RCPA Examinations in Anatomical pathology - Questions ... - Rcpa.tv
RCPA Examinations in Anatomical pathology - Questions ... - Rcpa.tv
RCPA Examinations in Anatomical pathology - Questions ... - Rcpa.tv

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Exam Update<br />
2008<br />
<strong>Anatomical</strong> Pathology<br />
10.3.06
Myths, Smoke and Mirrors<br />
The big myth is that <strong>in</strong>formation about tra<strong>in</strong><strong>in</strong>g and exam<strong>in</strong>ations is<br />
not available from the Board of Censors<br />
The “smoke and mirrors” appears to come from <strong>in</strong>dividuals who have<br />
not made any attempt to access the available <strong>in</strong>formation<br />
The follow<strong>in</strong>g slides show the material available to supervisors and<br />
candidates, compiled from <strong>in</strong>formation supplied predom<strong>in</strong>antly by<br />
the efforts of Members of the Board of Censors<br />
10.3.06
Available Information<br />
What is the Board of Censors and what is the Board’s<br />
mandate?<br />
• Available Information<br />
– Generic<br />
• <strong>RCPA</strong> Articles of Association<br />
10.3.06
Available Information<br />
<strong>RCPA</strong> ARTICLES OF ASSOCIATION<br />
BOARD OF CENSORS<br />
Appo<strong>in</strong>tment and Powers<br />
45. The Council shall have the power from time to time to appo<strong>in</strong>t censors<br />
to constitute a Board of Censors for the purpose of <strong>in</strong>quir<strong>in</strong>g <strong>in</strong>to and<br />
test<strong>in</strong>g the qualifications of candidates for membership of the College<br />
and to appo<strong>in</strong>t a Chairman of the Board of Censors. The Council may<br />
make by-laws def<strong>in</strong><strong>in</strong>g the powers of the Board of Censors and the<br />
Chairman thereof and prescrib<strong>in</strong>g rules for its procedure<br />
Council May Exercise Powers Where no Board of Censors<br />
46. At any time when there shall not be a Board of Censors <strong>in</strong> existence<br />
the Council may exercise and perform any powers duties and<br />
functions conferred or imposed on the Board of Censors by these<br />
Articles. The Council may from time to time co-opt not more than three<br />
additional Fellows of the College to be members of the Council for the<br />
purpose of exercis<strong>in</strong>g the last mentioned powers duties and functions.<br />
10.3.06
Available Information (cont.)<br />
Policy Manual – Guidel<strong>in</strong>es<br />
• Admission to Fellowship by Viva Exam<strong>in</strong>ation Alone<br />
• Assessment of Tra<strong>in</strong><strong>in</strong>g Programs for Accreditation of <strong>RCPA</strong><br />
Tra<strong>in</strong><strong>in</strong>g: Process for Assessment of Adequate Staff<strong>in</strong>g Levels<br />
• Jo<strong>in</strong>t Tra<strong>in</strong><strong>in</strong>g Programs with the Royal Australasian College of<br />
Physicians<br />
• Interview of Overseas Tra<strong>in</strong>ed Specialists<br />
10.3.06
Available Information (cont.)<br />
Policy Manual - Policies<br />
• Appo<strong>in</strong>tment to Major Committees<br />
• Assessment of Overseas Tra<strong>in</strong>ed doctors and Overseas Tra<strong>in</strong>ed<br />
Specialists <strong>in</strong> australia and new Zealand<br />
• <strong>Exam<strong>in</strong>ations</strong> for Overseas Tra<strong>in</strong>ed Specialists Incorporat<strong>in</strong>g Tim<strong>in</strong>g<br />
of Part II <strong>Exam<strong>in</strong>ations</strong><br />
• Interrupted and Part-time Tra<strong>in</strong><strong>in</strong>g<br />
• Repeat <strong>Exam<strong>in</strong>ations</strong><br />
• Selection of Exam<strong>in</strong>ers for the College<br />
10.3.06
Available Information (cont.)<br />
Policy Manual - Roles and Responsibilities<br />
• Chief Exam<strong>in</strong>ers and Associate Chief Exam<strong>in</strong>ers<br />
• Ombudsman for Tra<strong>in</strong>ees<br />
• Registrar and Deputy Registrar<br />
Policy Manual - Terms of Reference<br />
• Board of Censors<br />
• Tra<strong>in</strong><strong>in</strong>g and Exams - Accredited Labs<br />
• 2007 Lab Audit Form<br />
10.3.06
Available Information (cont.)<br />
Tra<strong>in</strong><strong>in</strong>g and Exams - Accredited Labs<br />
• Accredited Laboratories for <strong>RCPA</strong> Tra<strong>in</strong><strong>in</strong>g<br />
• Plus all forms for accreditation for <strong>in</strong>dividual discipl<strong>in</strong>es<br />
• Step Guide: Assessment of labs seek<strong>in</strong>g accreditation to tra<strong>in</strong><br />
Registrars of the <strong>RCPA</strong> and renewal of lab accreditation Jan 2008<br />
• The Board of Censors have full bus<strong>in</strong>ess meet<strong>in</strong>gs <strong>in</strong> March, July and<br />
November of each year. The dates for 2008 are 17 March, 14 July and<br />
24 November.<br />
10.3.06
Available Information (cont.)<br />
Tra<strong>in</strong><strong>in</strong>g and Exams - Exam Information<br />
• <strong>Anatomical</strong> Pathology Part I Candidates Instructions<br />
• <strong>Anatomical</strong> Pathology Part I Candidates Slides proforma<br />
• <strong>Anatomical</strong> Pathology Part II Candidates Instructions<br />
• APII Part II Practical and Slides candidates <strong>in</strong>structions<br />
• <strong>Anatomical</strong> Pathology Part II Slides proforma<br />
• AP Exam Presentation 2004<br />
• Presentation on AP exams at Pathology Update 2003 (192 kb)<br />
• AP exam presentation 2005 (536 kb)<br />
• Information given at Pathology Update 2005, re AP exams and 2004 Part II slides<br />
• AP Exams Update - March 2007<br />
• <strong>RCPA</strong> June 2007 Exam Venues 11 May07<br />
• <strong>RCPA</strong> November Exam<strong>in</strong>ation Timetable<br />
10.3.06
Available Information (cont.)<br />
Tra<strong>in</strong><strong>in</strong>g and Exams - Forms<br />
• Annual Registration and Exam Information 2008<br />
• Annual Registration and Exam Information 2008<br />
• Application for Annual Registration 2008<br />
• Autopsy Assessment Form (AP Tra<strong>in</strong>ees)<br />
• College Information 2008<br />
• Confirmation of Completion of Supervisors Module<br />
• Draft Exam Timetable 2008 as at 2Jan08<br />
• Exam<strong>in</strong>ation Application 2008<br />
• Exam<strong>in</strong>ation Application Information 2008<br />
• Fellowship Application Form 2007/8<br />
• Selection of Exam<strong>in</strong>ers<br />
10.3.06
Available Information (cont.)<br />
Tra<strong>in</strong><strong>in</strong>g and Exams - Past Exam Papers<br />
• <strong>Anatomical</strong> Pathology Part 1 Written Exams - 2006<br />
• <strong>Anatomical</strong> Pathology Part I Written Exam 2005<br />
• <strong>Anatomical</strong> Pathology Part I Written Exam Paper 2004<br />
• <strong>Anatomical</strong> Pathology Part I Written Exams 1999 - 2003<br />
• <strong>Anatomical</strong> Pathology Part II Forensic Slant 2005<br />
• <strong>Anatomical</strong> Pathology Part II Slant 2001<br />
• <strong>Anatomical</strong> Pathology Part II Slant Past Exams<br />
• <strong>Anatomical</strong> Pathology Part II Slant 2004<br />
• <strong>Anatomical</strong> Pathology PartII Slant 2006<br />
• Diploma of Cyto<strong>pathology</strong> Written Exam 2001<br />
• Diploma of Forensic Medic<strong>in</strong>e Exams 2001 - 2003<br />
10.3.06
Available Information (cont.)<br />
Tra<strong>in</strong><strong>in</strong>g and Exams - Policies<br />
• Acceptance of Australian Tra<strong>in</strong>ed International Medical Graduates onto <strong>RCPA</strong> Tra<strong>in</strong><strong>in</strong>g Programs <strong>in</strong> Australia<br />
• Admission to Fellowship by Viva Exam<strong>in</strong>ation Alone<br />
• Appo<strong>in</strong>tment of Pathology Registrars<br />
• Assessment of Overseas Tra<strong>in</strong>ed Specialists seek<strong>in</strong>g Medical Registration <strong>in</strong> Australia or New Zealand via the Australian Medical Council and the Medical Council of New<br />
Zealand Processes<br />
• Candidates <strong>in</strong> Tra<strong>in</strong><strong>in</strong>g and Sitt<strong>in</strong>g <strong>Exam<strong>in</strong>ations</strong> <strong>in</strong> Countries without College Representation<br />
• Information for Tra<strong>in</strong>ees <strong>in</strong> countries without a regional councillor or correspond<strong>in</strong>g felow<br />
• Cl<strong>in</strong>ical Privilege Guidel<strong>in</strong>es for Forensic Pathology Registrars<br />
• Cl<strong>in</strong>ical Privileges for Pathology Tra<strong>in</strong>ees<br />
• Compla<strong>in</strong>ts <strong>in</strong> Relation to <strong>Exam<strong>in</strong>ations</strong><br />
