DHHS 3056-ADAP Authorization Application (Nov 2012) - Epi
DHHS 3056-ADAP Authorization Application (Nov 2012) - Epi
DHHS 3056-ADAP Authorization Application (Nov 2012) - Epi

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
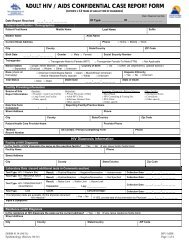
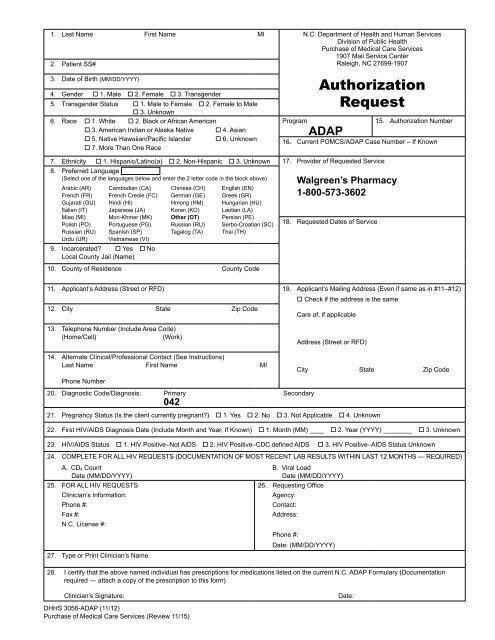
1. Last Name<br />
2. Patient SS#<br />
First Name MI N.C. Department of Health and Human Services<br />
Division of Public Health<br />
Purchase of Medical Care Services<br />
1907 Mail Service Center<br />
Raleigh, NC 27699-1907<br />
3. Date of Birth (MM/DD/YYYY)<br />
4. Gender 1. Male 2. Female 3. Transgender<br />
5. Transgender Status 1. Male to Female 2. Female to Male<br />
3. Unknown<br />
6. Race 1. White 2. Black or African American<br />
3. American Indian or Alaska Native 4. Asian<br />
5. Native Hawaiian/Pacific Islander 6. Unknown<br />
7. More Than One Race<br />
<strong>Authorization</strong><br />
Request<br />
Program 15. <strong>Authorization</strong> Number<br />
<strong>ADAP</strong><br />
16. Current POMCS/<strong>ADAP</strong> Case Number – If Known<br />
7. Ethnicity 1. Hispanic/Latino(a) 2. Non-Hispanic 3. Unknown 17. Provider of Requested Service<br />
8. Preferred Language<br />
(Select one of the languages below and enter the 2 letter code in the block above)<br />
Arabic (AR) Cambodian (CA) Chinese (CH) English (EN)<br />
French (FR) French Creole (FC) German (GE) Greek (GR)<br />
Gujarati (GU) Hindi (HI) Hmong (HM) Hungarian (HU)<br />
Italian (IT) Japanese (JA) Koran (KO) Laotian (LA)<br />
Miao (MI) Mon-Khmer (MK) Other (OT) Persian (PE)<br />
Polish (PO) Portuguese (PG) Russian (RU) Serbo-Croatian (SC)<br />
Russian (RU) Spanish (SP) Tagalog (TA) Thai (TH)<br />
Urdu (UR) Vietnamese (VI)<br />
9. Incarcerated Yes No<br />
Local County Jail (Name)<br />
10. County of Residence County Code<br />
Walgreen’s Pharmacy<br />
1-800-573-3602<br />
18. Requested Dates of Service<br />
11. Applicant’s Address (Street or RFD) 19. Applicant’s Mailing Address (Even if same as in #11–#12)<br />
12. City State Zip Code<br />
Check if the address is the same<br />
Care of, if applicable<br />
13. Telephone Number (Include Area Code)<br />
(Home/Cell)<br />
(Work)<br />
Address (Street or RFD)<br />
14. Alternate Clinical/Professional Contact (See Instructions)<br />
Last Name First Name MI<br />
Phone Number<br />
20. Diagnostic Code/Diagnosis: Primary Secondary<br />
042<br />
City State Zip Code<br />
21. Pregnancy Status (Is the client currently pregnant) 1. Yes 2. No 3. Not Applicable 4. Unknown<br />
22. First HIV/AIDS Diagnosis Date (Include Month and Year, If Known) 1. Month (MM) ____ 2. Year (YYYY) ________ 3. Unknown<br />
23. HIV/AIDS Status 1. HIV Positive–Not AIDS 2. HIV Positive–CDC defined AIDS 3. HIV Positive–AIDS Status Unknown<br />
24. COMPLETE FOR ALL HIV REQUESTS (DOCUMENTATION OF MOST RECENT LAB RESULTS WITHIN LAST 12 MONTHS — REQUIRED)<br />
A. CD 4 Count<br />
Date (MM/DD/YYYY)<br />
25. FOR ALL HIV REQUESTS<br />
Clinician’s Information:<br />
Phone #:<br />
Fax #:<br />
N.C. License #:<br />
27. Type or Print Clinician’s Name<br />
B. Viral Load<br />
Date (MM/DD/YYYY)<br />
26. Requesting Office<br />
Agency:<br />
Contact:<br />
Address:<br />
Phone #:<br />
Date: (MM/DD/YYYY)<br />
28. I certify that the above named individual has prescriptions for medications listed on the current N.C. <strong>ADAP</strong> Formulary (Documentation<br />
required — attach a copy of the prescription to this form)<br />
Clinician’s Signature:<br />
<strong>DHHS</strong> <strong>3056</strong>-<strong>ADAP</strong> (11/12)<br />
Purchase of Medical Care Services (Review 11/15)<br />
Date:
Instructions for <strong>Authorization</strong> Request<br />
All form fields must be completed or form will be pended.<br />
PURPOSE<br />
This form is used to request authorization for the <strong>ADAP</strong> program.<br />
Processing time is reduced when this form is legible and complete. If requested, additional information must be<br />
received within six months. Incomplete forms will be pended.<br />
INSTRUCTIONS FOR COMPLETING CERTAIN ITEMS ON THIS FORM<br />
9. If applicant/patient is incarcerated, check the box and indicate where applicant is currently residing.<br />
NOTE: Patients who are incarcerated in a state or federal prison cannot participate in the <strong>ADAP</strong><br />
Program.<br />
11. If applicant/patient provides an alternate mailing address (see #24) — all correspondence should be sent<br />
to that address.<br />
14. This alternate clinical/professional contact will be contacted by the <strong>ADAP</strong> office and/or pharmacy if the<br />
interviewer on file (the person submitting this form) is not the best clinical/professional contact.<br />
15. For POMCS use only. Do not complete this item.<br />
18. Will be the authorization date unless another date is requested and specified in this box.<br />
20. If applicable, enter secondary diagnosis code.<br />
28. Must be signed and dated or the application will be pended.<br />
Mail (do not Fax) this application and documentation to:<br />
<strong>DHHS</strong> Division of Public Health, Purchase of Medical Care Services, 1907 Mail Service Center, Raleigh, NC 27699-1907<br />
<strong>DHHS</strong> <strong>3056</strong>-<strong>ADAP</strong> (11/12)<br />
Purchase of Medical Care Services (Review 11/15)