A MESSAGE FROM THE EXECUTIVE DIRECTOR Nancy Chobin ...
A MESSAGE FROM THE EXECUTIVE DIRECTOR Nancy Chobin ...
A MESSAGE FROM THE EXECUTIVE DIRECTOR Nancy Chobin ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
CRITERION<br />
JA NUA RY 2004 “The Off icial Newsletter of the CBSPD, Inc.” VOLUME 9, I SSUE 1<br />
A <strong>MESSAGE</strong> <strong>FROM</strong> <strong>THE</strong> <strong>EXECUTIVE</strong> <strong>DIRECTOR</strong><br />
<strong>Nancy</strong> <strong>Chobin</strong>, RN, CSPDM<br />
Congratulations to all the new Certified personnel, including the 423 members who received reciprocal certification<br />
from the New Jersey Healthcare Central Service Association, California Central Service Association, Department<br />
of Veterans Affairs, IAHCSMM and Houston, TX area. We welcome you to the CBSPD.▲<br />
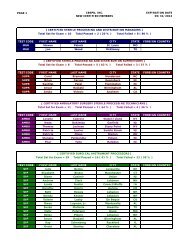
During 2003, the CBSPD offered its first certification<br />
examination in Mexico City. Forty<br />
four candidates sat for the exam and 82%<br />
passed. The certification process is being<br />
sponsored by 3M Mexico. In July, a ceremony<br />
was held to recognize the 39 students who<br />
successfully completed the Central Service<br />
training course. Physicians, nurses and 3M<br />
executives were present. It was a joyful day<br />
and I was honored to be present to witness<br />
this event.<br />
A second group sat for the October exam. In<br />
The 39 students who completed the CS training course sponsored by 3M Mexico<br />
2004, the CBSPD will assist Bogota, Colombia<br />
to start certification. Initial talks were held with representatives from Japan at the ASHCSP Annual Meeting in<br />
Grand Rapids, MI. ▲<br />
The CBSPD Board met in New Jersey in December (during a<br />
blizzard). The Board members bravely traveled to New Jersey<br />
and weathered the storm. Congratulations to all the Board<br />
Members! The CBSPD said goodbye to Pat Barnett who was<br />
the Manager representative. She was presented with a Plaque<br />
of Appreciation for her service. She will continue to write for<br />
the Criterion Newsletter. The Board welcomed newly elected<br />
members Karen Santos of Connecticut (Manager representative),<br />
Barbara Aldeman of Iowa (Department of Veterans’ Affairs<br />
representative), Lori Stratton of Vermont (Surgical Instrument<br />
Technician Representative) and Lanfrey Funches of<br />
Georgia (Technician Representative). The Board Members<br />
were taken on a site visit to the Chauncey Group International’s<br />
headquarters in Princeton and met with the Chauncey<br />
staff. The CBSPD Board was impressed with the services<br />
provided by the Chauncey Group and felt the trip was very<br />
worthwhile.<br />
Congratulations to Pat Barnett (left) (previous Manager representative)<br />
who was presented with a plaque for her service<br />
to the CBSPD, by <strong>Nancy</strong> Cho bin (ri ght)<br />
Continued on Next Page<br />
AAMI Update: Pg. 2 Ask Pat!: Page 6<br />
What’s Inside… Board Member Thoughts: Pg. 3 Inservice: Supply Distribution Systems: Pg. 6<br />
Continuing Ed. Report: Pg. 5
Message from <strong>Nancy</strong> <strong>Chobin</strong> Cont.<br />
In New Jersey, we continue to wait for the mandatory certification to take effect. The CBSPD is going to concentrate<br />
on bringing to focus the importance of the Sterile Processing Profession and to continue to push for<br />
mandatory certification nationwide with realistic salaries for this very important job. The Board believes that<br />
the only way we will get respect for our profession is to do it ourselves. We need to actively promote sterile<br />
processing as a worthy profession. After all, what facility can function without us? ▲<br />
I would like to encourage you to submit articles or notices to this Newsletter. It is your Newsletter. We would<br />
love to hear from you about what is going on at your facility. E-mail the information to us at: CBSPD@att.net.<br />
The deadline for the next Newsletter is June 1, 2004. ▲<br />
On behalf of the Board of Directors I wish all you Happy Holidays and a Healthy and Happy 2004!<br />
AAMI UPDATE (Association for the Advancement of Medical<br />
Instrumentation)<br />
• ST-46 (Steam Sterility and Sterility Assurance for Health Care Facilities) document has been updated and is<br />
available. This is an excellent document and should be the “Bible” for all processes in SPD.<br />
• TIR-12 – This is a new document in which manufacturers will be given guidance as to what information<br />
we (end users) need to process their reusable items. <strong>Nancy</strong> <strong>Chobin</strong> serves as Co-Chair of this Committee.<br />
• Rigid Container and Organizing Case Document - this document currently under development – will give<br />
guidance to manufacturers of rigid containers and organizing cases as to how to manufacture them (e.g.<br />
type of handles), weight, material of construction, cleaning and sterilization instructions, etc. A special<br />
meeting is scheduled for January 14, 2004 to continue work on this important document. Look for major<br />
changes in instructions in processing devices in containers and/or organizing cases as a result of this<br />
document.<br />
