Rapid health facility and community needs assessment; Hodeida ...
Rapid health facility and community needs assessment; Hodeida ...
Rapid health facility and community needs assessment; Hodeida ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Rapid</strong> <strong>health</strong> <strong>facility</strong> <strong>and</strong> <strong>community</strong><br />
<strong>needs</strong> <strong>assessment</strong>; <strong>Hodeida</strong>, Yemen<br />
Contents<br />
1 Executive Summary ............................................................................................................ 2<br />
2 Context <strong>and</strong> Background .................................................................................................... 4<br />
3 Key Objectives: .................................................................................................................. 4<br />
4 Methodology for the <strong>assessment</strong> ........................................................................................ 5<br />
4.1 Sampling Frame <strong>and</strong> methods ...................................................................................... 5<br />
4.2 Tools for data collection: ............................................................................................. 6<br />
5 Key Findings <strong>and</strong> Results: .................................................................................................. 6<br />
5.1 The Building blocks of Health Systems in <strong>Hodeida</strong>: ................................................... 6<br />
5.1.1 Governance: .......................................................................................................... 6<br />
5.1.2 Drugs, Equipment <strong>and</strong> infrastructure: .................................................................. 7<br />
5.1.3 HMIS .................................................................................................................... 8<br />
5.1.4 HR ......................................................................................................................... 9<br />
5.1.5 Health Financing ................................................................................................. 10<br />
5.1.6 Service Delivery ................................................................................................. 10<br />
5.2 Community <strong>needs</strong> Assessment .................................................................................. 11<br />
6 Conclusions <strong>and</strong> Recommendations ................................................................................. 12<br />
7 Annexes ............................................................................................................................ 14<br />
7.1 Annex-I; Map of <strong>Hodeida</strong>h <strong>and</strong> Merlin’s Intervention districts ................................ 14<br />
7.2 Appendix-II; Catchment Areas <strong>and</strong> populations ........................................................ 15<br />
7.3 Health Facilities assessed ........................................................................................... 16<br />
7.4 Key Contacts, <strong>Hodeida</strong> .............................................................................................. 17<br />
7.5 Health Facility Assessment template ......................................................................... 19
1 Executive Summary<br />
Background: To scope out the feasibility <strong>and</strong> modalities of Merlin’s proposed<br />
nutrition/<strong>health</strong> intervention is <strong>Hodeida</strong>, a rapid field <strong>assessment</strong> was conducted by<br />
technical team comprising of Health Officer <strong>and</strong> Global supplies manager between 10 th <strong>and</strong><br />
22 nd of July 2012. The approach involved conducting KPIs (Key Person Interview) with MoPH<br />
<strong>and</strong> implementing agencies, visits to field sites (2 district hospitals <strong>and</strong> 10 Temporary <strong>health</strong><br />
facilities), observations, review of records <strong>and</strong> <strong>community</strong> FGDs (Focus Group Discussions).<br />
Key Findings: The findings suggest that there are huge <strong>needs</strong> in 3 sectors; Nutrition, <strong>health</strong><br />
<strong>and</strong> WASH. Acute malnutrition in children < 5yrs is high <strong>and</strong> in line with findings of recent<br />
Unicef survey (r<strong>and</strong>om unsystematic MUAC screening of 28 children found 6 MAM <strong>and</strong> 2<br />
SAM cases). Lack of hygiene practices <strong>and</strong> clean drinking water is one of the key issues. The<br />
epidemiological data <strong>and</strong> FGDs suggest that the key morbidities in <strong>community</strong> are Diarrhoea,<br />
ARI <strong>and</strong> Malaria, with higher relative incidence rates in the children 90%<br />
patients leave <strong>health</strong> facilities without drugs <strong>and</strong> there is acute shortage of essential<br />
equipment <strong>and</strong> WASH facilities. All these factors convert to poor utilization of services; OPD<br />
utilization rate of 0.2/person/year which is far below SPHERE st<strong>and</strong>ards of<br />
1consultation/person/year. This situation is worsened by weak HMIS, loose HR structure,<br />
inadequate supportive supervision, lack of continued medical education <strong>and</strong> corruption.<br />
