Sagoff Breast Imaging & Diagnostic Centre ... - Faulkner Hospital
Sagoff Breast Imaging & Diagnostic Centre ... - Faulkner Hospital
Sagoff Breast Imaging & Diagnostic Centre ... - Faulkner Hospital

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
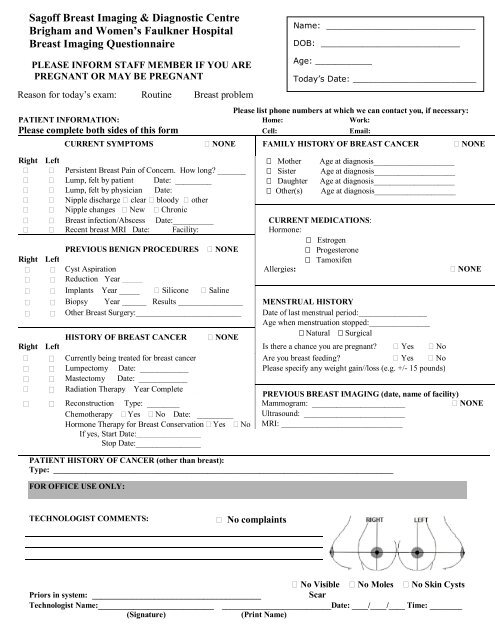
<strong>Sagoff</strong> <strong>Breast</strong> <strong>Imaging</strong> & <strong>Diagnostic</strong> <strong>Centre</strong><br />
Brigham and Women’s <strong>Faulkner</strong> <strong>Hospital</strong><br />
<strong>Breast</strong> <strong>Imaging</strong> Questionnaire<br />
Name: _____________________________<br />
DOB: ___________________________<br />
PLEASE INFORM STAFF MEMBER IF YOU ARE<br />
PREGNANT OR MAY BE PREGNANT<br />
Reason for today’s exam: Routine <strong>Breast</strong> problem<br />
Please list phone numbers at which we can contact you, if necessary:<br />
PATIENT INFORMATION: Home: Work:<br />
Please complete both sides of this form Cell: Email:<br />
CURRENT SYMPTOMS NONE FAMILY HISTORY OF BREAST CANCER NONE<br />
Right Left Mother Age at diagnosis____________________<br />
Persistent <strong>Breast</strong> Pain of Concern. How long _______ Sister Age at diagnosis____________________<br />
Lump, felt by patient Date: _________ Daughter Age at diagnosis____________________<br />
Lump, felt by physician Date: _________ Other(s) Age at diagnosis____________________<br />
Nipple discharge clear bloody other<br />
Nipple changes New Chronic<br />
<strong>Breast</strong> infection/Abscess Date:__________ CURRENT MEDICATIONS:<br />
Recent breast MRI Date: Facility: Hormone:<br />
Estrogen<br />
PREVIOUS BENIGN PROCEDURES NONE Progesterone<br />
Right Left<br />
Tamoxifen<br />
Cyst Aspiration Allergies: NONE<br />
Reduction Year _____<br />
Implants Year _____ Silicone Saline<br />
Biopsy Year ______ Results ________________ MENSTRUAL HISTORY<br />
Other <strong>Breast</strong> Surgery:__________________________ Date of last menstrual period:_________________<br />
Age when menstruation stopped:_______________<br />
HISTORY OF BREAST CANCER NONE<br />
Natural Surgical<br />
Right Left Is there a chance you are pregnant Yes No<br />
Currently being treated for breast cancer Are you breast feeding Yes No<br />
Lumpectomy Date: ____________ Please specify any weight gain//loss (e.g. +/- 15 pounds)<br />
Mastectomy Date: ____________<br />
Radiation Therapy Year Complete ______<br />
PREVIOUS BREAST IMAGING (date, name of facility)<br />
Reconstruction Type: ________ Mammogram: _______________________ NONE<br />
Chemotherapy Yes No Date: _________ Ultrasound: _________________________<br />
Hormone Therapy for <strong>Breast</strong> Conservation Yes No MRI: ______________________________<br />
If yes, Start Date:________________<br />
Stop Date:________________<br />
PATIENT HISTORY OF CANCER (other than breast):<br />
Type: ____________________________________________________________________________________<br />
FOR OFFICE USE ONLY:<br />
Age: ___________<br />
Today’s Date: ________________________<br />
TECHNOLOGIST COMMENTS:<br />
No complaints<br />
PLTE<br />
No Visible No Moles No Skin Cysts<br />
Priors in system: ______________________________________<br />
Scar<br />
Technologist Name:__________________________ ___________________________Date: ____/____/____ Time: ________<br />
(Signature)<br />
(Print Name)
Please list medications you are currently taking if you are scheduled for a procedure (i.e. biopsy, cyst<br />
aspiration, wire localization):<br />
Patient Choice<br />
Applies only to patients scheduled for a screening mammogram Monday-Friday, before 4 p.m.<br />
We know your time is valuable, and so we want to offer you a choice regarding how you receive your<br />
mammogram results today 1 . Please choose the option that best meets your needs today by checking the<br />
appropriate box below:<br />
Screening mammogram, results mailed to you (Appointment time ~30-45 minutes)<br />
Choose this option if you would like to leave after your screening mammogram is completed,<br />
and we will mail your results letter to you within 7 days. If the Radiologist requests additional<br />
diagnostic imaging 2 you will be called back for an additional appointment. If you are asked to<br />
return for a diagnostic mammogram 3 , you will meet with the Radiologist during the appointment.<br />
Screening mammogram, results given same day (Appointment Time ~60-90 minutes)<br />
Choose this option if you would like to receive your results today. A staff member will give you<br />
a results letter after the Radiologist has read your exam. If you wish to meet with the Radiologist<br />
who read your exam, please inform a staff member at any time during the course of your visit. If<br />
a Radiologist requests additional diagnostic imaging 2 , the exam will be completed today 3 .<br />
Note to Patient:<br />
(1) On the day of your annual screening mammogram appointment, if you present with a lump or any other sign<br />
or symptom of breast disease, a diagnostic mammogram will be performed instead of a screening mammogram.<br />
(2) Approximately 10% of patients having a screening mammogram will have additional views, also known as<br />
a diagnostic mammogram, requested by a Radiologist. <strong>Diagnostic</strong> mammograms, and sometimes breast<br />
ultrasound, are obtained when the radiologist needs to further evaluate a potential abnormality. Appointments<br />
may be longer than the stated time above if additional imaging is needed.<br />
(3) Though insurance companies will cover a screening mammogram, you may be responsible for charges<br />
associated with a diagnostic mammogram or breast ultrasound. We encourage you to contact your insurance<br />
carrier in advance of your screening appointment to determine whether or not diagnostic mammograms and<br />
breast ultrasound are covered services.<br />
Are you dizzy or weak today Yes No<br />
Do you walk with assistance Yes No<br />
Have you had any recent falls Yes No<br />
______________________________________________________________________________________<br />
Please sign and date<br />
(Date)<br />
Thank you.<br />
05/13