• Chemical Sterilants – this document is being updated and revised. A special water quality addendum will<br />
be included. The water quality will include standards for water used for cleaning, rinsing, etc. This document<br />
will impact on most facilities.<br />
• ST-79 – AAMI is coordinating all the steam documents into one large compendium called ST-79. It will<br />
include ST-46, ST35 (Decontamination), ST-33 (Flash Sterilization) and ST-37 (Rigid Containers). This is a major<br />
task and the work is continuing. Once this document is available, the other documents will be phased<br />
out (as individual purchases).<br />
For more information on AAMI publications, visit their web site at: www.aami.org. If your hospital or a<br />
member of your BioMedical Department is a member of AAMI you can purchase their publications at a discount.<br />
▲<br />
In Memoriam—The CBSPD sadly announces the passing of Arleen Capati, CSPDT, a long time<br />
member. Arleen lived and worked in New Jersey and held several positions in SPD; the last being SPD Manager<br />
at Monmouth Medical Center, Long Branch, NJ. Arleen will be remembered for her wonderful sense of<br />
humor and extensive knowledge of surgical instrumentation. She will be deeply missed. ▲<br />
THANK YOU NEW JERSEY HEALTHCARE CENTRAL SERVICE ASSOCIATION. The CBSPD announced<br />
a donation of $5,000 from the New Jersey Healthcare Central Service Association. The group has<br />
been a long time supporter of certification with contributions over the years totaling over $50,000! The funds<br />
will be used to support new credentials being considered. The Board greatly appreciates the continued support<br />
of the NJHCSA. ▲<br />
Continued on Next Page<br />
January 2004 Criterion - Page 2
NOCA Meeting—<strong>Nancy</strong> <strong>Chobin</strong> and Past<br />
Board Member Peggy Ryan attended the Annual National<br />
Organization for Competency Assurance meeting<br />
in Orlando in November. The focus of this meeting<br />
was on security and re-certification criteria. The<br />
CBSPD Board is looking to make some changes in<br />
both areas. ▲<br />
<strong>THE</strong> CBSPD <strong>EXECUTIVE</strong><br />
COMMISSIONERS<br />
(NON-VOTING)<br />
<strong>Nancy</strong> <strong>Chobin</strong>, RN, CSPDT, CSIT, CSPDS, CSPDM,<br />
Executive Director<br />
Teckla Ann Maresca, LPN, CSPDT, CSIT, CSPDS,<br />
CSPDM, Executive Commissioner, Chair CEU Committee<br />
Sue McManus, RN, CEH, CSPDT, CSIT, CSPDS, CSPDM, Executive Commissioner, Board Liaison,<br />
Chairperson Item Writing & Item Review Committee<br />
Nora Wikander, RN, CSPDT, CSIT, CSPDS, CSPDM, Executive Commissioner, Co-Chair CEU Committee<br />
M. Eleanor Reilly, B.S.N., CSPDT, CSIT, CSPDS, CSPDM, Board Member Emeritus<br />
Bobby Osburn, CSPDM, Dept of Veteran’s Affairs Representative<br />
Martha Young, CSPDT, International Liaison Representative<br />
CBSPD VOTING BOARD<br />
Karen Santos, LPN, CSPDM, Manager Representative<br />
Barbara Leigh, CSPDS, Supervisor Representative<br />
Lanfrey Funches, CSPDT, Technician Representative<br />
Lori Stratton, CSIT, CSPDT, Surgical Instrument Technician Representative<br />
Barbara Aldeman, Veteran’s Affairs Representative<br />
Paul Letersky, B.A., J.D., Public Member<br />
<strong>Nancy</strong> <strong>Chobin</strong> (left); Peggy Ryan (center) ; Sue McManus (right) attending<br />
the ASHCSP meeting in Grand Rapi ds, MI.<br />
Some Thoughts From Our New Board Members<br />
Lanfrey Funches—CSPDT, Technician Representative: My name is Lanfrey Funches and I hold the Certified<br />
Technician position on the CBSPD Board of Directors. I would like to say thanks to everyone that voted for<br />
me. For those that don’t know me, I have been working in Sterile Processing for 10 years. At the present time<br />
I’m the second shift Lead Tech at Athens Regional Medical Center in Athens, GA. I would say at my first<br />
board meeting I learned a lot about what goes into the making of SPD Certification Exams. I would like to say<br />
thanks to everyone at CBSPD, Inc. and the Chauncey Group. I would like to encourage everyone to run for a<br />
position on the Board of Directors at some point or another. I would like to wish everyone Happy Holiday’s<br />
and a Happy New Year. I can’t wait for the next meeting. Thank you. ▲<br />
Continued on Next Page<br />
January 2004 Criterion - Page 3
Board Thoughts Cont.<br />
Lori Stratton—CSIT, CSPDT, Surgical Instrument Technician Representative: Hi, my name is Lori Stratton<br />
and I was elected to the Board of Directors for the CBSPD this year. I represent the Certified Surgical Instrument<br />
Technicians spot on the Board. I live in northern VT in a small rural town just a few miles from the Canadian<br />
border. It is a very beautiful area year round. I have just returned from my first BOD meeting held in<br />
Flemington, NJ. It just happened to also be during the biggest blizzard the area had seen in quite a few years.<br />
Even by VT standards it was a LOT of snow! We did not let that keep us from the business at hand though. I<br />
have to say this it was a wonderful experience. Being in the same room with some of the heavy hitters in our<br />
area of work was really something. To be able to share in the exchange of information and to also be able to<br />