Conclusions <strong>and</strong> recommendations: The <strong>needs</strong> in <strong>community</strong> justify Merlin’s approach of an<br />
integrated nutrition, <strong>health</strong> <strong>and</strong> WASH programme. It is feasible to set up stabilization<br />
centres at district level hospitals of Az Zaidiah <strong>and</strong> Al Marawah, however OTP sites need to<br />
be supported by Mobile Health <strong>and</strong> Nutrition teams, with <strong>community</strong> level outreach services<br />
2
through CHWs. MoPH is quite forthcoming to Merlin; working with them, building technical<br />
<strong>and</strong> infrastructural capacity complemented by <strong>community</strong> buy in <strong>and</strong> social mobilization will<br />
be imperative for successful programme implementation. Key programmatic challenges<br />
could be (but not limited to); recruitment <strong>and</strong> retention of quality staff especially at SCs,<br />
coordination with OTP level <strong>health</strong> workers <strong>and</strong> social mobilization. Strategically, it is<br />
extremely important that Merlin establishes presence on the ground at the earliest, initiates<br />
preparations office hire, staff recruitment, logistical etc <strong>and</strong> maintains relations with the key<br />
stakeholders.<br />
3
2 Context <strong>and</strong> Background<br />
The nutritional survey conducted by UNICEF <strong>and</strong> the Ministry of Health (MoPH) in late 2011<br />
showed that GAM (Global Acute Malnutrition) rates in children under 5 years of age in Al-<br />
<strong>Hodeida</strong> governorate were 31.7% which far exceeded the WHO emergency threshold of<br />
15%. Merlin initially (beginning of 2012) planned to implement an integrated CMAM <strong>and</strong><br />
essential primary <strong>health</strong> care programme in Hais <strong>and</strong> Al Khokha districts of Al <strong>Hodeida</strong>.<br />
However, Merlin managed to secure registration in Yemen only in May 2012. In discussion<br />
with UNICEF <strong>and</strong> Nutrition sub cluster, new geographical areas of nutrition programme<br />
intervention were agreed upon by the Merlin team comprising of Head of the region-Asia<br />
<strong>and</strong> head of Safety <strong>and</strong> Security Merlin HQ. The new areas of intervention include 35<br />
temporary <strong>health</strong> facilities (THF) in Al Marawah, AZ Zaidiah <strong>and</strong> Zabid districts of Al <strong>Hodeida</strong><br />
governorate, covering a catchment population of 151,731.<br />
At the same time initial discussions were finalized with UNICEF for a potential PCA<br />
(Programme Cooperation Agreement). The PCA would entail provision of nutritional<br />
supplementation to the children
Yemen between 10 th <strong>and</strong> 22 nd July 2012. Besides identifying additional funding<br />
opportunities, finalizing ongoing negotiations with UNICEF <strong>and</strong> WFP <strong>and</strong> establishing<br />
working relationships with government ministries, WASH <strong>and</strong> <strong>health</strong> clusters <strong>and</strong> donor<br />
agencies, the key objectives of the team were to:<br />
<br />
<br />
<br />
To conduct a thorough <strong>health</strong> <strong>facility</strong> <strong>assessment</strong> (OTP <strong>and</strong> SC sites) <strong>and</strong> critical<br />
<strong>health</strong> <strong>and</strong>/or nutrition <strong>needs</strong> in <strong>Hodeida</strong> governorate, Yemen.<br />
To explore the feasibility <strong>and</strong> identify possible bottlenecks for the proposed CMAM<br />
programme in <strong>Hodeida</strong><br />
To develop/revise <strong>and</strong> submit log frames, work plans <strong>and</strong> narrative reports for PCA<br />
with UNICEF <strong>and</strong> WFP, Yemen.<br />
4 Methodology for the <strong>assessment</strong><br />
The <strong>health</strong> <strong>facility</strong> <strong>assessment</strong> was conducted in due consultation with the MoPH Sana’a . A<br />
letter of consent <strong>and</strong> support was obtained from MoPH which was also faxed to <strong>Hodeida</strong><br />
HQ. With the help of Nutrition Sub Cluster <strong>and</strong> Merlin’s Consultant Dr Reyad, meetings were<br />
organized with the Director General <strong>and</strong> other senior officials of MoPH <strong>Hodeida</strong>. Objectives<br />
of the <strong>assessment</strong> were shared with the MoPH <strong>Hodeida</strong> <strong>and</strong> Dr Fawwaz from MoPH <strong>Hodeida</strong><br />
was assigned to the <strong>assessment</strong> team for providing essential operational <strong>and</strong> logistical<br />
support.<br />
The key approach for this <strong>assessment</strong> included field visits to the <strong>health</strong> facilities <strong>and</strong> villages,<br />
KPIs (Key persons Interviews) with MoPH, <strong>health</strong> <strong>facility</strong> staff <strong>and</strong> the <strong>community</strong><br />
leaders/tribesmen, Community FGDs (Focus Group Discussions), observation <strong>and</strong> review of<br />
available records/data.<br />
4.1 Sampling Frame <strong>and</strong> methods<br />
Out of 35, a total of 12 <strong>health</strong> facilities (34%) were selected for this <strong>assessment</strong>. The<br />
selection was non r<strong>and</strong>om <strong>and</strong> the decision was limited by the logistical challenges <strong>and</strong> time<br />