• Discrim<strong>in</strong>ation and Harassment<br />
• Tra<strong>in</strong><strong>in</strong>g and Exams - Policies<br />
• Eligibility for Retrospective and Prospective Accreditation of Tra<strong>in</strong><strong>in</strong>g<br />
• Exam Exemption Guidel<strong>in</strong>es 5 March 2007<br />
• Exam<strong>in</strong>ation Candidates <strong>in</strong> Need of Consideration for Illness, Accident, Disability or Compassionate Grounds<br />
• Exam<strong>in</strong>ation Papers on the Website<br />
• Exam<strong>in</strong>ation Venues<br />
• Exam<strong>in</strong>ation Venues July 2001 (94kb)<br />
• Fees Associated with Failure to Attend an Exam<strong>in</strong>ation, Withdrawal from Sitt<strong>in</strong>g Exam<strong>in</strong>ation, Exemption from Exam<strong>in</strong>ation, Repeat Exam<strong>in</strong>ation and Late Applications<br />
• Guidel<strong>in</strong>es for Invigilators – Exam<strong>in</strong>ation Procedure<br />
• Interview of Overseas Tra<strong>in</strong>ed Specialists<br />
• Jo<strong>in</strong>t Tra<strong>in</strong><strong>in</strong>g Programs with the Royal Australasian College of Physicians<br />
• Laboratory Accreditation for Tra<strong>in</strong><strong>in</strong>g Programs<br />
• Limitation on the Number of Exam<strong>in</strong>ation Attempts and Length of Time Exam<strong>in</strong>ation Passes Rema<strong>in</strong> Valid<br />
• Mentor<strong>in</strong>g for Tra<strong>in</strong>ees<br />
• Occupational Tra<strong>in</strong>ees <strong>in</strong> Australia<br />
• Ownership and Confidentiality of Exam<strong>in</strong>ation Materials<br />
10.3.06
Available Information (cont.)<br />
Information for Tra<strong>in</strong>ees, <strong>in</strong>vigiltors and exam<strong>in</strong>ers<br />
• Payment of Fees for Retrospective Accreditation<br />
• Plagiarism and Cheat<strong>in</strong>g <strong>in</strong> <strong>Exam<strong>in</strong>ations</strong><br />
• Repeat <strong>Exam<strong>in</strong>ations</strong><br />
• Retention of Exam<strong>in</strong>ation Materials<br />
• Retra<strong>in</strong><strong>in</strong>g<br />
• Selection of Exam<strong>in</strong>ers for the College<br />
• Selection of Exam<strong>in</strong>ers for the College - October 2001 (92kb)<br />
• Selection of Tra<strong>in</strong>ees<br />
• Supervision of Tra<strong>in</strong><strong>in</strong>g<br />
• Tim<strong>in</strong>g of Part II <strong>Exam<strong>in</strong>ations</strong> <strong>in</strong> <strong>Anatomical</strong> Pathology with Particular Regard to Exemptions and OTS Candidates<br />
• Tra<strong>in</strong><strong>in</strong>g Determ<strong>in</strong>ations, Exam<strong>in</strong>ation Exemptions<br />
• Tra<strong>in</strong><strong>in</strong>g <strong>in</strong> an Unpaid Position<br />
• Tra<strong>in</strong><strong>in</strong>g Limitation<br />
• Tra<strong>in</strong><strong>in</strong>g time credits (Retrospective time)<br />
• Viva <strong>Exam<strong>in</strong>ations</strong><br />
10.3.06
Available Information (cont.)<br />
Tra<strong>in</strong><strong>in</strong>g and Exams - Publications<br />
• A Career <strong>in</strong> Pathology<br />
• AMC Accreditation F<strong>in</strong>al Report<br />
• AMC Accreditation F<strong>in</strong>al Report - appendices<br />
• Draft Induction Manual for Supervisors<br />
• Guide for Supervisors<br />
• <strong>RCPA</strong> Tra<strong>in</strong>ee Handbook<br />
• 2007 Tra<strong>in</strong>ee Handbook 24 September<br />
• Overall Results of Tra<strong>in</strong>ee Survey 2003<br />
• Supervisor's report for Tra<strong>in</strong>ees <strong>in</strong> <strong>Anatomical</strong> Pathology<br />
• Supervisor's report form<br />
10.3.06
Available Information<br />
10.3.06
What’s s Current ?<br />
• Forensic Pathology has its own exam<strong>in</strong>ation system<br />
• No slants at Part ll <strong>Anatomical</strong> <strong>pathology</strong> exam<strong>in</strong>ations<br />
• Proposed <strong>in</strong>troduction of (non mandatory) Diplomas at<br />
Post-Fellowship level to demonstrate advanced<br />
competency <strong>in</strong> selected sub-specialties<br />
specialties<br />
10.3.06
No More Slanted Part II Exams <strong>in</strong><br />
AP – Post Fellowship Diplomas<br />
What’s s it mean ?<br />
Proposed<br />
• If you have not already registered for a Part ll slant then you must<br />
sit the AP Part l and Part ll Exams to proceed to Fellowship<br />
• It is proposed that post-Fellowship Diplomas, such as the Diploma<br />
<strong>in</strong> Cyto<strong>pathology</strong> will also be offered <strong>in</strong> Neuro<strong>pathology</strong>* and<br />
Paediatric Pathology*<br />
‣ May be sat at any regular exam round<br />
‣ Candidates are proposed for Diplomas by 2 Fellows<br />
recognised as specialists <strong>in</strong> the particular area*<br />
*These proposals have still to be formulated, together with a<br />
curriculum, and ratified by the Board of Censors and Council<br />
10.3.06
<strong>Exam<strong>in</strong>ations</strong> <strong>in</strong> <strong>Anatomical</strong> Pathology<br />
CURRENT<br />
EXAMINATION<br />
FORMAT AND<br />
MARKING<br />
PROCEDURES<br />
10.3.06
To avoid confusion (and to also avoid repetitive<br />
questions) – please note the follow<strong>in</strong>g:-<br />
• The time allowed for the first practical exam<strong>in</strong>ations is 4 hours .<br />
• Change of format for mark<strong>in</strong>g practical exam<strong>in</strong>ations - exam<strong>in</strong>ers mark each question<br />
separately. This will avoid previous answers from a candidate hav<strong>in</strong>g any <strong>in</strong>fluence on the<br />
marks for the next case<br />
• Autopsy assessment - the autopsy assessment is a stand alone component attempted any<br />
time after the first 15 months of tra<strong>in</strong><strong>in</strong>g – the assessment must be satisfactorily completed<br />
before the Board of Censors will recommend the conferr<strong>in</strong>g of Fellowship lowship by Council<br />
• Exemptions for any one phase of the Part 1 exam<strong>in</strong>ation are only valid for one year<br />
• Exemptions for any one component of the Part 2 exam<strong>in</strong>ation are ord<strong>in</strong>arily o<br />
only valid to<br />
the next exam<strong>in</strong>ation<br />
10.3.06
<strong>Exam<strong>in</strong>ations</strong> <strong>in</strong> AP<br />
The aims of the current exam<strong>in</strong>ations are: -<br />
Part I<br />
• the ma<strong>in</strong> assessment hurdle with candidates expected<br />
to approach but not reach the standard required for<br />
the Part II<br />
Part II<br />
• more of an ‘exit’ exam<br />
• a cont<strong>in</strong>ued assessment of safe and unsupervised<br />
practice of AP at the specialist level<br />
10.3.06
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
Part I<br />
• One written paper<br />
• One 4 hour histo<strong>pathology</strong> slide exam<strong>in</strong>ation<br />
• Special practical exam<strong>in</strong>ation<br />
• Two 20-m<strong>in</strong>ute<br />
vivas<br />
Part II<br />
• Casebook<br />
• One 4 hour histo<strong>pathology</strong> slide exam<strong>in</strong>ation<br />
• One 2 hour cyto<strong>pathology</strong> exam<strong>in</strong>ation (12 cases)<br />
• Two 20-m<strong>in</strong>ute<br />
vivas<br />
All – Autopsy assessment, 2005 onwards<br />
10.3.06
Part I<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
Phase 1<br />
• One three-hour hour essay-type written paper compris<strong>in</strong>g 5 compulsory questions<br />
• A four-hour practical exam<strong>in</strong>ation of 20 cases consist<strong>in</strong>g entirely of surgical and<br />
autopsy <strong>pathology</strong><br />
Sat at around the same time, <strong>in</strong> regional venues, as at present<br />
Successful candidates will be <strong>in</strong>vited to the Phase 2<br />
10.3.06
Part I<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
Phase 2<br />
• A three-hour hour practical exam<strong>in</strong>ation <strong>in</strong>clud<strong>in</strong>g any of the follow<strong>in</strong>g:-<br />
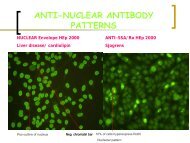
frozen sections, cytology, small biopsies, special sta<strong>in</strong>s,<br />
immunoperoxidase, , immunofluorescence photographs, electron<br />
micrographs and macrophotographs (12 stations)<br />
Sat at the same venue as the oral.<br />
Candidates rotate at regular <strong>in</strong>tervals through a series of stations<br />
• Two 20-m<strong>in</strong>ute oral exam<strong>in</strong>ations<br />
10.3.06
The Written Exam<strong>in</strong>ation<br />
• What do we tell the exam<strong>in</strong>ers?