draw on the expertise of everyone on the board was quite exciting. I must admit that I was unaware of the<br />
amount of work and hours that go into the development of one exam! The dedication and tireless effort that<br />
this board exhibits is camaraderie at its best. I feel very fortunate and humbled to be able to serve for such an<br />
amazing and outstanding group of people and the Certification Board they represent. I rate my first BOD<br />
meeting a 10+. ▲<br />
Karen Santos—LPN, CSPDM, Manager Representative: My<br />
name is Karen Santos. I am a LPN and CSPDM, employed as the<br />
Team Leader/Manager of Central Service at Connecticut Children’s<br />
Medical Center, a 110 bed pediatric hospital in Hartford,<br />
CT. My C.S. career began in 1979 as a C.S. Aide. In 1986 I was<br />
promoted to the Manager’s position and have worked in several<br />
CT hospitals in this position. I have been active in the CT Central<br />
Service Association, serving in all board positions.<br />
Certification began for me through CBSPD (at the time it was<br />
NICHSPDP) in 1990 as a Technician. In 1996 I became certified<br />
as a Manager, with re-certification in 2001. Having been in this<br />
career for so long, I can remember back in 1986 when <strong>Nancy</strong><br />
<strong>Chobin</strong> made the announcement at the ASHCSP annual meeting<br />
held in Hartford that certification was indeed going to become a<br />
reality. I am proud to be able to be a part of this organization,<br />
serving as the Manager representative on the CBSPD Board of<br />
Directors, as well as a member of the Item Review Committee.<br />
The first BOD meeting for me was held on December 5 & 6, 2003. Despite the winter storm, it was a very busy<br />
and productive two days. We traveled to Chauncey International to meet with the staff responsible for preparing<br />
and administering the certification exams. Here we learned the process they use starting with preparation<br />
of the exam all the way through the scoring and statistical analysis after the exam is administered. The<br />
exam does not stop with the final scoring. All questions are individually looked at during the final analysis<br />
for number of candidates answering correctly vs. not correctly, etc. It is difficult to imagine just how much<br />
goes into this whole process. We also were made aware of the amount of security the company maintains<br />
both at their site as well as the test sites throughout the country on the day of the exam.<br />
Other highlights of the meeting included reporting of the test statistics for the last three exams given and those<br />
re-certifying; our affiliation with the ASHCSP; our prestigious recognition by NOCA; and expansion of certification<br />
through CBSPD into several countries including Mexico and South America.<br />
Most of all, what I am learning is how unbelievably dedicated our Executive Director <strong>Nancy</strong> <strong>Chobin</strong> is to this<br />
organization. Her visions of the future for CBSPD are endless and with her diligence I have no doubt she will<br />
achieve them all. She and her executive committee members, Sue McManus, Tam Maresca and Nora Wikander,<br />
all volunteer their time to the CBSPD in addition to their full time hospital positions and family commitments.<br />
They are to be commended for their dedication. ▲<br />
January 2004 Criterion - Page 4
REPORT OF <strong>THE</strong> CONTINUING EDUCATION COMMITTEE<br />
Teckla Ann Maresca, LPN, CSPDM<br />
Nora Wikander, RN, CSPDM<br />
The Continuing Education Committee has reviewed all inservices and programs submitted requesting contact<br />
hour approval. There have been 1,062 individual inservice approvals; 189 for CS Association Seminars, 54<br />
Corporate inservices and 5 Newsletter approvals over the past year.<br />
The Committee continues to experience problems with programs and inservices not being submitted in a<br />
timely manner. In addition, due to the large volume of CEU requests, the Committee will review any requests<br />
that are over 6 months old. The number of individuals who are submitting large numbers of inservices over 1-<br />
2 years old is significant. There have also been non-approvals of CEUs because the topic was not relevant to<br />
the exam content outline.<br />
The Committee is concerned regarding the validity of using CEUs to verify an individual’s competency for recertification<br />
and ask that the Board of Directors re-evaluate this process. ▲<br />
SUE MCMANUS RECEIVES AWARD<br />
ASHCSP President Rose Seavey (left) and ASHCSP Board Member Etta<br />
Bushong (center) presenting the Bill Dennis Huma nitarian Award to Sue<br />
McManus (right) in October 2003.<br />
At the American Society for Healthcare Central<br />
Service Professionals’ Annual Meeting and Conference<br />
in Grand Rapids, MI, Sue McManus, RN,<br />
CSPDM, was awarded the first Bill Dennis Humanitarian<br />
Award. Sue has been a Board Member<br />
of the CBSPD since 1995 and has been the Item Review<br />
(Test Development) Liaison since 1991. Sue’s<br />
personal and professional achievements, including<br />
her many humanitarian contributions, were recognized<br />
by conferring this award on her. It is fitting<br />