5
constraints. However every possible measure was taken to make the sample size as<br />
representative <strong>and</strong> as generalizable as possible. The key inclusion criteria’s that were<br />
considered while selecting the sampled HFs were; the catchment population (smallest <strong>and</strong><br />
the largest) <strong>and</strong> the distance from district HQ (closest <strong>and</strong> farthest). Finally 10 THFs <strong>and</strong> 2<br />
district level hospitals were assessed. Zabid hospital was visited but was not formally<br />
assessed as it had already been assessed by the WHO for establishment of Stabilization<br />
Centre.<br />
4.2 Tools for data collection:<br />
The <strong>health</strong> <strong>facility</strong> <strong>assessment</strong> data was collected using the template (See Annex.I)<br />
developed through adaptation of existing formats including Merlin tool, WHO’s HeRAMS<br />
tool, Save the children’s Health <strong>facility</strong> <strong>assessment</strong> tool. This was done keeping in mind the<br />
pragmatic situation <strong>and</strong> data <strong>needs</strong>. All the data was collected real-time through spot<br />
checks, review of records <strong>and</strong> KPIs. The data from all these forms was later manually entered<br />
into the Ms Excel matrix <strong>and</strong> analysed. The data was double checked for errors <strong>and</strong> outliers.<br />
Community <strong>needs</strong> <strong>assessment</strong> data was collected using <strong>community</strong> discussion record sheet,<br />
with structured questions. Supplementary responses from the participants of FGDs were<br />
collected in the additional space.<br />
5 Key Findings <strong>and</strong> Results:<br />
5.1 The Building blocks of Health Systems in <strong>Hodeida</strong>:<br />
5.1.1 Governance:<br />
The team at the MoPH level is very new lead by Dr Abdul Rahman Garallah the Director<br />
General of Health Services who joined the office only couple of months ago. He seemed to<br />
be extremely committed <strong>and</strong> forthcoming <strong>and</strong> assigned Dr Fawwaz, to accompany the<br />
<strong>assessment</strong> team. The MoPH <strong>Hodeida</strong> team is dedicated <strong>and</strong> wants to improve the current<br />
situation, but most of them have clinical backgrounds rather than public <strong>health</strong>. The MoPH<br />
<strong>Hodeida</strong> does receive instructions from Sana’a however they have sufficient authority for<br />
decision making at local level.<br />
6
5.1.1.1 Supportive Supervision:<br />
None of the assessed <strong>health</strong> <strong>facility</strong> was ever visited by a district or <strong>Hodeida</strong> level official<br />
during past 2 months <strong>and</strong> 62% of the HFs were visited more than one year ago. Most of the<br />
visits by the officials were during the mass polio vaccination campaigns or other <strong>health</strong><br />
camps. There seem to be no structured mechanism or framework for monitoring the field<br />
level activities.<br />
5.1.2 Drugs, Equipment <strong>and</strong> infrastructure:<br />
Drugs are supplied from Sana’a, <strong>and</strong> as per the DG <strong>health</strong>, the drug supply is quite irregular<br />
<strong>and</strong> only twice a year. Essential drugs in very limited quantity are supplied to <strong>Hodeida</strong> HQ<br />
<strong>and</strong> same goes down to the <strong>health</strong> facilities. There is acute shortage of drugs <strong>and</strong> nearly<br />
three fourth (72%) <strong>health</strong> facilities suggested that >90% of the patients are turned back<br />
without provision of prescribed drugs. An effective drug management system <strong>and</strong> cold chain<br />
was also found lacking; expired (dated) anti-malarial drugs, condoms <strong>and</strong> vaccine was found<br />
at the assessed <strong>health</strong> facilities. It however could not be ascertained whether these were<br />
distributed/administered to the beneficiaries.<br />
Nearly 62% of the <strong>health</strong> facilities had shortage of essential medical equipment (e.g<br />
thermometer, tongue depressor, weighing scale etc) for the services being provided. The<br />
overall upkeep/storage of drugs <strong>and</strong> equipment was poor (dusty, broken, unsterilized<br />
equipment, drugs stored at high temperatures). There were also instances when delivery kits<br />
supplied by Unicef/MoH few years ago remained packed <strong>and</strong> unused till date.<br />
Only 50% of <strong>health</strong> facilities assessed had any access to electricity. None of the <strong>health</strong><br />
facilities assessed had incinerators or safe waste disposal mechanisms. 3 of the 12 has<br />
running water, but without quality control or chlorination facilities, <strong>and</strong> only 1 offered<br />
drinking water for patients.<br />
District hospital buildings have patient waiting areas <strong>and</strong> an adequate number of rooms (10)<br />
for <strong>health</strong> services including OPD, FP, EPI, ANC, nutrition, delivery <strong>and</strong> laboratory. There are<br />
14 beds available for emergency use. However not all of the rooms or beds were being<br />
7
utilized, including a minor OT in Az Zaidiah. The condition of the buildings was reasonable<br />