Sample portions of Letter To<br />
Exam<strong>in</strong>ers – Part l, 2005<br />
Dear Dr,<br />
Thank you for agree<strong>in</strong>g to mark a question <strong>in</strong> the Part I <strong>Anatomical</strong> al Pathology Written<br />
Exam<strong>in</strong>ation. The exam<strong>in</strong>ation will be held Friday 10 June. You have h<br />
been assigned<br />
question 1:<br />
1. A 74-year<br />
year-old male with severe chronic obstructive airways disease<br />
presents with abdom<strong>in</strong>al discomfort and is found on imag<strong>in</strong>g to have a<br />
thicken<strong>in</strong>g <strong>in</strong> his term<strong>in</strong>al ileum and retroperitoneal lymphadenopathy. athy. After<br />
assessment he is found to be a poor risk for general anaesthetic and open<br />
biopsy. The radiologists have been asked to obta<strong>in</strong> material from m his<br />
peritoneal lymph nodes under imag<strong>in</strong>g guidance.<br />
You are called by the radiologist on duty and asked for advice as to the<br />
specimens you would prefer to maximise the chance of reach<strong>in</strong>g a def<strong>in</strong>itive<br />
diagnosis.<br />
State what advice you would give, consider<strong>in</strong>g the possible differential<br />
diagnoses, <strong>in</strong>clud<strong>in</strong>g the reasons for each type of specimen you would w<br />
require.<br />
How would you handle and distribute each of the specimens once they t<br />
are<br />
collected?
Instructions to Exam<strong>in</strong>ers<br />
“ In sett<strong>in</strong>g the paper we have<br />
attempted to move away from<br />
questions requir<strong>in</strong>g only<br />
factual knowledge and have<br />
tried to <strong>in</strong>troduce questions<br />
that require the candidate to<br />
apply that knowledge.”
Some of the po<strong>in</strong>ts we had <strong>in</strong> m<strong>in</strong>d when sett<strong>in</strong>g<br />
question 1 <strong>in</strong>cluded:<br />
• The differential diagnosis to be considered <strong>in</strong>clud<strong>in</strong>g possible<br />
<strong>in</strong>fectious causes (Mycobacterial(<br />
<strong>in</strong>fection, Yers<strong>in</strong>ial <strong>in</strong>fection,<br />
Slamonella etc.), <strong>in</strong>flammatory causes <strong>in</strong>clud<strong>in</strong>g Crohn’s disease)<br />
and neoplastic disorders <strong>in</strong> this situation (lymphoma etc.)<br />
• Specimens to consider request<strong>in</strong>g should <strong>in</strong>clude material for<br />
histopathological exam<strong>in</strong>ation, microbiological exam<strong>in</strong>ation, flow<br />
cytometry and immunohistochemistry<br />
• Discussion of handl<strong>in</strong>g of the specimens should <strong>in</strong>clude OH&S<br />
considerations<br />
• The candidates should be able to give advice as to the limitations of<br />
procedures <strong>in</strong>clud<strong>in</strong>g FNA biopsy and core biopsy techniques
• On receipt of this letter would you please liaise with your co-<br />
exam<strong>in</strong>er re. the required content of the answer for this particular<br />
question – i.e. the m<strong>in</strong>imum <strong>in</strong>formation you consider necessary<br />
for a pass. Between you, you may decide that further <strong>in</strong>formation,<br />
other than that which Tony Thomas and I have mentioned, should<br />
also be <strong>in</strong>cluded. This is acceptable, but please correspond with us<br />
re. any extra <strong>in</strong>formation you th<strong>in</strong>k was necessary, after you have<br />
completed your mark<strong>in</strong>g.<br />
• After you have agreed on the content would you please mark the<br />
papers <strong>in</strong>dependently and keep a record of your orig<strong>in</strong>al<br />
assessment to forward to us, together with an agreed assessment<br />
<strong>in</strong> the case of any major discrepancies. If there are major<br />
unresolved discrepancies a review of the candidate's paper by a<br />
third exam<strong>in</strong>er may be necessary. We are request<strong>in</strong>g that you<br />
follow this procedure to fall <strong>in</strong> l<strong>in</strong>e with suggestions from the<br />
curriculum review and assessment outcomes thus far.
Question 2<br />
Write short notes on three of the follow<strong>in</strong>g:<br />
The use of micro-arrays <strong>in</strong> def<strong>in</strong><strong>in</strong>g tumour differentiation<br />
Implications of a diagnosis of serrated adenoma<br />
Flow cytometry and gene re-arrangement studies <strong>in</strong> the diagnosis of<br />
cutaneous lymphomas<br />
Micro-satellite <strong>in</strong>stability <strong>in</strong> large bowel adenocarc<strong>in</strong>omas<br />
Electron microscopy <strong>in</strong> the diagnosis of soft tissue tumours
Question 3<br />
You are directed by the Coroner to perform an autopsy on the body y of<br />
a 38-year<br />
year-old male who has died follow<strong>in</strong>g perforation of the<br />
oesophagus, followed by suppurative mediast<strong>in</strong>itis and septicaemia.<br />
a.<br />
Endoscopy four days prior to death showed an oesophageal ulcer and a<br />
biopsy revealed herpes virus <strong>in</strong>clusions <strong>in</strong> the squamous epithelium<br />
adjacent to the ulcer and fungal elements, presumed to be Candida<br />
sp., <strong>in</strong> the ulcer slough.<br />
Describe your approach to the autopsy under the follow<strong>in</strong>g head<strong>in</strong>gs:<br />
-<br />
Possible differential diagnoses as to any underly<strong>in</strong>g disease process you<br />
might expect to encounter;<br />
Occupational health and safety issues;<br />
Macroscopic exam<strong>in</strong>ation;<br />
Specimen collection and exam<strong>in</strong>ation:<br />
Potential microscopic f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> exam<strong>in</strong>ation of lymph nodes.
Some of the po<strong>in</strong>ts we had <strong>in</strong> m<strong>in</strong>d<br />
when sett<strong>in</strong>g question 3 <strong>in</strong>cluded:<br />
• Differential should <strong>in</strong>clude the range of conditions which might<br />
cause immunosuppression <strong>in</strong> this age group<br />
• Occupational health and safety Issues should <strong>in</strong>clude universal and a<br />
any special precautions for deal<strong>in</strong>g with possible <strong>in</strong>fectious material<br />
<strong>in</strong> the autopsy situation and <strong>in</strong> the handl<strong>in</strong>g of collected specimens<br />
ens<br />
• The macroscopic and microscopic exam<strong>in</strong>ations should <strong>in</strong>clude<br />
evidence of exam<strong>in</strong>ation for possible factors related to acquisition ion of<br />
acquired immune deficiency and also related <strong>pathology</strong>, <strong>in</strong>clud<strong>in</strong>g<br />
<strong>in</strong>fections. The possibility that the perforation is iatrogenic should s<br />
also be addressed<br />
• Lymph node exam<strong>in</strong>ation should <strong>in</strong>clude features seen <strong>in</strong> HIV<br />
<strong>in</strong>fection/AIDS and also other conditions <strong>in</strong> which immune<br />
compromise might be seen, <strong>in</strong>clud<strong>in</strong>g previously undiagnosed<br />
lymphoma etc.