that Sue received the award since both she and Bill<br />
Dennis are from North Carolina. Both past president<br />
of NCAHCSP and the ASHCSP, Bill Dennis<br />
was a longtime ASHCSP member who died suddenly<br />
in 2001. The CBSPD is proud of Sue’s receipt<br />
of this prestigious award. ▲<br />
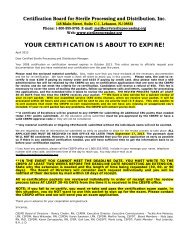
**REMINDER TO ALL UPCOMING APRIL RE-CERTS**<br />
Group #1: You were originally certified on 4/23/94, then re-certified in 1999, and are due again this year.<br />
Please have your completed re-certification packet into the CBSPD office no later than 4/30/04.<br />
Group # 2: You were originally certified on 4/17/99 and are due for re-certification this year. Please have your<br />
completed re-certification packet into the CBSPD office no later than 4/30/04.<br />
January 2004 Criterion - Page 5
Puzzled by Sterilization or Infection<br />
Control Issues?<br />
Ask Pat!<br />
Pat Barnett, RN, CSPDM<br />
Q: Can you find out how long we legally have to keep our sterilization records?<br />
A: Laws governing recommended times vary from state to state. I recommend checking with the legal/risk<br />
management department of your facility. Another resource for this information is your state hospital association.<br />
Most facilities keep sterilization records in the department or readily available for twelve months and<br />
then archive them off campus for up to seven years (if your surgical services is primarily Pediatrics-most recommendations<br />
suggest twenty-one years, as the child has that window of opportunity to bring a suit). You<br />
should also check with your facility’s legal counsel regarding length of time for retention of sterilization records.<br />
Q: I notice that the other CS certification organization is now offering certification tests through the computer<br />
at designated sites. Is this as safe as the certification given semi-annually by CBSPD and are there plans<br />
to change how testing is administered?<br />
A: While people consider computer testing a step up in security from just mailing a test to a hospital and<br />
asking them to administer the test, there is considerable security risks involved with computer testing. In my<br />
opinion, there are definitely far more opportunities to have compromised test results. The process that CBSPD<br />
uses is very similar to the registration test for professional nursing. There are specific security checks throughout<br />
the system and the process is validated.<br />
There are no plans to change our testing process. While computer testing may be more convenient and<br />
probably cheaper to administer; the rigorous measures taken by CBSPD to assure security, offers all of us in<br />
the sterilization field protection against those who use unscrupulous measures to measure their skills and<br />
competency. ▲<br />
PRE-APPROVED INSERVICE<br />
“Supply Distribution Systems”<br />
Bobby L. Osburn, CSPDM<br />
INTRODUCTION TO DISTRIBUTION. The medical and surgical supplies<br />
inventory for the medical center must be managed in a centralized distribution<br />
area. The distribution area of SPD/CS performs a major role in not only getting the<br />
correct supplies and equipment to users but also in assuring that these supplies are in the correct quantity,<br />
quality, location, and condition for use. This allows clinical staff to spend their time on patient care needs. It<br />
also allows large volume purchases and fewer orders to process, which saves the medical center time and resources.<br />
Continued on Next Page<br />
January 2004 Criterion - Page 6
Supply Distribution Systems Inservice Cont.<br />
Items are sent to the user areas via closed carts, exchange carts, covered carts, dumb waiters, and pneumatic<br />
tubes or are hand-carried in impervious bags or containers. All stat items are hand-carried to ensure that these<br />
items are delivered promptly to the area in the critical time of need. Care must be taken to ensure the sterility<br />
of medical supplies and equipment when transporting these items to delivery points throughout the medical<br />
center. Covers must be impervious and completely surround the cart, bin, or item.<br />
TYPES OF DISTRIBUTION<br />
A. When clean and sterile supplies are needed in the user areas of the healthcare facility, they must be transferred<br />
from the SPD/CS department to the point of use. There are five main types of distribution systems<br />
available that may be used to ensure that the correct product is delivered in the right condition and on<br />
time. The type of system used depends on the services the healthcare facility provides, its size, physical<br />
design, age, resources, and mission. The systems are as follows:<br />
[1] DEMAND DISTRIBUTION SYSTEM<br />
(a) Every healthcare facility has used the demand distribution system (also known as a requisition and delivery<br />
distribution system) at one time or another. In this system, the staffs of various user areas are responsible<br />
for maintaining an adequate level of supplies for use in that area. When supplies must be replenished,<br />
or an individual item is needed, the user must prepare a requisition and request the necessary<br />
items, usually by telephone or in person. The SPD/CS staff fills the order and delivers it to the user area<br />
