ATAPS Referral Form - WentWest
ATAPS Referral Form - WentWest
ATAPS Referral Form - WentWest

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
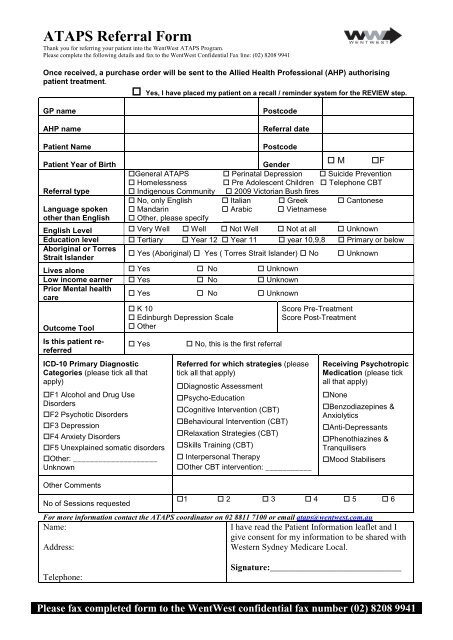
<strong>ATAPS</strong> <strong>Referral</strong> <strong>Form</strong><br />
Thank you for referring your patient into the <strong>WentWest</strong> <strong>ATAPS</strong> Program.<br />
Please complete the following details and fax to the <strong>WentWest</strong> Confidential Fax line: (02) 8208 9941<br />
Once received, a purchase order will be sent to the Allied Health Professional (AHP) authorising<br />
patient treatment.<br />
Yes, I have placed my patient on a recall / reminder system for the REVIEW step.<br />
GP name<br />
AHP name<br />
Postcode<br />
<strong>Referral</strong> date<br />
Patient Name<br />
Patient Year of Birth<br />
<strong>Referral</strong> type<br />
Language spoken<br />
other than English<br />
Postcode<br />
Gender<br />
M F<br />
General <strong>ATAPS</strong> Perinatal Depression Suicide Prevention<br />
Homelessness Pre Adolescent Children Telephone CBT<br />
Indigenous Community 2009 Victorian Bush fires<br />
No, only English Italian Greek Cantonese<br />
Mandarin Arabic Vietnamese<br />
Other, please specify<br />
English Level Very Well Well Not Well Not at all Unknown<br />
Education level Tertiary Year 12 Year 11 year 10,9,8 Primary or below<br />
Aboriginal or Torres<br />
Yes (Aboriginal) Yes ( Torres Strait Islander) No Unknown<br />
Strait Islander<br />
Lives alone Yes No Unknown<br />
Low income earner Yes No Unknown<br />
Prior Mental health<br />
care<br />
Yes No Unknown<br />
Outcome Tool<br />
Is this patient rereferred<br />
K 10<br />
Edinburgh Depression Scale<br />
Other<br />
Yes<br />
ICD-10 Primary Diagnostic<br />
Categories (please tick all that<br />
apply)<br />
F1 Alcohol and Drug Use<br />
Disorders<br />
F2 Psychotic Disorders<br />
F3 Depression<br />
F4 Anxiety Disorders<br />
F5 Unexplained somatic disorders<br />
Other: ____________________<br />
Unknown<br />
Other Comments<br />
No of Sessions requested<br />
No, this is the first referral<br />
Referred for which strategies (please<br />
tick all that apply)<br />
Diagnostic Assessment<br />
Psycho-Education<br />
Cognitive Intervention (CBT)<br />
Behavioural Intervention (CBT)<br />
Relaxation Strategies (CBT)<br />
Skills Training (CBT)<br />
Interpersonal Therapy<br />
Other CBT intervention: ___________<br />
Score Pre-Treatment<br />
Score Post-Treatment<br />
Receiving Psychotropic<br />
Medication (please tick<br />
all that apply)<br />
None<br />
Benzodiazepines &<br />
Anxiolytics<br />
Anti-Depressants<br />
Phenothiazines &<br />
Tranquilisers<br />
Mood Stabilisers<br />
1 2 3 4 5 6<br />
For more information contact the <strong>ATAPS</strong> coordinator on 02 8811 7100 or email ataps@wentwest.com.au<br />
Name:<br />
I have read the Patient Information leaflet and I<br />
give consent for my information to be shared with<br />
Address:<br />
Western Sydney Medicare Local.<br />
Telephone:<br />
Signature:______________________________<br />
Please fax completed form to the <strong>WentWest</strong> confidential fax number (02) 8208 9941
<strong>ATAPS</strong> <strong>Referral</strong> <strong>Form</strong><br />
Thank you for referring your patient into the <strong>WentWest</strong> <strong>ATAPS</strong> Program.<br />
Please complete the following details and fax to the <strong>WentWest</strong> Confidential Fax line: (02) 8208 9941<br />
Group Sessions Section<br />
Type of Group Anger Busters Anxiety Busters<br />
Anxiety Management<br />
Managing Insomnia<br />
Depression Management<br />
Perinatal Group Therapy<br />
Risk of Harm to Self Suitability: Mild Moderate<br />
Comments if any:<br />
Risk of Harm to Others<br />
Affects on Functioning in a Group<br />
Setting<br />
Clinical Information/ Reason for<br />
<strong>Referral</strong><br />
Any Other Providers Involved in<br />
Care<br />
I have informed the patient that the triage service will contact them.<br />
Patients contact number.<br />
Please fax completed form to the <strong>WentWest</strong> confidential fax number (02) 8208 9941