Part II - Casebook<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
From 2005:<br />
Only eight cases are required as outl<strong>in</strong>ed <strong>in</strong> the<br />
tra<strong>in</strong>ee handbook. (under review)<br />
**Please check the requirements as outl<strong>in</strong>ed <strong>in</strong> the Tra<strong>in</strong>ee Handbook**<br />
10.3.06
Part II - Casebook<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
• At least two cases must have been handled dur<strong>in</strong>g the 12 months<br />
immediately preced<strong>in</strong>g the deadl<strong>in</strong>e for submission on 31st March <strong>in</strong> the<br />
year of the exam<strong>in</strong>ation<br />
• Cases must be handled personally by the candidate as part of his or her<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> the discipl<strong>in</strong>e<br />
• Cases cannot be used <strong>in</strong> any other casebook at any time or by any other<br />
candidate<br />
• Individual case reports <strong>in</strong> peer-reviewed reviewed journals, and paper or poster<br />
presentations dur<strong>in</strong>g the period of tra<strong>in</strong><strong>in</strong>g and for which the candidate is<br />
either the pr<strong>in</strong>cipal author or has had a significant <strong>in</strong>put are acceptable; a<br />
a<br />
copy should be <strong>in</strong>cluded with the casebook<br />
10.3.06
Part II - Casebook<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
The aims of the casebook are to achieve: -<br />
• Content as set out <strong>in</strong> the Tra<strong>in</strong>ees’ handbook<br />
• A succ<strong>in</strong>ct presentation of no more than 10 pages with the discussion<br />
sion<br />
at least twice as long as the rema<strong>in</strong>der of the presentation with<br />
• A bibliography <strong>in</strong> the order of 15 to 30 references and <strong>in</strong>clud<strong>in</strong>g<br />
recent peer-reviewed reviewed literature<br />
• Should <strong>in</strong>clude a comprehensive and critical appraisal of the cited<br />
literature<br />
and<br />
• High quality photomicrographs/illustrations<br />
The volume should be bound (spirax(<br />
b<strong>in</strong>d<strong>in</strong>g OK) and submitted <strong>in</strong><br />
duplicate<br />
10.3.06
Part II - Casebook<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
Casebooks are assessed simply as:<br />
☺Satisfactory<br />
Unsatisfactory - revise and resubmit the same year<br />
Resubmission by 31st October for consideration and<br />
recommendation to BoC November meet<strong>in</strong>g; otherwise<br />
by 31st March the follow<strong>in</strong>g year<br />
Exam is <strong>in</strong>complete until a pass grade is obta<strong>in</strong>ed<br />
PROPOSED CHANGE - It is proposed that Candidates not meet<strong>in</strong>g the<br />
31st March deadl<strong>in</strong>e will be permitted to sit the Part 2 exam<strong>in</strong>ation ion <strong>in</strong><br />
the same year, but we will not guarantee your results will be ready by<br />
the end of the August exam cycle<br />
New cases will be necessary if not passed <strong>in</strong> the same year<br />
10.3.06
Part II - Practical<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
• Include not only the recognition of commonplace and classical<br />
uncommon disorders, but also cases where the diagnosis may<br />
not be straightforward, and for which there may be no def<strong>in</strong>ite<br />
answer<br />
• Emphasis is now be placed on rational and scientific approach<br />
to differential diagnosis as part of problem-solv<strong>in</strong>g <strong>in</strong> AP<br />
• Consequently the number of cases is less than <strong>in</strong> the Part 1<br />
• The cases may <strong>in</strong>clude surgical and autopsy <strong>pathology</strong><br />
• Sat <strong>in</strong> regional venues<br />
• The oral exam rema<strong>in</strong>s unchanged and comprises two<br />
20-m<strong>in</strong>ute<br />
vivas<br />
10.3.06
Part II - Cyto<strong>pathology</strong> Practical<br />
Current Exam<strong>in</strong>ation Format <strong>in</strong> AP<br />
12 cases to be completed <strong>in</strong> a 2 hour period<br />
Cases may <strong>in</strong>clude: -<br />
• Gynaecological (Pap.) cytology<br />
• FNA Cytology<br />
• Body fluid cytology<br />
• Exfoliative cytology<br />
• Sputum, ur<strong>in</strong>e etc.<br />
10.3.06
Part I and Part II practical<br />
exam<strong>in</strong>ations <strong>in</strong> AP<br />
• Cases are submitted by senior consultants from<br />
Departments around Australia, New Zealand,<br />
S<strong>in</strong>gapore, Malayasia and Hong Kong<br />
• The practicals are designed to encompass a broad<br />
range of neoplastic and non-neoplastic<br />
neoplastic disorders<br />
• The suitability of material for each exam<strong>in</strong>ation is<br />
assessed by a panel of senior consultants who are<br />
experienced exam<strong>in</strong>ers<br />
10.3.06
Mark<strong>in</strong>g of the Part I and Part II practical<br />
exam<strong>in</strong>ations <strong>in</strong> AP<br />
• Candidates’ answer books are identified by candidate number<br />
only and rema<strong>in</strong> anonymous to <strong>in</strong>dividual exam<strong>in</strong>ers<br />
• An overall fail grade is usually the result of a number of errors.<br />
This may <strong>in</strong>clude too many misdiagnoses or a lesser number that<br />
are considered by the exam<strong>in</strong>ers to be ‘serious’ <strong>in</strong> the sense that<br />
misdiagnosis could impact adversely on patient management -<br />
NEVER BASED ON ONE CASE!<br />
• Candidates and supervisors should be reassured that the<br />
evaluation process is <strong>in</strong>tended to be fair and impartial with<br />
crosschecks and balances at each phase of the assessment<br />
10.3.06
Mark<strong>in</strong>g of the Part I and Part II practical<br />
exam<strong>in</strong>ations <strong>in</strong> AP<br />
1st Exam<strong>in</strong>er<br />
Pass<br />
2nd Exam<strong>in</strong>er<br />
3rd Exam<strong>in</strong>er<br />
Fail<br />
Progress to<br />
orals/2nd phase<br />
Borderl<strong>in</strong>e/<br />
Discrepancies<br />
No progression to<br />
orals/2nd phase<br />
Pass<br />
Pass<br />
4th Exam<strong>in</strong>er<br />
Borderl<strong>in</strong>e<br />
Reviewed<br />
Fail<br />
Fail<br />
Borderl<strong>in</strong>e<br />
10.3.06
The Autopsy Assessment <strong>in</strong> AP<br />
• This assessment can be undertaken any time after 15<br />
months of tra<strong>in</strong><strong>in</strong>g and before award<strong>in</strong>g Fellowship<br />
• The assessment is a “stand alone” component <strong>in</strong> the<br />
overall assessment for qualification for Fellowship of<br />
the College <strong>in</strong> AP<br />
• The current guidel<strong>in</strong>es and assessment form are as<br />
follows:-<br />
10.3.06
The Autopsy Assessment <strong>in</strong> AP<br />
• Two assessors required to substantiate competence <strong>in</strong> this area of assessment<br />
• Each assessor must <strong>in</strong>dependently complete a copy of the assessment form.<br />
A third comb<strong>in</strong>ed and agreed assessment should also be submitted.<br />
• A depersonalised copy of the autopsy report must be forwarded, together t<br />
with the completed assessment sheets to the College office.<br />
• The autopsy must be assessed by : -<br />
– Departmental Autopsy Service supervisor<br />
and one of the follow<strong>in</strong>g<br />
– <strong>RCPA</strong> Fellow (<strong>in</strong> AP or GP) (external to department) – preferred<br />
– <strong>RCPA</strong> Fellow (<strong>in</strong> AP or GP) other than the autopsy supervisor<br />
– Cl<strong>in</strong>ician <strong>in</strong>volved <strong>in</strong> the case<br />
• The whole of the autopsy need not be observed by the assessors but b<br />
both<br />
assessors must be present at the <strong>in</strong>troductory discussion, the demonstration<br />
of f<strong>in</strong>d<strong>in</strong>gs and assessment of key organ dissection.<br />
• The requirements for assessment are available on the <strong>RCPA</strong> web site <strong>in</strong> the<br />
form of an assessor’s s sheet<br />
10.3.06
Feedback on the performance and<br />
<strong>in</strong>terpretation of the autopsy f<strong>in</strong>d<strong>in</strong>gs<br />
and the proposed recommendations<br />
of the assessors should be discussed<br />
with the candidate at the completion<br />
of the autopsy report<br />
10.3.06
<strong>Exam<strong>in</strong>ations</strong> <strong>in</strong> <strong>Anatomical</strong> Pathology<br />
QUESTIONS AND<br />
COMMENTS FOR<br />
DISCUSSION<br />
10.3.06
“Markers should be selected from a variety of<br />
departments and practices to reflect the diversity of<br />
pathological practice”<br />
They are:<br />
• At the end of the day, it is the content of the<br />
report and not the style which is of<br />
fundamental importance and it is this which<br />
forms the basis of a pass grade<br />
10.3.06
“Mark<strong>in</strong>g of essays is spread across Australia and argument<br />
that the slides are marked differently to expedite the process is i<br />
difficult to reconcile consider<strong>in</strong>g the time it takes to get results<br />
lts”<br />
• S<strong>in</strong>ce 1999, some borderl<strong>in</strong>e papers have been assessed by<br />
up to 5 different exam<strong>in</strong>ers <strong>in</strong> three different states and<br />
further reviewed by the Chief Exam<strong>in</strong>ers: this comment is<br />
not justified<br />
• The current system gives the candidate the best possible<br />
chance of progress<strong>in</strong>g to the vivas and it is not appropriate<br />
to expedite results at the expense of candidates<br />
• It is not practicable or desirable to have 20 answers books<br />