by dumb waiter or in person. After delivery of the items, the requesting user is responsible for storing the<br />
items or transferring them to the point of use. This distribution system is generally carried out on a regularly<br />
scheduled basis or as needed, hence the term "Demand" Distribution System.<br />
(b) The Demand Distribution System is a simple process and has fulfilled supply needs for the healthcare facilities<br />
for many years. There is a tendency to maintain high levels of stock (hoarding) in the user area to<br />
eliminate frequent requisitioning and documentation. Maintaining excessively high inventories can be<br />
very costly to healthcare facilities. The disadvantages of the demand system are as follows:<br />
⇒ The method is very labor-intensive. It is generally unsuitable for high-volume distribution in a large facility.<br />
⇒ Personnel in the user areas generally have patient care responsibilities and other priorities and do not<br />
have the time or the training to commit themselves to do adequate inventory control.<br />
[2] PAR-LEVEL RESTOCKING DISTRIBUTION SYSTEM<br />
(a) In this type of system, an inventory or par-level is set for each stocked item used daily. These levels<br />
should be reviewed frequently and changed as necessary to reflect actual usage. The SPD/CS technician<br />
is responsible for reviewing the levels daily as stock is being inventoried and maintained. The SPD/CS<br />
technician should communicate with the customers in order to make necessary changes based on patient<br />
care needs. Supply closets, treatment rooms, and nurse servers are used for storage of these supplies.<br />
(b) A typical procedure to maintain stock in the areas is to assign a technician to each area(s). The technician<br />
will inventory all supplies in the treatment rooms, supply closets, and other areas where supplies are<br />
stocked. The technician will return to the SPD/CS department and fill in the inventory sheets or have<br />
them filled by other technicians. When the supplies have been obtained, the technician then replenishes<br />
the user area with the preset "par-levels." Healthcare facilities utilizing nurse servers for patient care supplies<br />
also use a par-level restocking system.<br />
(c) A listing of all needed supply items and levels are posted on the inside of the nurse servers; therefore, the<br />
user and the SPD/CS technicians will know what should be readily available at all times for patient care.<br />
The nurse servers are stocked with supplies as needed to bring supply levels up to "par" or preset levels.<br />
Nurse servers are usually restocked from a mobile supply cart that contains all needed supplies. This cart<br />
is inventoried and restocked daily by the SPD/CS technician. The par-level system is user-friendly in that<br />
the users no longer have the time-consuming task of maintaining their own supply inventory, and inventories<br />
can be maintained at more optimum levels than in the demand system. In most healthcare facilities,<br />
this system provides an excellent means of tracking the use of patient care items.<br />
Continued on Next Page<br />
January 2004 Criterion - Page 7
Supply Distribution Systems Inservice Cont.<br />
(d) The disadvantage of this system is that distribution is a timely process if the healthcare facility is large or<br />
spread over several areas. Some medical centers use a replenishment cart, which the SPD/CS technician<br />
takes to each area for restocking medical supplies to par-levels. This procedure may require the technician<br />
to return to the SPD/CS department frequently for restocking the replenishment cart.<br />
(e) Point-of-Use Equipment. Point-of-Use (POU) equipment is an automatic dispensing system that provides<br />
secured storage of supplies close to where the supplies are used. Access to supplies is limited to employees<br />
who are provided passwords. The use of POU should be considered for areas with high cost and high<br />
volume to track actual costs to patient or procedure. These units may also have potential for remote clinics<br />
and areas where inventory managers are not assigned, such as community based outpatient clinics.<br />
The POU equipment not only allows for tracking usage, but also reduces the consumption and loss of<br />
products.<br />
(3) EXCHANGE CART SYSTEM<br />
(a) The exchange cart system, like the par-level restocking system, has pre-set levels that have been established<br />
by the user and the SPD/CS technician. In the exchange cart system, two identical carts are stocked<br />
with supplies. Once the levels of these carts have been established, one cart is placed in the user<br />
area and one in SPD/CS. On a regular basis, the cart in the user area is returned to SPD/CS<br />
and the identical (fully stocked) cart in SPD/CS is exchanged in its place.<br />
(b) The exchange cart system is practical, flexible, dependable, easy to manage, and can be<br />
used in all healthcare facilities. This system allows for thorough documentation, good<br />
control of patient care supplies, and identification of lost stock. This distribution<br />
system can be extremely cost-effective through its control of inventory, timesaving,<br />