but some of the areas needed major repairs e.g. big cracks in the wall of pharmacy, missing<br />
electricity fittings, <strong>and</strong> tiles falling off the walls in Az Zaidiah hospital. The electricity cuts are<br />
up to 14 hrs per day <strong>and</strong> both hospitals had working generators (100KV <strong>and</strong> 2KV). The waste<br />
disposal mechanisms were not being followed; syringes <strong>and</strong> needles were disposed off right<br />
in front of Az Zaidiah hospital. The toilets were available but very dirty. Running water was<br />
available from overhead tanks but was never chlorinated or tested for quality in the past one<br />
year. There were no drinking water facilities for the patients visiting the hospitals. Even the<br />
SAM children eating plumpy nut in the hospitals were not provided with drinking water as<br />
per CMAM protocols.<br />
Temporary <strong>health</strong> facilities 70% of assessed THFs were being run from 1-2 rooms in the<br />
house of <strong>health</strong> workers, 10% from a room in another government building (school) <strong>and</strong> 20%<br />
only existed on paper (as there was no space/room allocated to these facilities). None of the<br />
8 THFs in Al Marawah allocated to Merlin were functional on the ground. According to the<br />
District <strong>health</strong> manager of Al Marawah it is really hard to find rooms for THFs in these<br />
villages. As per him, the <strong>health</strong> workers are deployed for these THFs but only visit the areas<br />
for carrying out EPI activities. He had no answer when asked; ‘what do the <strong>health</strong> workers do<br />
on the other days’ 1 This feedback has been shared with DG <strong>health</strong> <strong>and</strong> he assured that all 8<br />
<strong>health</strong> facilities would be put in place before Merlin starts interventions’ in Al Marawah (it<br />
seems unlikely though <strong>and</strong> may need a follow up).<br />
There are no WASH (drinking water <strong>and</strong> toilets) facilities available at temporary <strong>health</strong><br />
facilities unless <strong>health</strong> workers let the beneficiaries use their own toilets. 50% of the HFs<br />
used personal gensets (probably out of the money earned through private consultations).<br />
5.1.3 HMIS<br />
There are specific reporting formats, registers <strong>and</strong> protocols for reporting of the <strong>health</strong><br />
information but the consistency <strong>and</strong> reliability of data is questionable. The <strong>assessment</strong> team<br />
1 The <strong>assessment</strong> team approached Sheikh of village Al-Shaibah who was very forthcoming (but had never been<br />
approached by MoH) <strong>and</strong> promised to provide a room <strong>and</strong> all possible help to set up the THF.<br />
8
got different information on different occasions regarding coverage of <strong>health</strong> services <strong>and</strong><br />
the epidemiological data, while reports did not match the data in registers on couple of<br />
occasions. No coverage charts except EPI were displayed in the <strong>health</strong> facilities but the<br />
presented EPI data was often ambiguous e.g. DPT-3 coverage > DPT-1 coverage. The <strong>health</strong><br />
management information system is mostly paper based <strong>and</strong> only computerised at MoPH<br />
<strong>Hodeida</strong> level for transmission to Sana’a. However, most importantly this data is not<br />
analysed or used for monitoring <strong>and</strong> appropriate corrective actions.<br />
5.1.4 HR<br />
The human resources for <strong>health</strong> in <strong>Hodeida</strong> varied in qualifications, technical skills <strong>and</strong><br />
contract agreements. The district level hospitals had reasonable number of <strong>health</strong> service<br />
providers (range 15 to 21); both hospitals had at least 1 doctor, 2 to 4 nurses <strong>and</strong> 6-9 midwives<br />
but no specialists. 90% 2 of the temporary <strong>health</strong> facilities had one <strong>health</strong> worker but<br />
their qualifications varied from nurse, nurse technician <strong>and</strong> <strong>health</strong> guide to doctor assistant.<br />
None of the facilities assessed had a specialist or MD on staff. Only one third of <strong>health</strong><br />
facilities had midwives available - though the district level facilities had several on staff, the<br />
majority of rural <strong>health</strong> facilities have no midwives available.<br />
The <strong>health</strong> staff in 75% of the THFs was officially employed by the MoPH however remaining<br />
25% THFs were being run by ‘Voluntary <strong>health</strong> workers’, who did not have any contract with<br />
MoPH but hoped to get it someday. These ‘voluntary’ <strong>health</strong> workers received some drugs<br />
(Amoxicillin <strong>and</strong> Anti malarial), vaccine, OCPs <strong>and</strong> RDTs for malaria from MoPH (district<br />
level). They maintained the <strong>health</strong> records on OPD, EPI, Malaria <strong>and</strong> family planning in MoPH<br />
supplied registers <strong>and</strong> submitted monthly reports to the District <strong>health</strong> office on prescribed<br />
formats. All of these voluntary <strong>health</strong> workers charged the beneficiaries for their services<br />
<strong>and</strong> personal drugs. As per them, they provided the Govt. supplied drugs free of charge<br />