per candidate and up to 20 different markers, or to have<br />
only a few candidates assessed by different exam<strong>in</strong>ers<br />
10.3.06
“If it is essential to keep the slide mark<strong>in</strong>g to one<br />
city why not rotate the city responsible annually?”<br />
• The Chief and Associate Chief Exam<strong>in</strong>ers are<br />
answerable to the Board of Censors and must be<br />
responsible for ensur<strong>in</strong>g the ma<strong>in</strong>tenance of standards,<br />
impartiality and cont<strong>in</strong>uity from year to year<br />
• To annually rotate from city to city without the<br />
<strong>in</strong>volvement of the Chief Exam<strong>in</strong>ers would result <strong>in</strong><br />
variation of standards and possible loss of anonymity<br />
• cf. UK system where standards have <strong>in</strong> the past been<br />
vastly different from centre to centre.<br />
10.3.06
“What are the criteria for allow<strong>in</strong>g candidates to be<br />
assessed on extra slides at the viva?”<br />
This applies to the Part II only !<br />
• Candidates obta<strong>in</strong><strong>in</strong>g a borderl<strong>in</strong>e grade for the practical will be b<br />
required to report on extra slides at the time of the vivas<br />
• Candidates who fail the practical for the third time but who have<br />
achieved a pass grade or borderl<strong>in</strong>e result on a previous occasion,<br />
and whose <strong>in</strong>correct answers on this last occasion do not exceed<br />
one third of the cases may be <strong>in</strong>vited to report on extra slides at<br />
the vivas<br />
• Reduc<strong>in</strong>g the number of slides from 20 to 15 has led to a number<br />
of candidates who cannot be assessed as pass or fail despite hav<strong>in</strong>g<br />
their papers marked by up to 5 exam<strong>in</strong>ers. These candidates are<br />
<strong>in</strong>vited to report on extra slides at the vivas<br />
10.3.06
“A A recurr<strong>in</strong>g problem has been the general uncerta<strong>in</strong>ty<br />
about what is required <strong>in</strong> terms of the content and structure<br />
of a Pass answer.”<br />
• Perhaps the best guide, other than common<br />
sense, may be found by view<strong>in</strong>g previous<br />
Tra<strong>in</strong>ee Update Presentations, especially the<br />
“<strong>in</strong>teractive” presentation from 2004.<br />
• This is available from the College Office<br />
10.3.06
“Sample answers and publication of answers to the<br />
slides would be helpful to both fail and pass candidates”<br />
• In the next part of this presentation we will<br />
consider cases from the 2007 Part ll first<br />
practical exam<strong>in</strong>ation<br />
• We will show comments and/or answers on<br />
cases to give you an idea of what is expected<br />
10.3.06
Indication as to what is required for slide<br />
report<strong>in</strong>g <strong>in</strong> the practical exam<strong>in</strong>ations<br />
• Instructions to candidates are now issued with the<br />
acceptance letter for exam<strong>in</strong>ation <strong>in</strong> addition to those<br />
provided at the time of the exam (Instructions to<br />
Candidates for the Special Part I practical are issued<br />
with <strong>in</strong>vitation to participate <strong>in</strong> the vivas):<br />
– “The aim of this practical is to evaluate your ability<br />
as a pathologist to diagnose “a a slide” that is<br />
representative of a particular lesion(s) and, for Part<br />
II, to practice safe and unsupervised microscopy <strong>in</strong><br />
AP at a specialist standard”<br />
10.3.06
Indication as to what is required for slide<br />
report<strong>in</strong>g <strong>in</strong> the practical exam<strong>in</strong>ations<br />
– “It is <strong>in</strong> your <strong>in</strong>terest not to waste time on overly long<br />
histological descriptions. You should describe the<br />
features (succ<strong>in</strong>ctly) and state how you would reach the<br />
appropriate diagnosis (if this is not obvious to you)<br />
– “For Part I, most cases represent examples of important<br />
and common diseases and classical less common<br />
disorders”<br />
– “For Part II, the cases <strong>in</strong>clude some that are<br />
straightforward and for which a def<strong>in</strong>itive diagnosis can<br />
be made whilst others are more complex and for which<br />
there may be no straightforward answer. Here, the<br />
exam<strong>in</strong>ers seek to assess the capacity for an analytical<br />
and cl<strong>in</strong>icopathological approach”<br />
10.3.06
Indication as to what is required for slide<br />
report<strong>in</strong>g <strong>in</strong> the practical exam<strong>in</strong>ations<br />
– “Report on each case along the l<strong>in</strong>es you would use <strong>in</strong><br />
everyday practice, <strong>in</strong>clud<strong>in</strong>g a brief microscopic<br />
description of each slide. Whenever possible, identify<br />
the organ or tissue and emphasise any features you<br />
would need to highlight <strong>in</strong> your report to the referr<strong>in</strong>g<br />
cl<strong>in</strong>ician”<br />
– “If you are unsure as to the diagnosis, a differential<br />
diagnosis should be given and the means by which you<br />
arrive at your preferred diagnosis <strong>in</strong>dicated”<br />
– “Differential diagnoses should be discrim<strong>in</strong>at<strong>in</strong>g ,<br />
reflect your microscopic description and should show<br />
discernment of the issues illustrated <strong>in</strong> the sections”<br />
10.3.06
Indication as to what is required for slide<br />
report<strong>in</strong>g <strong>in</strong> the practical exam<strong>in</strong>ations<br />
Do not simply give a non-discrim<strong>in</strong>at<strong>in</strong>g list of all<br />
potential differential diagnoses<br />
Do not simply give a list of potential special sta<strong>in</strong>s and/or<br />
immunoperoxidase studies without justification and an<br />
<strong>in</strong>dication of the expected outcome<br />
Do not ‘second guess’ the exam<strong>in</strong>ers<br />
Write and <strong>in</strong>dicate your preferred diagnosis clearly at the<br />
end of your report<br />
10.3.06
1“Are slides weighted?’<br />
2“Are there sudden death slides?”<br />
1 Yes, to a degree<br />
An error which would have led to unnecessary<br />
amputation is considered more serious than one which<br />
would not have affected the patient and this may be<br />
taken <strong>in</strong>to account <strong>in</strong> overall performance<br />
2 No<br />
There have been no ‘sudden death’ slides dur<strong>in</strong>g the<br />
term of office of the last two Chief Exam<strong>in</strong>ers and there<br />
will be none dur<strong>in</strong>g the current Chief Exam<strong>in</strong>er’s s term<br />
of office.<br />
10.3.06
Practical <strong>Exam<strong>in</strong>ations</strong><br />
What are the exam<strong>in</strong>ers told ?
This is the overall format of the letter of<br />
Instructions sent to the practical exam<strong>in</strong>ers<br />
• Chief Exam<strong>in</strong>er <strong>in</strong> <strong>Anatomical</strong> Pathology Telephone: (03) 92884551<br />
• Richard A Williams, MB BS, PhD, F<strong>RCPA</strong>, FHKCPath. International: 613 92884551<br />
• Department of <strong>Anatomical</strong> Pathology Fax: (03) 9288 4580<br />
• St. V<strong>in</strong>cent’s Pathology. 41 Victoria Pde.,<br />
International: 613 9288 4580<br />
• Fitzroy, Vic. 3065<br />
email: williara@svhm.org.au<br />
•<br />
•<br />
Date<br />
• Dr<br />
• Department of <strong>Anatomical</strong> Pathology<br />
• Ground Floor<br />
• Dear ,<br />
• Re: <strong>RCPA</strong> Part II Practical <strong>Exam<strong>in</strong>ations</strong> <strong>in</strong> <strong>Anatomical</strong> Pathology<br />
• Once aga<strong>in</strong>, many thanks for agree<strong>in</strong>g to mark the slides for the Part II practical exam<strong>in</strong>ation held on Saturday 29th May.<br />
• Please f<strong>in</strong>d enclosed x sets of answers for y Candidates, a set of slides with accompany<strong>in</strong>g exam<strong>in</strong>ation question sheet and <strong>in</strong>structions<br />
to candidates and mark<strong>in</strong>g sheets.<br />
to candidates and mark<strong>in</strong>g sheets. I have attached a set of the case histories, together with an op<strong>in</strong>ion<br />
(“diagnosis”)) for each case. Please feel free to disagree and assess accord<strong>in</strong>gly.<br />
• We have made one change to the way the papers are to be marked this t<br />
year, <strong>in</strong> l<strong>in</strong>e with advice and recommendations from the<br />
curriculum review/assessment educational experts. We would ask that t<br />
the cases be marked “horizontally” rather than “vertically” this<br />
year. To this end we are forward<strong>in</strong>g the answer sheets bundled by question, rather than by candidate book – i.e. all slide 1 answers are<br />
bundled together and should be marked as a s<strong>in</strong>gle group, before cont<strong>in</strong>u<strong>in</strong>g to all of the slide 2 answers, etc. For each question/slide I<br />
have <strong>in</strong>cluded a sheet for prelim<strong>in</strong>ary marks but also <strong>in</strong>clude the standard collation mark sheet for each <strong>in</strong>dividual candidate. Once all the<br />
mark<strong>in</strong>g has been completed, it may be easier to have your secretarial staff transfer the <strong>in</strong>dividual case marks and comments from the<br />
‘horizontal’ prelim<strong>in</strong>ary mark sheets to the standard (‘vertical(<br />
vertical’) ) <strong>in</strong>dividual candidate’s s f<strong>in</strong>al mark sheet. The College has agreed to<br />
reimburse your Department for this extra work time on receipt of an <strong>in</strong>voice.