and manpower. The disadvantages of this system are that duplication of stock<br />
and large amounts of space are needed for storage and handling of carts in the<br />
SPD/CS distribution section. The cost to establish this system can be very expensive<br />
due to the initial purchase of the exchange carts and the additional inventory<br />
required to stock them.<br />
(4) CASE CART SYSTEM<br />
(a) In the case cart system, the operating room is provided with selected supplies for each surgery via a case<br />
cart system. These case carts have supplies and instruments that will be used for individual cases. The<br />
supplies and instruments for the case cart system can be provided by different methods, such as procedure<br />
cards, computer printouts, and requisition forms. The method used most frequently is the computer<br />
printout. In this method, each surgery is generally assigned a computer number by SPD/CS. The surgery<br />
schedule is given to the SPD/CS computer operator who generates a case care listing for each surgery.<br />
When surgery receives the schedule, a computer number is assigned to each case accordingly. These computer<br />
case cart sheets are given to the SPD/CS technician who fills the case carts with supplies and instruments<br />
that are located in SPD/CS. The case carts are filled according to the time the surgery is scheduled<br />
for the next day. All scheduled first case carts are delivered and placed in the operating room or clean<br />
corridor until time for use. All other case carts are delivered to the operating room at the time of need. At<br />
the completion of the surgery, all contaminated supplies are placed within the soiled holding area. The<br />
carts are retrieved by SPD/CS personnel and taken to the decontamination area for reprocessing.<br />
(b) A major advantage for using the case cart system is the efficiency and cost savings that can be gained by<br />
concentrating processing and inventory management expertise and equipment in SPD/CS. Another advantage<br />
is the improvement of patient care during surgical intervention. By removing non-nursing activities,<br />
the nursing staff can spend more time on patient care and implementation of the nursing process.<br />
Patient care and employee safety can be enhanced by the effective infection control that the case cart system<br />
provides. Using a separate cart for each case can provide confinement and containment. A closed<br />
case cart system provides for enhanced infection control. The implementation of a case cart system avoids<br />
costly duplication of effort, equipment, and inventory. When case carts are prepared for each procedure,<br />
there is better control of inventory which results in cost savings.<br />
Continued on Next Page<br />
January 2004 Criterion - Page 8
Supply Distribution Systems Inservice Cont.<br />
(5) SPECIALTY CARTS<br />
(a) Specialty carts are carts that contain supplies needed in emergency or special situations. Specialty carts<br />
include the following: disaster, implant, crash or code carts, and special procedure carts, such as arterial<br />
line, central line, Swanz Ganz, urology, and suture.<br />
⇒ Disaster carts are stocked with medical supplies needed for use in emergencies (internal/external disasters)<br />
such as a large traffic accident, bombing, or flood. These supplies should be stocked on a cart that<br />
can be easily transported to the scene of the disaster. Transportation of the carts should be conducted in a<br />
manner so as not to compromise the medical supplies contained within the cart. It is recommended that<br />
the contents of disaster carts be reviewed and updated as needed or, at minimum, on an annual basis.<br />
⇒ Implant carts are stocked with implants, such as intraocular lenses, vascular grafts, and knee and hip prostheses<br />
that are transported to the operating room at the time of surgery.<br />
⇒ Crash or code carts are specialty carts used in emergency situations to revive victims from respiratory failure<br />
or cardiac arrest. SPD/CS personnel stock these carts with medical supplies, and the pharmacy department<br />
stocks drugs and intravenous solutions. Code or crash carts containing supplies and drugs are<br />
to be kept locked to secure their contents. Filled crash carts are maintained throughout medical facilities<br />
so that they can be utilized quickly during emergencies. Backup crash carts are readily available in SPD/<br />
CS for exchange when one is used. The outside of the code or crash cart should be inspected daily by hospital<br />
personnel to ensure the security of the cart and exterior supplies and equipment. The outside of the<br />
code or crash cart will contain a listing of all supplies that are needed.<br />
(b) Specialty carts will be cleaned between use, or as needed, and brought to the receiving area of SPD/CS.<br />
Contents will be removed and inspected before taking the cart to the decontamination area for processing.<br />
Under no circumstances will medical supplies be taken into the decontamination area. Any item taken<br />
into the decontamination area must be considered contaminated. Any item that cannot be reprocessed<br />
(i.e., single use or disposable items) will be disposed of.<br />