(however this could not be verified).<br />
2 1 <strong>health</strong> <strong>facility</strong> in Zabid had 3 workers; 2 hired locally by the government <strong>health</strong> worker who had flourishing<br />
private practice<br />
9
The commitment <strong>and</strong> technical skills of the <strong>health</strong> officials <strong>and</strong> workers were inadequate.<br />
The salary of government staff is quite low; while a doctor receives approx. US$ 250 per<br />
month, a THF level <strong>health</strong> worker receives US$ 100-120. This is one of the key issues leading<br />
to poor motivation in the <strong>health</strong> workforce <strong>and</strong> an underlying reason for private practice (at<br />
least they say so). The level of skills in the <strong>health</strong> workers was low <strong>and</strong> there was a clear lack<br />
of continued medical education. Only 50% of the <strong>health</strong> workers received any training during<br />
past 1 year. The trainings received were on EPI <strong>and</strong> nutrition only.<br />
5.1.5 Health Financing<br />
The <strong>assessment</strong> team could not undertake major deliberations on this topic given the<br />
sensitivities around it. However <strong>health</strong> financing was immensely poor at central <strong>and</strong><br />
governorate levels. As per DG <strong>health</strong> they have to charge user fees in order to sustain the<br />
services at <strong>health</strong> facilities. On the other h<strong>and</strong> an expat doctor working in one of the<br />
assessed hospitals told that, ‘funds received by hospital don’t actually trickle down into the<br />
essential drugs <strong>and</strong> equipment’.<br />
5.1.6 Service Delivery<br />
Both the district level hospitals provided OPD, Family planning, ANC/PNC/delivery, nutrition<br />
(UNICEF supported OTP – screening <strong>and</strong> provision of plumpy-nut), EPI <strong>and</strong> lab services.<br />
However the services are only provided between 8 am to 1pm. All the services (including<br />
general OPD <strong>and</strong> lab tests) are paid <strong>and</strong> price lists are displayed at the entrance. Only Az<br />
Zaidiah hospital had a paediatric ward, which worked till 1pm <strong>and</strong> afterwards emergency<br />
patients were referred to <strong>Hodeida</strong>. Al Marawah had no paediatric ward but the district<br />
<strong>health</strong> manager’s office on 1 st floor had enough space to establish the stabilization centre 3 .<br />
All the catchment population of 100% assessed <strong>health</strong> facilities live within 2 hours walking<br />
distance from the <strong>health</strong> facilities. 87% 4 of the temporary <strong>health</strong> facilities provided OPD <strong>and</strong><br />
EPI services, 50% provided Family planning <strong>and</strong> 25% skilled birth attendance. However the<br />
3 Dr Reyad (Merlin Consultant) said he could arrange for necessary permissions to obtain the space<br />
4 All except Al Marawah THFs<br />
10
annual OPD utilization rates for the assessed <strong>health</strong> facilities were low; range 0.1-0.7 5 <strong>and</strong><br />
total 0.2 per person per year. This is far below the SPHERE st<strong>and</strong>ards of 1 consultation per<br />
person per year in a stable rural <strong>and</strong> dispersed population. According to the THF records, the<br />
SBA coverage for the catchment population was also quite low - 11%. The reported EPI<br />
coverage was 95% (range 64% - 340%) however this could not be verified in the field.<br />
The official working hours for all the <strong>health</strong> facilities are 8 am to 1pm. However 80% of the<br />
<strong>health</strong> workers (government employed or Voluntary) in functional THFs provided charged<br />
services beyond 1 pm; govt supplied drugs, (if any) were free. One of the THF worker had<br />
flourishing practice <strong>and</strong> he even locally hired a mid wife (@ $100 per month) to provide<br />
wider range of services including deliveries <strong>and</strong> lab facilities. Even senior MoPH staff<br />
engaged in post working hour’s private practice which is legal in Yemen.<br />
5.2 Community <strong>needs</strong> Assessment<br />
This was not one of the major components of <strong>assessment</strong> but information was gathered<br />
wherever feasible. The focus group discussions <strong>and</strong> KPIs suggested that there are huge<br />
nutrition (between 30 – 90% of families reported extreme food shortages), <strong>health</strong> <strong>and</strong> WASH<br />
<strong>needs</strong> in the <strong>community</strong>. There are acute food shortages as communities have less means to<br />
purchase the commodities. Women headed households are the most vulnerable, <strong>and</strong> 80%<br />
are reportedly unable to meet their daily food <strong>needs</strong>. In a r<strong>and</strong>om non-systematic MUAC<br />
screening (quick <strong>and</strong> dirty) of 28 children from different villages of the 3 districts, the<br />
<strong>assessment</strong> team found 2 SAM <strong>and</strong> 6 MAM cases. This gives a GAM rate of 28% which is<br />
similar to MoPH UNICEF Nutritional survey findings.<br />
The key <strong>health</strong> <strong>needs</strong> included prevention <strong>and</strong> treatment of diarrhoeal disease, acute<br />
respiratory infections <strong>and</strong> malaria. The children <strong>and</strong> women are most vulnerable to these<br />