letter of Instructions (cont.)<br />
As <strong>in</strong> the past we would ask you to mark each slide as ‘right’, ‘wrong’ or ‘borderl<strong>in</strong>e’ and once all the<br />
mark<strong>in</strong>g is completed, consider the overall number of slides ‘wrong’ or ‘borderl<strong>in</strong>e’ and the<br />
seriousness of errors <strong>in</strong> assess<strong>in</strong>g whether an <strong>in</strong>dividual candidate has passed or failed. For the Part II we<br />
• As <strong>in</strong> the past<br />
have worked on over 3 ‘wrong’ answers (equivalent to over 20% wrong answers), or over 2 ‘wrong’ and 2 ‘borderl<strong>in</strong>e’ answers to be a fail grade depend<strong>in</strong>g on the<br />
seriousness of the errors. Although some weight<strong>in</strong>g is given to the t<br />
seriousness of an error, we have not adopted the policy of a s<strong>in</strong>gle 'sudden death slide'.<br />
Normally, for those cases where a differential diagnosis can be justified, provided the candidate has<br />
given an appropriate description and differential diagnosis, and can demonstrate that he/she would<br />
have arrived at the correct diagnosis through appropriate ancillary ary techniques, we would consider<br />
that answer to be at least ‘borderl<strong>in</strong>e’ if not ‘right’ even if the preferred diagnosis is wrong.<br />
• If appropriate, could you please make brief comments <strong>in</strong> the column provided for each case. This helps <strong>in</strong> formulat<strong>in</strong>g assessment reports and allows me to review<br />
<strong>in</strong>dividual slide box numbers <strong>in</strong> the event of discrepancies. F<strong>in</strong>ally, for each candidate, could you give an overall op<strong>in</strong>ion as to ‘pass’, ‘fail’ or ‘borderl<strong>in</strong>e’ based on the<br />
above criteria.<br />
• I hope I have not totally confused you as to the approach – much of it is commonsense although there are always those candidates dates that are ‘borderl<strong>in</strong>e’ no matter which<br />
way one assesses them. Could you also make a recommendation for those borderl<strong>in</strong>e candidates who you th<strong>in</strong>k may be taken onto the orals and shown extra slides at<br />
that time.<br />
• This year we have given an undertak<strong>in</strong>g to have the results published by the end of July and have not bowed to the pressure of publish<strong>in</strong>g same earlier because of the<br />
<strong>in</strong>crease <strong>in</strong> the number of candidates present<strong>in</strong>g this year, however er we would appreciate the results back <strong>in</strong> time for Tony and myself to review any discrepancies and<br />
have the scripts re-marked if necessary. Thus it would be appreciated if the mark<strong>in</strong>g g could be completed as soon as possible to enable the scripts to be sent to further<br />
exam<strong>in</strong>ers as required.<br />
• Could you please return the mark sheets to us by courier as soon as possible at the follow<strong>in</strong>g address:-<br />
• Chief Exam<strong>in</strong>ers <strong>in</strong> <strong>Anatomical</strong> Pathology Telephone: (08) 8204 4259<br />
• C/- Anthony C Thomas, MB BS, PhD, FRCPath, F<strong>RCPA</strong> International: 618 8204 4259<br />
• Department of <strong>Anatomical</strong> Pathology Fax: (08) 8374 1437<br />
• Fl<strong>in</strong>ders Medical Centre International: 618 8374 1437<br />
• Bedford Park, SA 5042<br />
email:Tony.Thomas@fl<strong>in</strong>ders.edu.au<br />
Tony.Thomas@fl<strong>in</strong>ders.edu.au<br />
• Thank you once aga<strong>in</strong> for undertak<strong>in</strong>g this task.<br />
• Best wishes,<br />
• Richard Williams<br />
• Chief Exam<strong>in</strong>er <strong>in</strong> <strong>Anatomical</strong> Pathology.
Part 2 Practical
Before we Start on the Part ll Cases<br />
• Don’t t second guess the exam<strong>in</strong>ers:-
Analytical Assessment of Cases<br />
• Don’t t try and diagnose “<strong>in</strong>tuitively”<br />
• Become an “analytical” diagnostician
Case 1: Female 36 – suspicious<br />
lesion on mammography
Case 1: Female 36 – suspicious<br />
lesion on mammography<br />
• MICROSCOPIC<br />
• The breast tissue conta<strong>in</strong>s a well circumscribed <strong>in</strong>vasive tumour. There is one component of the tumour where<br />
the cells are arranged <strong>in</strong> large nests separated by fibrous bands. . With<strong>in</strong> the cell nests there is a predom<strong>in</strong>ance of<br />
small basaloid cells many of which surround aggregates of eos<strong>in</strong>ophilic homogeneous material. There are also<br />
true lumens present l<strong>in</strong>ed by cells with more abundant eos<strong>in</strong>ophilic ic cytoplasm. Surround<strong>in</strong>g this area of nested<br />
tumour there are <strong>in</strong>filtrat<strong>in</strong>g small tubules, nests and trabeculae e of tumour cells. Aga<strong>in</strong> these consists of both<br />
basaloid cells and cells with more abundant eos<strong>in</strong>ophilic cytoplasm surround<strong>in</strong>g true lumens.<br />
• Comment<br />
• The presence of small basaloid cells associated with more epithelial appear<strong>in</strong>g cells and aggregates of eos<strong>in</strong>ophilic<br />
material <strong>in</strong>dicates an adenoid cystic carc<strong>in</strong>oma. The differential l diagnosis <strong>in</strong>cludes an <strong>in</strong>filtrat<strong>in</strong>g cribriform<br />
carc<strong>in</strong>oma and <strong>in</strong> places the clear<strong>in</strong>g around some of the <strong>in</strong>filtrat<strong>in</strong>g t<strong>in</strong>g nests raises the possibility of a micropapillary<br />
carc<strong>in</strong>oma.<br />
• Investigations<br />
• Alcian blue, , PAS, immunoperoxidase sta<strong>in</strong>s for oestrogen and progestagen receptors<br />
• The eos<strong>in</strong>ophilic material present should show positive sta<strong>in</strong><strong>in</strong>g with Alcian blue and be negative for PAS with the<br />
true glandular lum<strong>in</strong>a show<strong>in</strong>g positive sta<strong>in</strong><strong>in</strong>g with PAS. Immunoperoxidase sta<strong>in</strong>s for oestrogen and<br />
progestagen receptors should be negative <strong>in</strong> adenoid cystic carc<strong>in</strong>oma with positive p<br />
sta<strong>in</strong><strong>in</strong>g <strong>in</strong> an <strong>in</strong>filtrat<strong>in</strong>g<br />
cribriform carc<strong>in</strong>oma and frequent positive sta<strong>in</strong><strong>in</strong>g <strong>in</strong> a micropapillary carc<strong>in</strong>oma.<br />
• SUMMARY/ Preferred diagnosis<br />
• Breast: Adenoid cystic carc<strong>in</strong>oma
Heart: Giant cell myocarditis
Case 3: Male 19 – cystic lesion <strong>in</strong><br />
the right humeral head
Case 3: Male 19 – cystic lesion <strong>in</strong><br />
the right humeral head<br />
• MICROSCOPIC<br />
• The biopsy consists of fragments of the tumour with focal peripheral eral reactive sclerosis and new<br />
bone formation. The tumour has a population of mononuclear cells s with admixed mult<strong>in</strong>ucleated<br />
giant cells. The mononuclear cells form sheets, have a moderate amount of eos<strong>in</strong>ophilic<br />
cytoplasm and slightly elongated nuclei with longitud<strong>in</strong>al grooves. There are fragments of tissue<br />
show<strong>in</strong>g the cells with<strong>in</strong> a chondroid matrix. The chondroid matrix has a slightly more<br />
eos<strong>in</strong>ophilic hue than normal cartilage. Focal calcification is occurr<strong>in</strong>g with<strong>in</strong> the chondroid<br />
matrix. There is also area of fibrosis with haemosider<strong>in</strong> conta<strong>in</strong><strong>in</strong>g macrophages and prom<strong>in</strong>ent<br />
th<strong>in</strong> walled vascular spaces that raise the possibility of previous trauma.<br />
• Comment<br />
• This histologic appearance favours the diagnosis of chondroblastoma.. oma.. The differential diagnosis<br />
based on the histology alone would <strong>in</strong>clude a giant cell tumour of bone, a chondromyxoid fibroma<br />
and an osteosarcoma.<br />
• Radiological assessment is essential with a bone tumour. Both giant g<br />
cell tumours and<br />
chondroblastomas occur at the epiphysis (the epiphyseal plate is open with chondroblastoma and<br />
is closed <strong>in</strong> giant cell tumour) and the chondromyxoid fibroma <strong>in</strong>volves the metaphysis.<br />
Histologically the chondromyxoid fibroma also appears more myxoid. The giant cell tumour has<br />
mononuclear cells that lack the nuclear grooves and do not show reactive sclerosis at the<br />
periphery. An osteosarcoma will have pleomorphic cells <strong>in</strong> a sheetlike pattern that permeate the<br />
surround<strong>in</strong>g bone trabeculae.<br />
• SUMMARY<br />
• Right humeral head: Chondroblastoma
Case 4: Female 42 – right thyroid<br />
nodule
Case 4: Female 42 – right thyroid<br />
nodule<br />
• MICROSCOPIC<br />
• The thyroid conta<strong>in</strong>s an encapsulated follicular nodule. The follicular licular structures vary <strong>in</strong> size and<br />
there appears to be central cystic degeneration with<strong>in</strong> the nodule. The cells are predom<strong>in</strong>antly<br />
low cuboidal with round nuclei conta<strong>in</strong><strong>in</strong>g small <strong>in</strong>conspicuous nucleoli. Nuclear crowd<strong>in</strong>g and<br />
overlapp<strong>in</strong>g are not prom<strong>in</strong>ent. Nuclear clear<strong>in</strong>g and nuclear grooves oves are not evident. Golden<br />
brown pigment is present <strong>in</strong> some of the follicular epithelial cells. The fibrous capsule varies <strong>in</strong><br />
thickness and <strong>in</strong> one area there is extension of follicular structures tures <strong>in</strong>to the capsule but not<br />
beyond. However <strong>in</strong> another area there is a f<strong>in</strong>ger-like projections of thyroid follicles which<br />
extends beyond the contours of the capsule <strong>in</strong>to the surround<strong>in</strong>g thyroid. There still appears to<br />
be a small rim of fibrous tissue surround<strong>in</strong>g this extension. However the appearance is consistent<br />
with capsular <strong>in</strong>vasion. Vascular <strong>in</strong>vasion is unable to be identified.<br />
ified.<br />
• Comment<br />
• The presence of capsular <strong>in</strong>vasion <strong>in</strong>dicates that this is a m<strong>in</strong>imally <strong>in</strong>vasive follicular carc<strong>in</strong>oma.<br />
Exam<strong>in</strong>ation of the rema<strong>in</strong><strong>in</strong>g capsule of the follicular nodule and d further levels of the area of<br />
capsular <strong>in</strong>vasion will be exam<strong>in</strong>ed to determ<strong>in</strong>e if there is more extensive <strong>in</strong>vasion <strong>in</strong>to the<br />
surround<strong>in</strong>g thyroid gland.<br />
• SUMMARY<br />
• Thyroid: M<strong>in</strong>imally <strong>in</strong>vasive follicular carc<strong>in</strong>oma.