B. The type of system used depends on the services the healthcare facility provides, its size, physical design,<br />
age, resources, and mission. SPD/CS management may periodically reevaluate their distribution systems<br />
in order to meet the current demands placed on the facility (e.g., census, finances). The important considerations<br />
in evaluating a distribution system are whether it provides information on future supply needs,<br />
the timeliness and accuracy with which supplies can be made available to the user, and how the system<br />
provides for control and documentation of inventory movement. It is important that the technicians be<br />
familiar with the characteristics, advantages, and disadvantages of each type of distribution system. This<br />
way they can better understand why a particular system is used at their medical system and how they can<br />
help make their distribution system as cost-effective, reliable, and efficient as possible.<br />
DELIVERY METHODS AND EQUIPMENT. Several methods and types of equipment are used to deliver<br />
and store medical supplies. Distribution carts are used to transport and store supplies. Dumbwaiters and<br />
other mechanical devices are used to transport small quantities of supplies to the point of use upon request.<br />
In emergency situations, SPD/CS personnel may be requested to deliver items "stat" ("stat" meaning immediately).<br />
"Stat" supplies will be delivered by the fastest method available, preferably hand delivery. Hand delivery<br />
will ensure the needed items reach the point of use as soon as possible. Mechanical devices cannot ensure<br />
that "stat" items reach their destination, due to a possible power failure or electrical outage. Users can obtain<br />
items directly from SPD/CS. This is called window distribution, which is utilized by some healthcare facilities.<br />
DISTRIBUTION WORK PRACTICES. SPD/CS personnel must remember that careful handling and timely<br />
delivery of supplies are needed in the patient care area. If not, the user may lose confidence in SPD/CS services.<br />
This will cause the users to hoard supplies resulting in duplication that can be costly. Patient care can<br />
be adversely affected if the right item is not delivered, in the right condition, at the right time, and ready for<br />
use.<br />
Answer Key to Post Test: 1:D, 2:B, 3:D, 4:A, 5:C, 6:D, 7:C, 8:D, 9:B, 10:C<br />
Continued on Next Page<br />
January 2004 Criterion - Page 9
Supply Distribution Systems Inservice Cont.<br />
SELECTION OF ITEMS <strong>FROM</strong> INVENTORY. The distribution process begins when a request is received<br />
for supplies or equipment. These items should be handled carefully to avoid damage or contamination. The<br />
type and quantity of items should be verified before transporting them to the point of use. All items used in<br />
or distributed by SPD/CS must be checked for expiration date and external chemical indicator (to verify the<br />
item was subjected to the sterilization process). In addition, all packages and items will be inspected to ensure<br />
that the packaging is not damaged, wet, or soiled.<br />
DELIVERY OF ITEMS TO PATIENT CARE AREAS. During transport, clean and sterile supplies must be<br />
covered or enclosed to protect the supplies from the environmental hazards. Distribution carts, which are<br />
used for the transport of clean or sterile supplies, must have a barrier or solid bottom shelf protecting the supplies<br />
from the wheels and floor. Items that fall on the floor during transport must be inspected for damage to<br />
determine if there is a need for reprocessing or disposal. Clean/sterile supplies will never be transported on<br />
the same carts or in the same containers as contaminated. SPD/CS technicians will never leave distribution<br />
carts unattended. Leaving carts unattended could cause patient/employee injury, loss or theft of supplies,<br />
and contamination of clean or sterile supplies.<br />
Supply Distribution Systems Test—January 2004 Criterion<br />
THIS PRE-APPROVED INSERVIC E IS WORTH 1 CEU<br />
1. The five methods of Distribution of Medical/Surgical supplies to users area are; Par-level, Exchange Cart,<br />
Case Cart, Specialty Cart and _______________.<br />
A) Normal<br />
B) Emergency<br />
C) Run out<br />
D) Demand<br />
2. With the Par-Level distribution method, who makes sure the<br />
supplies are at the proper level?<br />
A) The user<br />
B) The SPD/CS Tech<br />
C) The Ward Clerk<br />
D) The Doctor<br />
3. Transports carts must:<br />
A) be closed or have impervious cover<br />
B) protect the supplies from being damages<br />
C) be easy to push<br />
D) all of the above<br />
4. With the Demand distribution method, who makes sure the supplies<br />
are at the proper level?<br />
A) The user<br />
B) The SPD/CS Tech<br />
C) The vendor<br />
D) The Director of SPD/CS<br />
Questions 5-10 On Next Page<br />
January 2004 Criterion - Page 10
Supply Distribution Systems Test Cont.<br />
5. The Par-level distribution method has several advantages, but one of the biggest is:<br />
A) It takes a lot of time for the SPD/CS Staff<br />
B) It keeps the SPD/CS tech out SPD/CS<br />
C) It frees the user up to do patent care and not doing inventory management<br />
D) It increases the stock levels<br />
