EMPHYSEMATOUS PYELONEPHRITIS - Health Sciences
EMPHYSEMATOUS PYELONEPHRITIS - Health Sciences
EMPHYSEMATOUS PYELONEPHRITIS - Health Sciences

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Pictorial Commentary Emphysematous Pyelonephritis<br />
PICTORIAL COMMENTARY<br />
<strong>EMPHYSEMATOUS</strong> <strong>PYELONEPHRITIS</strong><br />
Contributed by C Anand MD and RP Swaminathan, MD<br />
Department of Medicine, Jawaharlal Institute of Postgraduate Medical Education and Research<br />
(JIPMER), Dhanvantari Nagar PO, Pondicherry – 605006<br />
Address for correspondence: RP Swaminathan, Professor of Medicine, Department of Medicine, JIPMER,<br />
Dhanvantari Nagar PO, Pondicherry – 605006.<br />
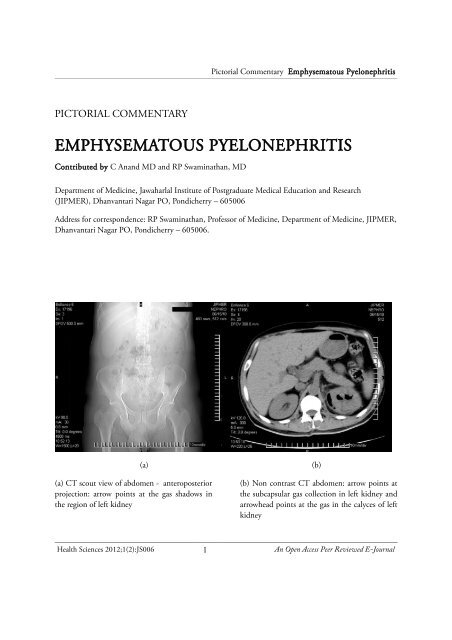
(a) (b)<br />
(a) CT scout view of abdomen - anteroposterior<br />
projection: arrow points at the gas shadows in<br />
the region of left kidney<br />
(b) Non contrast CT abdomen: arrow points at<br />
the subcapsular gas collection in left kidney and<br />
arrowhead points at the gas in the calyces of left<br />
kidney<br />
<strong>Health</strong> <strong>Sciences</strong> 2012;1(2):JS006 1 An Open Access Peer Reviewed E-Journal
Pictorial Commentary Emphysematous Pyelonephritis<br />
A 40yr old male patient, a known patient with<br />
type 2 diabetes and poorly controlled blood<br />
glucose levels presented with intermittent high<br />
grade fever, left sided flank pain, loss of appetite,<br />
decreased urine output and edema of one week<br />
duration. He had dysuria and hematuria as well.<br />
He was a diabetic for 3 years, was on oral<br />
hypoglycemics and had undergone operation for<br />
diabetic foot in the past. He had no history of<br />
either renal stone disease or tuberculosis in the<br />
past.<br />
Examination revealed pallor, bilateral pitting<br />
pedal edema and left renal angle tenderness. He<br />
was hemodynamically stable. Cardiovascular,<br />
respiratory and central nervous systems were<br />
normal on examination. His blood glucose at<br />
presentation was 320mg/dL; he had no evidence<br />
of diabetic ketoacidosis.<br />
A diagnosis of left side pyelonephritis was<br />
suspected and an ultrasound of kidneys, ureter<br />
and bladder (KUB) was done, which revealed<br />
gas in the left kidney and pelvis. The diagnosis<br />
of emphysematous pyelonephritis was<br />
considered and a non contrast CT of KUB was<br />
performed for confirmation of diagnosis and<br />
staging of the disease. CT of KUB revealed gas<br />
in the subcapsular space, parenchyma and the<br />
collecting system of left kidney. The diagnosis<br />
was – class IIIa emphysematous pyelonephritis<br />
of the left Kidney. Right kidney was normal.<br />
There was no evidence of any urinary calculi or<br />
obstruction.<br />
He was treated with intravenous antibiotics –<br />
ceftriaxone and ciprofloxacin empirically along<br />
with insulin. Antibiotics were changed to<br />
meropenam and amikacin based on urine<br />
culture which grew E.Coli. Patient became<br />
afebrile within 48 hrs of initiation of<br />
meropenam and amikacin. Patient improved<br />
symptomatically and required no surgical<br />
intervention. Renal function did not recover<br />
completely. This was attributed to the presence<br />
of underlying diabetic nephropathy. Patient was<br />
discharged in euglycemic state with stable renal<br />
functions after 4 weeks of antibiotic course,<br />
which included 2 weeks of<br />
Amikacin/Meropenam.<br />
CLINICAL PEARLS<br />
The above case provides several insights to a<br />
potentially life threatening infection –<br />
emphysematous pyelonephritis<br />
• Diabetes predisposes patients to severe<br />
infections of the urinary tract. The<br />
upper urinary tract may be involved in<br />
up to 80% of the patients. 1<br />
• Emphysematous pyelonephritis (EPN)<br />
can occur in insulin dependent and<br />
non- insulin dependent patients even in<br />
the absence of ureteric obstruction.<br />
• EPN may present with vague clinical<br />
symptoms such as fever, abdominal<br />
pain, nausea and vomiting with sudden<br />
clinical deterioration.<br />
• Renal angle tenderness is the most<br />
common clinical finding and pyuria is<br />
present in almost all cases. 2<br />
• Most patients with EPN have a<br />
deranged renal function at<br />