Case 5: Male 38 – right<br />
retroperitoneal mass
Case 5: Male 38 – right<br />
retroperitoneal mass<br />
• MICROSCOPIC<br />
• The section shows predom<strong>in</strong>antly adipose tissue with mild variation <strong>in</strong> the size of the<br />
adipocytes. . In places there is a suggestion of <strong>in</strong>creased <strong>in</strong>terstitial tissue sue compris<strong>in</strong>g<br />
sp<strong>in</strong>dle cells between the adipocytes. . In other areas there are <strong>in</strong>terlac<strong>in</strong>g bundles of<br />
sp<strong>in</strong>dle cells. The sp<strong>in</strong>dle cells appear to show a degree of cytoplasmic vacuolation.<br />
Thick walled vessels are not prom<strong>in</strong>ent however there is a background of small<br />
capillaries and larger th<strong>in</strong> walled vessels.<br />
• Comment<br />
• The comb<strong>in</strong>ation of fat, smooth muscle and slightly abnormal vessels els <strong>in</strong>dicates an<br />
angiomyolipoma. Immunoperoxidase sta<strong>in</strong>s for S100 and HMB45 as well as muscle<br />
specific act<strong>in</strong> would help confirm this diagnosis as these lesions s show positive sta<strong>in</strong><strong>in</strong>g<br />
for HMB45 and to a lesser degree S100. The smooth muscle shows positive sta<strong>in</strong><strong>in</strong>g<br />
<strong>in</strong>g<br />
for muscle specific act<strong>in</strong>. This lesion may be seen <strong>in</strong> patients with tuberous sclerosis<br />
and cl<strong>in</strong>ical correlation is required<br />
• SUMMARY<br />
• Right retroperitoneal mass: Angiomyolipoma
Case 6:Female 29 – persistent<br />
bleed<strong>in</strong>g post partum
Case 6:Female 29 – persistent<br />
bleed<strong>in</strong>g post partum<br />
• MICROSCOPIC<br />
• The curett<strong>in</strong>gs consist of decidua and immature<br />
chorionic villi. Some of the villi show oedema of<br />
the stroma. Fetal blood vessels can be identified<br />
with<strong>in</strong> the villi. There is no evidence of cistern<br />
formation, excessive trophoblastic proliferation<br />
or a dual population of villi. There is no evidence<br />
of gestational trophoblastic disease.<br />
• SUMMARY<br />
• Uter<strong>in</strong>e curett<strong>in</strong>gs: Products of conception<br />
confirmed.
Case 7: Male 68 – left scrotal mass
Case 7: Male 68 – left scrotal mass<br />
• MICROSCOPIC<br />
• There is atrophic testis with sclerosed tubules, rete testis and paratesticular soft tissue with an<br />
<strong>in</strong>filtrate which consist predom<strong>in</strong>antly of atypical lymphoid cells s and also <strong>in</strong>cludes occasional<br />
eos<strong>in</strong>ophils. With<strong>in</strong> the soft tissue the <strong>in</strong>filtrate is associated d with fat necrosis and vessels with<br />
prom<strong>in</strong>ent endothelial cells. The cells appear to be of medium size s<br />
and <strong>in</strong> many cells the nuclei<br />
appear slightly convoluted.<br />
• Comment: The <strong>in</strong>filtrate appears to be composed of atypical lymphoid cells s consistent with a<br />
lymphoma. The occasional eos<strong>in</strong>ophils, the nuclear morphology and d the prom<strong>in</strong>ent endothelial<br />
cells raise the possibility a T-cell T<br />
lymphoma however flow cytometry and immunohistochemistry is<br />
required for further categorisation.<br />
• Investigations<br />
• Check past history of patient<br />
• Check to see if tissue was sent for flow cytometry.<br />
• Immunoperoxidase sta<strong>in</strong>s; CD20, CD79a for B l<strong>in</strong>age, CD3, CD43 for T l<strong>in</strong>age also Bcl2, BcL6,<br />
CD5, CD10, CD30. If just CD43 positive also do MPO to assess for myeloid l<strong>in</strong>age.<br />
• SUMMARY<br />
• Testis and paratesticular tissue: Non-Hodgk<strong>in</strong>'s lymphoma; subclassification based on flow<br />
cytometry and immunoperoxidase results
Case 8: Female 35 – enlarg<strong>in</strong>g<br />
pa<strong>in</strong>ful soft tissue mass <strong>in</strong> left foot
Case 8: Female 35 – enlarg<strong>in</strong>g<br />
pa<strong>in</strong>ful soft tissue mass <strong>in</strong> left foot<br />
• MICROSCOPIC<br />
• There is a tumour present with<strong>in</strong> a tendon or aponeurosis with adjacent skeletal muscle. The<br />
tumour shows central necrosis. The viable tumour consists of cells with large vesicular nuclei,<br />
prom<strong>in</strong>ent nucleoli and a moderate amount of eccentrically located d eos<strong>in</strong>ophilic cytoplasm<br />
arranged <strong>in</strong> nests separated by fibrous septa. Focally there is stream<strong>in</strong>g of cells with<strong>in</strong> nests.<br />
The tumour is well circumscribed but not encapsulated. Mitotic figures are present.<br />
• Comment<br />
• The histologic appearance is that of a soft tissue malignant tumour. The location of the tumour<br />
and the histology would favour a clear cell sarcoma of tendon and d aponeurosis with a differential<br />
diagnosis which <strong>in</strong>cludes metastatic melanoma, synovial sarcoma, epitheloid sarcoma, malignant<br />
peripheral nerve sheath tumour and metastatic carc<strong>in</strong>oma.<br />
• Investigations<br />
• Cytogenetic for characteristic t(12;22) of clear cell sarcoma<br />
• Immunoperoxidase sta<strong>in</strong>s: S100, HMB45, Leu7, NSE– positive <strong>in</strong> clear cell sarcoma .<br />
• Kerat<strong>in</strong>, EMA, CD99, Bcl2 – positive <strong>in</strong> synovial sarcoma<br />
• CAM5.2, EMA, viment<strong>in</strong>, , CD34 – positive <strong>in</strong> epitheloid sarcoma<br />
• S100 – variable positive <strong>in</strong> malignant peripheral nerve sheath tumour<br />
• AE1/AE3, CK5/6, CAM5.2 – positive <strong>in</strong> carc<strong>in</strong>oma<br />
• SUMMARY<br />
• Left foot: Clear cell sarcoma of tendon and aponeurosis
Case 9: Male 60 – left pleural mass
Case 9: Male 60 – left pleural mass<br />
• MICROSCOPIC<br />
• The entire section consists of tumour which is composed of <strong>in</strong>terlac<strong>in</strong>g bland cells with elongated<br />
cytoplasm consistent with fibroblasts. These are separated by collagen. c<br />
In places the collagen<br />
appears slightly oedematous and other areas compact. A scatter<strong>in</strong>g of mast cells is present<br />
throughout the tumour. No mitotic figures can be identified and there is no evidence of<br />
cytological atypia.<br />
• Comment<br />
• The histology favours a benign lesion of such as a solitary fibrous tumour of the pleura. The<br />
differential diagnosis may <strong>in</strong>clude a sarcomatoid mesothelioma, a monophasic synovial sarcoma<br />
and possibly a nerve sheath tumour however the histology does not t favour a malignant lesion.<br />
• Investigations<br />
• CD 34 and BCL 2 would be performed and positivity would confirm the diagnosis of a solitary<br />
fibrous tumour. Immunoperoxidase sta<strong>in</strong>s for CK5/6 should be negative and if the positive would<br />
raise the possibility of a mesothelioma. Synovial sarcoma. may show s<br />
positive sta<strong>in</strong><strong>in</strong>g for<br />
kerat<strong>in</strong>,EMA,bcl2 and CD99 and is usually negative for CD34.<br />
• SUMMARY<br />
• Left pleural mass: Solitary fibrous tumour
Case 10: Male 4 days old –<br />
neonatal liver failure and death
Case 10: Male 4 days old –<br />
neonatal liver failure and death<br />
• MICROSCOPIC<br />
• The hepatic architecture appears to have been <strong>in</strong>tact with normal central ve<strong>in</strong> - portal<br />
tract relationships. Geographic areas of acute hepatocellular necrosis n<br />
with very little<br />
<strong>in</strong>flammation are present. With<strong>in</strong> the areas of necrosis there are e degenerate cells<br />
with eos<strong>in</strong>ophilic nuclear <strong>in</strong>clusions and marg<strong>in</strong>ated chromat<strong>in</strong>. These <strong>in</strong>clusions<br />
appear to be viral <strong>in</strong> nature. Cytoplasmic <strong>in</strong>clusions are unable e to be identified and<br />
the nuclei do not appear to the markedly enlarged.<br />
• Comment<br />
• The viral <strong>in</strong>clusions are consistent with herpes virus <strong>in</strong>fection and<br />
immunohistochemistry for HSV 1 and HSV 2 as well as PCR for herpes es virus 1 and<br />
herpes virus 2 will be undertaken to confirm the nature of the virus. v<br />
The morphology<br />
of the <strong>in</strong>fected cells is not typical for cytomegalovirus and the necrosis and the type<br />
of cells <strong>in</strong>fected are not typical for parvovirus B 19 however immunohistochemistry<br />
munohistochemistry<br />
and PCR can also be undertaken to exclude these diagnoses.<br />
• SUMMARY<br />
• Liver: Herpes simplex virus <strong>in</strong>fection.