6. Specialty Carts are:<br />
A) Carts use to transport medical/surgical supplies to user are for restocking<br />
B) A-line type carts used inside SPD/CS to pull supplies for larger carts<br />
C) Carts with special wheels for use in hospitals<br />
D) Carts that contain supplies needed in a emergency or special situations<br />
7. Which of the following statements is not true regarding Exchange-Carts?<br />
A) Exchange carts allow for flexibility in stocking users areas<br />
B) They are easy to manage<br />
C) They take less space and inventory to manage than other methods<br />
D) Can be used in all healthcare facilities<br />
8. Crash or Code carts is an example of a Specialty Carts used to:<br />
A) Control bleeding<br />
B) For isolation<br />
C) For burn patients<br />
D) Revive victims from respiratory failure or cardiac arrest<br />
9. Case carts are set up and used primarily for:<br />
A) Cath Lab<br />
B) Operating Room<br />
C) X-ray<br />
D) Emergency Room<br />
10. Some of the key advantages of the case cart system are:<br />
A) Allow the O.R. staff to blame the SPD/CS staff for all problems<br />
and missing items<br />
B) Gives SPD/CS staff an important roll in surgery<br />
C) It provides efficiency and cost saving, allows O.R. to speed more time with patient care duties, and<br />
enhanced infection control<br />
D) It takes less instruments.<br />
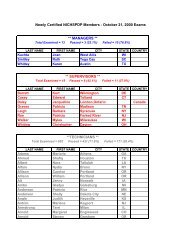
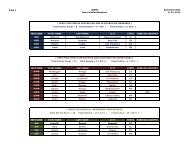
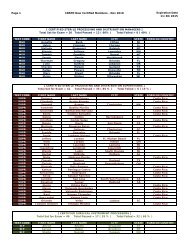
**OCTOBER 2003 CBSPD CERTIFICATION EXAM STATS**<br />
TECHNICIAN: Total Sat for Exam = 669; Total Passed = 533 (80%); Total Failed = 136 (20%)<br />
MANAGER: Total Sat for Exam = 10; Total Passed = 3 (30%); Total Failed = 7 (70%)<br />
SUPERVISOR: Total Sat for Exam = 22; Total Passed = 14 (64%); Total Failed = 8 (36%)<br />
SURGICAL INSTRUMENT TECH: Total Sat for Exam=41; Total Passed=21 (51%); Total Failed=20 (49%)<br />
January 2004 Criterion - Page 11
OPINION SECTION - It’s Time to GROW-UP!<br />
<strong>Nancy</strong> <strong>Chobin</strong>, RN, CSPDM<br />
Everyone talks about the lack of respect for the sterile processing profession. Low salaries, no recognition, etc.<br />
Even the common public is not aware of our existence. How often have you told someone that you work in<br />
Central Service/Sterile Processing and they say “what’s that?”. Everyone knows Housekeeping, Dietary, etc.<br />
but not CS/SPD. Whose fault is that? Ours! We do not do enough to promote this noble profession. And no<br />
one is going to resolve the problems for CS/SPD personnel unless we do because it is our problem. It is time<br />
we GROW UP and take responsibility.<br />
What is needed is a massive public awareness campaign to focus on what we do and how critical our jobs are<br />
to the public health. We need to mandate certification for all CS/SPD workers and we need to make sure that<br />
people who get certified are recognized by title and salary. If nurses and other professionals are recognized<br />
by title and salary for their certifications, why not us?<br />
Many individuals still envision the sterile processing worker preparing thermometers and bedpans as we did<br />
many years ago. When was the last time someone from Administration visited your department? Do you<br />
prepare a storyboard or other type of display during CS/SPD week to demonstrate to your hospital colleagues<br />
exactly what you do? There is a saying that goes “if you cannot bring Mohammed to the mountain…then<br />
bring the mountain to Mohammed!” Maybe you should try this! Does anyone who purchases the highly sophisticated<br />
surgical devices ever say to themselves “I wonder who will clean and sterilize this?”. Probably<br />
not. Hospitals spend hundreds of thousands of dollars on surgical instruments and specialty devices. Does<br />
anyone consider the time to disassemble, clean, reassemble, inspect, package, sterile and store the device? We<br />
have grown up and our jobs have changed dramatically. With that change came the urgent need for training,<br />
education, competency and now certification.<br />
A good example of this crisis is airport security workers. These people are some of the lowest paid people in<br />
airport security yet how important is their screening to your safety? Same thing in CS/SPD. Low pay, yet<br />
tremendous responsibility.<br />
Our profession is relatively new when compared to others but we have training materials and programs in<br />
place to facilitate preparation for certification examinations. We need to convince the public and hospital administrations<br />
that a competent sterile processing team will reduce costs, improve patient safety and increase<br />
surgeon satisfaction. We also need to promote the profession and ensure decent salaries to not only attract<br />
new people but to retain those we have. There is something inherently wrong in healthcare when a person<br />
can make more money at McDonald’s than in sterile processing.<br />
Look for the CBSPD to be very vocal this year and in the years to come. We plan to continue to speak up for<br />
the sterile processing professionals around the world….because we are worth it and because our patients deserve<br />
the best care available.<br />
January 2004 Criterion - Page 12