BIORESORB® Macro Pore Augmentation material - Optident
BIORESORB® Macro Pore Augmentation material - Optident
BIORESORB® Macro Pore Augmentation material - Optident

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
BIORESORB ® <strong>Macro</strong> <strong>Pore</strong><br />
<strong>Augmentation</strong> <strong>material</strong><br />
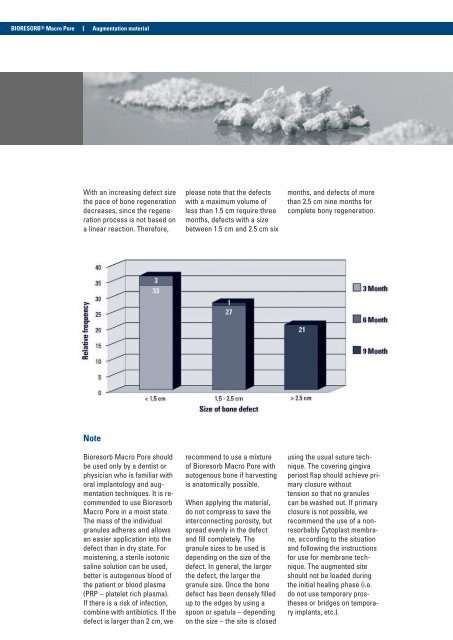
With an increasing defect size<br />
the pace of bone regeneration<br />
decreases, since the regeneration<br />
process is not based on<br />
a linear reaction. Therefore,<br />
please note that the defects<br />
with a maximum volume of<br />
less than 1.5 cm require three<br />
months, defects with a size<br />
between 1.5 cm and 2.5 cm six<br />
months, and defects of more<br />
than 2.5 cm nine months for<br />
complete bony regeneration.<br />
Note<br />
Bioresorb <strong>Macro</strong> <strong>Pore</strong> should<br />
be used only by a dentist or<br />
physician who is familiar with<br />
oral implantology and augmentation<br />
techniques. It is recommended<br />
to use Bioresorb<br />
<strong>Macro</strong> <strong>Pore</strong> in a moist state.<br />
The mass of the individual<br />
granules adheres and allows<br />
an easier application into the<br />
defect than in dry state. For<br />
moistening, a sterile isotonic<br />
saline solution can be used,<br />
better is autogenous blood of<br />
the patient or blood plasma<br />
(PRP – platelet rich plasma).<br />
If there is a risk of infection,<br />
combine with antibiotics. If the<br />
defect is larger than 2 cm, we<br />
recommend to use a mixture<br />
of Bioresorb <strong>Macro</strong> <strong>Pore</strong> with<br />
autogenous bone if harvesting<br />
is anatomically possible.<br />
When applying the <strong>material</strong>,<br />
do not compress to save the<br />
interconnecting porosity, but<br />
spread evenly in the defect<br />
and fill completely. The<br />
granule sizes to be used is<br />
depending on the size of the<br />
defect. In general, the larger<br />
the defect, the larger the<br />
granule size. Once the bone<br />
defect has been densely filled<br />
up to the edges by using a<br />
spoon or spatula – depending<br />
on the size – the site is closed<br />
using the usual suture technique.<br />
The covering gingiva<br />
periost flap should achieve primary<br />
closure without<br />
tension so that no granules<br />
can be washed out. If primary<br />
closure is not possible, we<br />
recommend the use of a nonresorbably<br />
Cytoplast membrane,<br />
according to the situation<br />
and following the instructions<br />
for use for membrane technique.<br />
The augmented site<br />
should not be loaded during<br />
the initial healing phase (i.e.<br />
do not use temporary prostheses<br />
or bridges on temporary<br />
implants, etc.).