PARENT/CAMPER KIT - the Cooperstown Dreams Park
PARENT/CAMPER KIT - the Cooperstown Dreams Park
PARENT/CAMPER KIT - the Cooperstown Dreams Park

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
6<br />
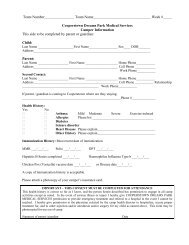
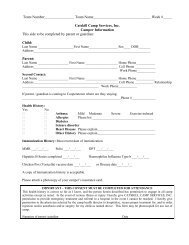
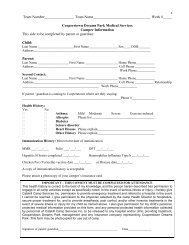
Team Number________________ Team Name_______________________________ Week #_____<br />
<strong>Cooperstown</strong> <strong>Dreams</strong> <strong>Park</strong> Medical Services<br />
Camper Information<br />
This side to be completed by parent or guardian:<br />
Child:<br />
Last Name _____________________First Name_________________ Sex____ DOB_______<br />
Address_____________________________________________________________________<br />
Parent:<br />
Last Name __________________ First Name ___________________ Home Phone___________<br />
Address__________________________________________________ Cell Phone ____________<br />
Work Phone___________<br />
Second Contact:<br />
Last Name __________________ First Name ___________________ Home Phone___________<br />
Address__________________________________________________ Cell Phone ___________ Relationship<br />
_____________________________________________ Work Phone___________<br />
If parent / guardian is coming to <strong>Cooperstown</strong> where are <strong>the</strong>y staying:<br />
__________________________________________________________Phone #______________<br />
Health History:<br />
Yes No<br />
Asthma: Mild Moderate Severe Exercise induced<br />
Allergies Please list ____________________________________<br />
Diabetes<br />
Seizure disorder<br />
Heart Disease Please explain__________________________________<br />
O<strong>the</strong>r History Please explain__________________________________<br />
Immunization History: Most recent date of immunization<br />
MMR ___/___/___ Polio ___/___/___ DPT ___/___/___<br />
Hepatitis B Series completed ___/___/___<br />
Haemophilus Influenza Type b ___/___/___<br />
Chicken Pox (Varicella) vaccine date ___/___/___<br />
or Disease date___/___/__<br />
A copy of immunization history is acceptable.<br />
Please attach a photocopy of your camper’s insurance card.<br />
IMPORTANT – THIS CONSENT MUST BE COMPLETED FOR ATTENDANCE<br />
This health history is correct to <strong>the</strong> best of my knowledge, and <strong>the</strong> person herein described has permission to<br />
engage in all camp activities except as specifically noted. In <strong>the</strong> event of serious illness or injury, I hereby give<br />
Catskill Camp Services Inc. permission to provide emergency treatment and referral to a hospital in <strong>the</strong> event<br />
I cannot be reached. I give permission to <strong>the</strong> physician selected by <strong>the</strong> camp Health Director to hospitalize,<br />
secure proper treatment for, and to provide anes<strong>the</strong>sia, pain control, and/or o<strong>the</strong>r invasive treatments in <strong>the</strong><br />
event of severe illness or injury for my child as named above. I also give permission for my child’s personal,<br />
protected medical information provided on this form, and any personal protected health information collected<br />
by personnel of Catskill Camp Services Inc. to be released to any hospital and/or clinic providing treatment,<br />
<strong>Cooperstown</strong> <strong>Dreams</strong> <strong>Park</strong> management and any insurance company representing <strong>Cooperstown</strong> <strong>Dreams</strong><br />
<strong>Park</strong>. This form may be photocopied for use out of camp.<br />
Signature of parent/ guardian______________________________________<br />
Date_______________