diseases. Communities expressed a need for provision of Maternal <strong>and</strong> child <strong>health</strong> services<br />
closer to their villages, as well as midwives <strong>and</strong> skilled birth attendance in rural <strong>health</strong><br />
facilities.. The epidemiological data (2011) provided by MoPH suggest that the top 3<br />
5 Higher utilization rates in HFs with very low catchment population e.g Deer Ali HF in Az Zaidiah with<br />
catchment population of 1425 had utilization of 0.7 but Al Badwa with 10,625 had rate of 0.2 consultations per<br />
person /year<br />
11
morbidities in <strong>Hodeida</strong> include Respiratory infections (27.8%), Diarrhoea <strong>and</strong> Gastroenteritis<br />
(10.4%) <strong>and</strong> Malaria (9.1%). However children
drinking water <strong>and</strong> hygiene sanitation practices) which are further aggravated due to<br />
poverty, lack of awareness <strong>and</strong> <strong>health</strong> seeking behaviour, geographical distances <strong>and</strong><br />
user fees at point of service delivery.<br />
2. Health systems are weak in all of the 6 areas; Weak HMIS, acute shortage of drugs<br />
<strong>and</strong> equipment, poor infrastructure, loosely structured <strong>and</strong> technically weak <strong>health</strong><br />
workforce, inadequate range <strong>and</strong> coverage of essential <strong>health</strong> services are largely the<br />
result of weak governance, lack of commitment, corruption <strong>and</strong> inadequate <strong>health</strong><br />
financing.<br />
3. Merlin’s approach of an integrated nutrition, <strong>health</strong> <strong>and</strong> WASH programme is<br />
justified <strong>and</strong> <strong>needs</strong> based. If certain components are left unfunded, Merlin should<br />
seek additional opportunities<br />
4. MoPH officials at <strong>Hodeida</strong> level are quite forthcoming <strong>and</strong> have in principal agreed to<br />
provide all necessary support to Merlin’s programme. It will be imperative to work<br />
with/through them but also keep MoPH officials from Sana’a level in loop. It will be<br />
most productive to engage <strong>and</strong> build the capacity of staff at HF <strong>and</strong> <strong>community</strong><br />
levels.<br />
5. It is feasible to set up stabilization centres at district level hospitals of Az Zaidiah <strong>and</strong><br />
Al Marawah but will need lot additional logistical <strong>and</strong> operational efforts during start<br />
up / initial phase. Merlin will need to hire its own staff for SCs, <strong>and</strong> paediatric ward<br />
would need to be established in Al Marawah; 1 st floor in main building would be ideal<br />
6. OTP sites need to be supported by Mobile Health <strong>and</strong> Nutrition teams, with<br />
<strong>community</strong> level outreach services through CHWs. While a top up incentive (which is<br />
OK with MoPH) <strong>and</strong> capacity building of the THF workers will leverage support for<br />
MHNTs, the free distribution of essential drugs <strong>and</strong> equipment provided by Merlin<br />
will need to be monitored through setting up of Village <strong>health</strong> committees.<br />
7. Key programmatic challenges could be (but not limited to); recruitment <strong>and</strong><br />
retention of quality staff especially at SCs, minimizing corruption, coordination with<br />
OTP level <strong>health</strong> workers <strong>and</strong> social mobilization.<br />
8. Strategically, it is extremely important that Merlin establishes presence on the<br />
ground at the earliest (before end of Ramadan), <strong>and</strong> maintains relations with key<br />
stakeholders before more of areas allocated to Merlin are overtaken by other<br />
agencies (e.g Zabid SC taken over by WHO in July).<br />
13
7 Annexes<br />
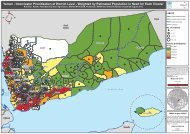
7.1 Annex-I; Map of <strong>Hodeida</strong>h <strong>and</strong> Merlin’s Intervention districts<br />
Figure 2: Map of Al <strong>Hodeida</strong>h, Yemen showing 3 districts of Intervention (Source Nutrition Cluster Yemen, 2012)<br />
14
7.2 Appendix-II; Catchment Areas <strong>and</strong> populations
7.3 Health Facilities assessed<br />
S.<br />
No.<br />
District Facility Distance from<br />
HQ (hrs by<br />
Car)<br />
Distance<br />
from Dist.<br />
HQ (hr.min)<br />
Key Informants Designation Phone<br />
1 Az Zaidiah Az Zaidiah hospital 0.50 0.00 Dr Abdul Wahab M.O Medical officer<br />
__________<br />
Mohd. A Gilan Matron<br />
737126179<br />
2 Az Zaidiah Al Rabat THF 1.10 0.20 Yahya Ali Health worker 733526585<br />
3 Az Zaidiah Deer Al Wagih THF 1.30 0.40 Issa Hadi Haggagi Volunteer (Diploma 736575002<br />
Nursing)<br />
4 Az Zaidiah Burkhul THF 2.00 1.00 Yusuf Abdullah Yusuf Volunteer (Doctor<br />
711891366<br />
Assistant)<br />
5 Az Zaidiah Deer Ali THF 1.00 0.10 Kasim Abdullah Ali Volunteer (Nurse Male) 770101764<br />
6 Zabid Al-Badwa THF 1.00 0.10 Futeini Yahya<br />
Saida Abdulla Siddique<br />
Health worker<br />
Hired volunteer<br />
777350276<br />
736218819<br />
7 Zabid AL Tawelah THF 2.00 0.45 Nasher Hussein Mahi Health Worker 733524133<br />
Daoud Ismail Ali<br />
8 Zabid Al Habeel THF 2.00 0.50 Abid Abdullah Nurse 734021321<br />
9 Zabid Al Fadel THF 1.45 0.35 Samira hamid Health Worker 735757361<br />
10 Al Marawah Al Marawah<br />
Health Centre<br />