presentation. 3, 4<br />
<strong>Health</strong> <strong>Sciences</strong> 2012;1(2):JS006 2 An Open Access Peer Reviewed E-Journal
Pictorial Commentary Emphysematous Pyelonephritis<br />
• CT KUB is the definitive investigation<br />
for establishing the diagnosis.<br />
The commonly followed classification of EPN<br />
based on CT was given by Huang and Tseng. 2<br />
resuscitation, antibiotics and control of<br />
blood sugars.<br />
• Obstruction of the urinary tract has<br />
been reported in 29% of the individuals<br />
with emphysematous pyelonephritis. 6<br />
CLASS<br />
I<br />
CT FINDING<br />
Gas in collecting system only<br />
• Percutaneous nephrostomy or ureteric<br />
stent may be needed in a patient with<br />
ureteric obstruction.<br />
II Parenchymal gas only<br />
IIIa Extension of gas into<br />
perinephric space<br />
IIIb<br />
IV<br />
Extension of gas into pararenal<br />
space<br />
EPN in solitary kidney, or<br />
bilateral disease<br />
The classification serves as a useful guide for<br />
therapy and prognosis.<br />
• Nephrectomy is reserved for patients<br />
who are unresponsive to medical<br />
treatment, and fulfill one or more of the<br />
following criteria: possession of a<br />
nonfunctioning kidney, presentation of<br />
gross renal parenchymal destruction,<br />
display of a class IIIa or IIIb gas pattern,<br />
and existence of two or more risk<br />
factors.<br />
• Thrombocytopenia, acute renal failure,<br />
disturbance of consciousness and shock<br />
are factors which predict a poor<br />
outcome 2 . Other factors are bilateral<br />
emphysematous pyelonephritis and<br />
renal parenchymal necrosis on imaging<br />
with either no fluid content or a<br />
streaky/mottled gas pattern.<br />
• Commonest urinary pathogen causing<br />
EPN are E.coli and Klebsiella<br />
pneumonia. 4, 5<br />
• Initial management of EPN involves a<br />
three pronged approach with involves<br />
Management algorithm for a patient<br />
presenting with EPN is given below: 7<br />
DIABETIC PATIENT WITH FEVER,<br />
RENAL ANGLE PAIN AND PYURIA<br />
ANTIBIOTICS<br />
<strong>Health</strong> <strong>Sciences</strong> 2012;1(2):JS006 3 An Open Access Peer Reviewed E-Journal
Pictorial Commentary Emphysematous Pyelonephritis<br />
PCN OR STENT<br />
HYDRONEPHROSIS<br />
KUB XRAY*<br />
STONE<br />
NORMAL<br />
USG KUB<br />
PCD OR STENT<br />
GAS<br />
GAS<br />
CT<br />
NEPHRECTOMY OR PCD<br />
CHRONIC RENAL FAILURE<br />
PARENCHYMAL GAS<br />
NORMAL RENAL FUNCTION; HUANG<br />
AND TSENG CLASS III, FIT<br />
NEPHRECTOMY<br />
SPECIAL GROUPS<br />
PCD +/- NEPHRECTOMY<br />
BILATERAL DISEASE<br />
PCD<br />
PCD +/- NEPHRECTOMY<br />
SOLITARY KIDNEY<br />
FAILURE TO RESPOND<br />
Abbreviations: PCD, percutaneous drainage;<br />
PCN, percutaneous nephrostomy. Asterisks<br />
denote alternatives for where CT is not readily<br />
available.<br />
References<br />
1. Forland M, Thomas V, Shelokov A.<br />
Urinary tract infections in patients with<br />
diabetes mellitus: studies on antibody<br />
coating of bacteria. JAMA1977;<br />
238:1924-6.<br />
2. Huang JJ and Tseng CC.<br />
Emphysematous pyelonephritis:<br />
Clinicoradiological classification,<br />
management, prognosis and<br />
pathogenesis. Arch Intern Med<br />
2000;160:797-805.<br />
3. Michaeli J, Mogle P, Perlberg S,<br />
Herman S and Caine M.<br />
Emphysematous pyelonephritis. J Urol<br />
1984; 131, 205–207.<br />
4. Shokeir AA, eL-Azab M, Mohsen T and<br />
el Diosly T. Emphysematous<br />
pyelonephritis. A 15 year experience<br />
with 20 cases. Urology 1997;49:343–<br />
346.<br />
5. Chen MT, et al. Percutaneous drainage<br />
in the treatment of emphysematous<br />
pyelonephritis : a 10 year experience. J<br />
Urol 1997; 157:1569–1573.<br />
6. Stein JP, et al. Bilateral emphysematous<br />
pyelonephritis: a case report and review<br />
of the literature. Urology 1996;47:129–<br />
134.<br />
7. Pontin AR and Barnes RD. Current<br />
management of emphysematous<br />
pyelonephritis. Nat Rev Urol 2009;<br />
<strong>Health</strong> <strong>Sciences</strong> 2012;1(2):JS006 4 An Open Access Peer Reviewed E-Journal
Pictorial Commentary Emphysematous Pyelonephritis<br />
6:272-279.<br />
<strong>Health</strong> <strong>Sciences</strong> 2012;1(2):JS006 5 An Open Access Peer Reviewed E-Journal