories<br />
Essential Health Benefits (EHBs) can vary by state,<br />
but they must all provide a minimum package of<br />
benefits that covers these categories:<br />
››<br />
Ambulatory patient services<br />
››<br />
Emergency services<br />
››<br />
Hospitalizations<br />
››<br />
Maternity and newborn care<br />
››<br />
Mental health and substance use<br />
disorders<br />
››<br />
Rehabilitative and habilitative services<br />
and devices<br />
››<br />
Laboratory services<br />
››<br />
Prescription drugs<br />
››<br />
Preventive and wellness services and<br />
chronic disease management<br />
››<br />
Pediatric services, including oral and<br />
vision care<br />
Source: Cristine Vogel, Navigant Consulting<br />
more >>><br />
4/5<br />
PO Box 44365 | Madison WI 53744-4365 | 800.223.4139 | 608.276.6620 p | 608.276.6626 f | www.the-alliance.org
Exchanges: An Emerging Insurance Marketplace, continued:<br />
5. <strong>The</strong>re will still be an insurance coverage “gap” and some individuals are likely to have difficulty<br />
complying with ACA rules.<br />
››<br />
Some people will earn too much to qualify for Medicaid and yet fail to qualify for the subsidy<br />
because they earn under 100 percent of the federal poverty level. For these individuals, the<br />
only option would be to go to the marketplace and apply for a certificate of exemption from the<br />
individual mandate to obtain insurance coverage.<br />
››<br />
When individuals qualify for a tax credit for insurance it is paid directly to the insurance issuer<br />
each month. If consumers fail to report/update their actual income for each family member,<br />
they could end up owing money to the Internal Revenue Service. Low-income tax filers who have<br />
simple returns are most likely to be impacted.<br />
Vogel noted that much hinges on the individual mandate that requires nearly every American to have health insurance<br />
beginning in 2014. She called this the “glue” for the ACA. Yet it is proving difficult to get the word out to individuals about<br />
the need to enroll in the exchanges. That is just one of the many challenges linked to implementing the ACA by Jan. 1, 2014<br />
for individuals and employers alike.<br />
Individual Mandate Penalties<br />
<strong>The</strong> penalty for individuals who are not exempt and who<br />
fail to get insurance coverage is the greater of either:<br />
››<br />
A percentage of income.<br />
»»<br />
1 percent in 2014<br />
»»<br />
2 percent in 2015<br />
»»<br />
2.5 percent in 2016 and beyond<br />
››<br />
A flat dollar amount paid on each taxpayer and<br />
dependent, which will be adjusted for inflation.<br />
»»<br />
$95 in 2014<br />
»»<br />
$325 in 2015<br />
»»<br />
$695 in 2016 and beyond<br />
»»<br />
Capped at 300 percent of the annual flat amount<br />
for the total family<br />
››<br />
<strong>The</strong> penalty for noncompliance cannot exceed the<br />
national average for a bronze-level plan.<br />
Source: Cristine Vogel, Navigant Consulting<br />
PO Box 44365 | Madison WI 53744-4365 | 800.223.4139 | 608.276.6620 p | 608.276.6626 f | www.the-alliance.org<br />
<strong>The</strong> <strong>Alliance</strong> moves health care forward by controlling costs, improving quality, and engaging individuals in their health. An employer-owned, not-for-profit<br />
cooperative, our 180 members provide coverage to more than 80,000 individuals in Wisconsin, Illinois, and Iowa.<br />
5/5