0.25 0.00 Ahmed Shaibah<br />
Abdul Qayei<br />
11 Al Marawah Mahal Omer THF 1.00 0.30 Ahmed Shaibah<br />
Abdul Qayei<br />
12 Al Marawah Al Shaibah THF 1.10 0.45 Ahmed Shaibah<br />
Abdul Qayei<br />
District Health Manager,<br />
Manager Health Centre<br />
District Health Manager,<br />
Manager Health Centre<br />
District Health Manager,<br />
Manager Health Centre<br />
777311633<br />
771129489<br />
777311633<br />
771129489<br />
777311633<br />
771129489<br />
16
7.4 Key Contacts, <strong>Hodeida</strong><br />
Agency/Organization Name Position E:mail Tel #<br />
Government<br />
<strong>Hodeida</strong> Governorate<br />
Local Council<br />
Governor’s Office<br />
Chairman<br />
Health office Aabdulrahman Garallah DG of Health office Gar_psych@yahoo.com 777202996<br />
Health office Dr. Ahmed Zabarah Deputy DG <strong>health</strong> 771341766<br />
Dr Fawaz Al Kajlani Health Care Service dr.fawaz777@gmail.com 777383426<br />
Dr Abdulwahab Al Faquih Assistant manager 7772245672<br />
Dr Yassir Shahar<br />
International Cooperation<br />
777245100<br />
manager<br />
Dr Ali Shuaib PHC Manager alishuiab2008@yahoo.com 777269060<br />
Yahya Gunaid Health Education 777176230<br />
Local NGOs<br />
Abo mosa NGO Mr. Abdoh Ali Mnsoob DG Abo mosa NGO Alashary5@gmail.com 777715690<br />
CSSW Mr.Faisal Al-ghushaimi Coordinator falghoshaimi@gmail.com 777215126,712045807<br />
WES group Mrs. Fatima Jelan Manager wesgroup_w@hotmail.com 733886029<br />
WES group Mr. Hatem Musleh Executive Director wesgroup_w@hotmail.com 777189462,733314284<br />
Me for my country Ms.Shawqeah Al-absi General manager Mem.hod@gmail.com 733570210<br />
Future NGO Dr. Mohamed Taleb General manager moust360@yahoo.com 777310092<br />
Future NGO Mr. Abdoh Yassen moust360@yahoo.com 733574754<br />
YFCA Mrs .Asia Shaibani 733870655<br />
YFCA Ms.Takia Ali Fakirah 771571166,73520608<br />
YWU Mariam Omar Al-haj WYU_hod@yahoo.com<br />
777743971<br />
khammash26@yahoo.com<br />
YWU Amat Al-rahman Ahmed amtalrhman2009@gmail.com 777544511<br />
ROPHD Abdoh Mohamed al-khewani Coordinator Abdua43@gmail.com 700696946,773047465<br />
17
International NGOs<br />
OXFAM Tinka Lydia Project manager LTinka@oxfam.org.uk 735177753<br />
OXFAM Apollo Arora Emergency food sec.& aarora@oxfam.org.uk 734982777<br />
livelihood coordinator<br />
OXFAM Ms. Eva Niederberger HSP PHP ENiederberger@oxfam.org.uk 736801054<br />
Save the Children Dr Mariam 711103331<br />
Save the Children Ms. Alem Greiling Nutrition specialist AGreiling@mena.savethechildren.se 735201534<br />
Save the Children Dr.Shihab Ibrahim Programme Officer sibraheem@mena.savethechildren.se 736444928<br />
Islamic relief Mr.Hashem Awnallah Country Director hashem.awnallah@iryemen.org 772388880<br />
Global sports partners Mr. Kevin Graham General manager GSPYEMEN@pobox.com<br />
733118176<br />
kevinbgraham@pobox.com<br />
GIZ-SFS Mr. Parta Advisor sfsyemen@yahoo.com 777187450<br />
SOUL Ms Nadden Noor Al-hebshi Team leader n_noor@soul-yemen.org 711138383<br />
IRD Dr.Sue Ellis Country Director sellis@irdglobal.org 736845226<br />
IRD Mr.Hunter Price Program Officer hprice@ird-dc.org 733137615<br />
IRD Mr. Basam Al-absi Consultant alabsibassam@gmail.com 735400500<br />
Vision hope Ms.Ypie de Wolf Project Director Disaster ypie.dewolf@vision-hope.org 733199474<br />
Response<br />
Vision hope Mr. Matthias Leibbr<strong>and</strong> Chief Executive Officer matthias.leibbr<strong>and</strong>@vision-hope.org 733712036<br />
United Nations Organisations<br />
WFP Ms.Ami Nagamune Program officer ami.nagamune@wfp.org 736777834<br />
WFP Ms. Amani Al –Manakhi Programme assistant Amani.AlManakhi@wfp.org 736777827<br />
UNICEF Dr. Rasha Al-ardi Health <strong>and</strong> Nutrition Officer ralardi@unicef.org 712223014<br />
UNICEF Salaam Education/WASH 712223494<br />
UNICEF Dr. Khaled Al-shaibani Field officer <strong>Hodeida</strong>h kalshaibani@unicef.org 711684553<br />
UNOCHA Abdirahman Mohamed Humanitarian Affairs Officer Mohamed142@un.org 712222817<br />
UNDSS El Saeed Karara Field Security Coordinator elsaid.karara@undss.org 712222466<br />
18
7.5 Health Facility Assessment template<br />
Health Facility Assessment Form<br />
QES No.: ______ Date: ______/________/______ Governorate: _____________________<br />
District: _______________ Village Name: ___________________ Coord.: X ________Y ________<br />
Distance from State HQ (by car): ___ hr_____min<br />
Distance from District HQ (by hour/car): ___hr_____min<br />
Name of Interviewer: ________________________<br />
Name, Designation <strong>and</strong> Contact no of Key Informant:______________________________________________<br />
*****************************************************************************************<br />
GENERAL INFORMATION<br />
1. Estimated Population of the catchment area served by this HF:<br />
Total Population ______ or HH _______ No. of villages:_________<br />
2. Type of Health Facilities: Health Center (Bedded) ____ (# beds) PHC Unit <br />
Health Center (No bed) Dispensary <br />
Dressing Others: ________<br />
3. Which is/are the organization/s supporting this Health Facility: ____________________________<br />
______________________________________________________________________________________<br />
4. Was the building constructed by: MOH when ________________<br />
NGO _______when ________________<br />
Other _______when ________________<br />
(specify the type of construction, e.g. brick, tent, etc.) ________________________________________<br />
5. How many rooms <strong>and</strong> for which services they are available<br />
Room Diameter Doors Windows paint Comment on equipments absent Other<br />
comments
Plan of the Health <strong>facility</strong> (with the actual distribution of the services)<br />
6. Electricity Connection Available: Yes No Average duration of load shedding/Day: _______hrs<br />
Alternative source of electricity: Genset Solar Inverter Other_____________ None<br />
7. Is there a functional incinerator available Yes No <br />
Are there adequate mechanisms for safe disposal of Medical Waste Yes No <br />
8. Is water available at this HF Yes No IF NOT, SKIP TO No. 8<br />
If yes, is there a network system Yes No <br />
If not, where is the water from:<br />
Town network system<br />
Protected well<br />
Unprotected well<br />
Other source<br />
<br />
<br />
<br />
_____________________________<br />
If not from a network system, where is the water stored: ________________________<br />
Is the water chlorinated <strong>and</strong> tested for residual chlorine Chlorinated Y/N<br />
Tested Y/N<br />
9. Are latrines available Yes No <br />
If yes, how many: ___________<strong>and</strong> in which condition: good fair bad <br />
Separate for Males <strong>and</strong> Females Yes No <br />
10. Is this Health Facility serving: IDP only IDP & Residents Residents only <br />
HEALTH SERVICE AND MANPOWER<br />
11. No. of Health Staff present at the HF:<br />
Staff<br />
Doctor<br />
Doctor<br />
Pharmaci<br />
Nurse<br />
Laboratory<br />
Nutrition<br />
Watsan<br />
Mid<br />
Health<br />
CHW<br />
Other<br />
Specialist<br />
General<br />
st<br />
Technician<br />
Staff<br />
Officer<br />
Wife<br />
visitor<br />
National<br />
International<br />
20
12. Health Facilities type of services provided:<br />
Type of services<br />
OPD<br />
Availability<br />
Y / N<br />
Any comments on functionality,<br />
Numbers/coverage for past month<br />
IPD Beds<br />
Male<br />
Female<br />
SMALL THEATRE<br />
PHARMACY<br />
LABORATORY<br />
(Essential<br />
Drugs)<br />
ANC<br />
PNC/FP<br />
EOC/Delivery<br />
>5 Child HC<br />
SFC<br />
TFC<br />
NUTRITION<br />
CTC<br />
VIT. A<br />
GMP<br />
EPI/cold chain<br />
ORT<br />
OTHER (specify)<br />
13. Is an OPD SERVICE provided Yes No If Yes, Please fill the following table:<br />
No. Description Available Qty Functioning Not Functioning Remarks<br />
1 Stethoscope<br />
2 Sphygmomanometer<br />
3 Thermometer<br />
4 Torch<br />
5 Tongue Depressor<br />
6 Foetoscope<br />
7 Paracheck<br />
8 Table<br />
9 Chair<br />
14. Is an IPD SERVICE provided Yes No If Yes, Please fill the following table:<br />
21
No. Description Available Qty<br />
1 Bed (male)<br />
2 Bed (female)<br />
3 Drip Holder<br />
4 Safety Box<br />
15. Is a LABORATORY SERVICE provided Yes No If Yes, Please fill the following table:<br />
No. Description Available Qty Functioning Not Functioning Remarks<br />
1 Microscope<br />
2 Manual centrifuge<br />
3 Slides<br />
4 Reagent Gemsa Stain<br />
5 Safety box<br />
16. Are CHILD HEALTH/NUTRITION SERVICES provided Yes No If Yes, Please fill the following<br />
table:<br />
No. Description Available Qty Functioning Not Functioning Remarks<br />
1 Weighing/height Scales<br />
2 Oxygen Concentrator<br />
3 Timer<br />
4 Thermometer<br />
5 Nebulizer<br />
6 GM card<br />
7 Vaccination card<br />
16a. Is there adequate <strong>and</strong> appropriate space for storage of Nutrition commodities Yes No <br />
17. Is a REPRODUCTIVE HEALTH SERVICE provided Yes No If Yes, Please fill the following table:<br />
No. Description Available Qty Functioning Not Functioning Remarks<br />
1 Stethoscope<br />
2 Sphygmomanometer<br />
3 Thermometer<br />
4 Weighing Scale<br />
5 Foetoscope<br />
6 Antenatal Care Card<br />
7 Poster on FP<br />
8 Poster on FP, HIV/AIDS/STI<br />
9 Poster on Obstetric Risk Factors<br />
10 Anaemia Management Guide<br />
11 Table<br />
12 Chair<br />
18. Are Contraceptive available Yes No <br />
If yes, can you list which methods:<br />
__________________________________<br />
__________________________________<br />
__________________________________<br />
19. Is a DELIVERY SERVICE provided Yes No If Yes, Please fill the following table:<br />
22
No. Description Available Qty<br />
1 Delivery kit<br />
2 Bed<br />
3 Drip Holder<br />
4 Safety Box<br />
20. Is an ORT CORNER available Yes No If Yes, Please fill the following table:<br />
No. Description Available Qty Remarks<br />
1 Aluminium Jug<br />
2 Cups & Spoon<br />
3 Nasogastric Tube<br />
4 Explanation Table<br />
5 Chair<br />
6 ORT Poster<br />
21. Is EPI SERVICE provided Yes No If NO, Skip the following questions<br />
22. Do you know about VACCINATION TARGET <strong>and</strong> STRATEGY<br />
No DESCRIPTION TARGET % WHEN WHERE # of Children<br />
Vaccinated*<br />
1 Fix Centre<br />
2 Outreach<br />
3 Mobile Team<br />
23. Please fill the following table:<br />
(*refer to previous month: _____________)<br />
No. Description Available Qty Functioning Not Functioning Remarks<br />
1 Solar Vaccine Refrigerator<br />
2 Vaccine Carrier<br />
3 Cold Chain Monitoring<br />
4 Vaccine Vial Monitoring<br />
5 Vaccination Card<br />
6 Vaccination register<br />
7 Safety Box<br />
8 Table<br />
9 Chair<br />
VACCINES:<br />
10 - BCG Available Qty Vaccine Stock Outs (in Past 3 months) Period (From to)<br />
11 - PENTA<br />
12 - OPV<br />
13 - MEASLES<br />
14 - TT<br />
23