Case 11: Female 52 – nausea,<br />
abdom<strong>in</strong>al pa<strong>in</strong>, iron deficiency<br />
anaemia
Case 11: Female 52 – nausea,<br />
abdom<strong>in</strong>al pa<strong>in</strong>, iron deficiency<br />
anaemia<br />
• MICROSCOPIC<br />
• There are five fragments of small <strong>in</strong>test<strong>in</strong>al mucosa<br />
present on the slide. Brunner’s s glands are evident <strong>in</strong><br />
one of the fragments <strong>in</strong>dicat<strong>in</strong>g that the biopsies are<br />
from the duodenum. The villi appear to be of normal<br />
length with normal villus crypt ratio. The surface<br />
epithelium and brush border are normal. There is no<br />
evidence of <strong>in</strong>creased numbers of lymphocytes with<strong>in</strong><br />
the surface epithelium. There is no evidence of<br />
<strong>in</strong>creased number of <strong>in</strong>flammatory cells the lam<strong>in</strong>a<br />
propria. No Giardia can be identified.<br />
• SUMMARY<br />
• Histologically normal duodenal mucosa.
Case 12: Male 52 – burns on<br />
hands, tissue from thickened ulnar<br />
nerve
Case 12: Male 52 – burns on<br />
hands, tissue from thickened ulnar<br />
nerve<br />
• MICROSCOPIC<br />
• The submitted slide shows soft tissue conta<strong>in</strong><strong>in</strong>g an area of granulomatous<br />
<strong>in</strong>flammation. The <strong>in</strong>flammation is well circumscribed but not encapsulated, shows<br />
central necrosis and a peripheral rim of mononuclear cells <strong>in</strong>clud<strong>in</strong>g macrophages and<br />
lymphocytes. Residual peripheral nerve is unable to be identified. ed. Adjacent to this<br />
there is a small l<strong>in</strong>ear structure which appears to represent a small s<br />
nerve. This<br />
shows per<strong>in</strong>eural and <strong>in</strong>traneural <strong>in</strong>filtration by lymphocytes.<br />
• Comment: Correlation of the histological f<strong>in</strong>d<strong>in</strong>gs of granulomatous <strong>in</strong>flammation<br />
and per<strong>in</strong>eural <strong>in</strong>flammation with the cl<strong>in</strong>ical history of burns on hands and a<br />
thickened ulnar nerve is consistent with a diagnosis of leprosy <strong>in</strong>volv<strong>in</strong>g the ulnar<br />
nerve.<br />
• Investigations<br />
• Immunoperoxidase sta<strong>in</strong> for EMA and S100 may demonstrate residual per<strong>in</strong>eurium<br />
and Schwann cells. A Wade-Fite<br />
sta<strong>in</strong> or PCR for Mycobacterium leprae would be<br />
undertaken to confirm the presence of organisms.<br />
• SUMMARY<br />
• Ulnar nerve: Granulomatous <strong>in</strong>flammation consistent with leprosy.
Case 13: Male 65 – tumour at the<br />
base of ur<strong>in</strong>ary bladder
Case 13: Male 65 – tumour at the<br />
base of ur<strong>in</strong>ary bladder<br />
• MICROSCOPIC<br />
• There are multiple fragments of adenocarc<strong>in</strong>oma present. There is crush<br />
artefact. The carc<strong>in</strong>oma has a papillary and glandular pattern. The<br />
glandular and papillary structures are l<strong>in</strong>ed by columnar to pseudostratified<br />
columnar epithelium. Mitoses are numerous. No prostatic tissue can be<br />
identified. There is a fragment of smooth muscle and fibrous tissue<br />
consistent with bladder wall.<br />
• Comment<br />
• There is an adenocarc<strong>in</strong>oma present. At the base of the bladder this is<br />
more likely to represent a prostatic adenocarc<strong>in</strong>oma rather than a primary<br />
bladder adenocarc<strong>in</strong>oma. Immunoperoxidase sta<strong>in</strong>s for PSA and PAP would<br />
be performed. As the morphology of the tumour favours a prostatic ductal<br />
adenocarc<strong>in</strong>oma these would be expected to be positive to confirm the<br />
diagnosis. If the PSA and PAP are negative <strong>in</strong>vestigations to exclude the<br />
possibility of a metastatic adenocarc<strong>in</strong>oma (eg CEA) will be undertaken.<br />
• SUMMARY<br />
• Bladder: Large duct carc<strong>in</strong>oma of prostate
Case 14: Female 45 – left temporal<br />
lobe mass
Case 14: Female 45 – left temporal<br />
lobe mass<br />
• MICROSCOPIC<br />
• There is a th<strong>in</strong> layer of men<strong>in</strong>ges overly<strong>in</strong>g the cerebral cortex. There is a diffuse<br />
<strong>in</strong>filtrate of relatively uniform small cells with round nuclei throughout t<br />
the white<br />
matter and the overly<strong>in</strong>g grey matter. These show cells show "satellitosis" around<br />
the cortical neurones and also condensation <strong>in</strong> the outer cortex. Most of the cells<br />
have poorly def<strong>in</strong>ed cytoplasm and the nuclei appear to be surrounded by a clear<br />
halo however some cells show an eccentric collection of eos<strong>in</strong>ophilic ilic cytoplasm. An<br />
area of microcystic change is present.<br />
• Comment: The histology is of a diffuse glioma and the cellular morphology<br />
comb<strong>in</strong>ed with the pattern of <strong>in</strong>filtration is consistent with an oligodendroglioma. The<br />
differential diagnosis may <strong>in</strong>clude a diffuse low grade glioma however on<br />
morphological grounds (diffuse <strong>in</strong>filtration of uniform cells with pe<strong>in</strong>uclear clear<strong>in</strong>g)<br />
this is less likely.<br />
• Investigations: FISH studies for allelic losses from chromosomes 1p and 19q<br />
should be undertaken and these may give prognostic <strong>in</strong>dications as well as assist<strong>in</strong><br />
confirmation of the diagnosis.<br />
• SUMMARY<br />
• Bra<strong>in</strong>: Oligodendroglioma
Case 15: Female 40 – right orbital<br />
mass
Case 15: Female 40 – right orbital<br />
mass<br />
• MICROSCOPIC<br />
• The slide shows fibrous tissue <strong>in</strong>filtrated by a population of predom<strong>in</strong>antly small lymphoid cells.<br />
The cells are atypical and have slightly irregular nuclei with m<strong>in</strong>imal m<br />
discernible cytoplasm. There<br />
are scattered larger cells with vesicular nuclei and small nucleoli. No follicular structures or<br />
lymphoepithelial lesions can be identified.<br />
• Comment<br />
• The histologic appearance is that of a lymphoma. While this appears to be a small cell lymphoma<br />
and the location <strong>in</strong> the orbit favours an extra nodal marg<strong>in</strong>al zone lymphoma further<br />
categorisation requires confirmation by flow cytometry and immunoperoxidase sta<strong>in</strong>s.<br />
• Investigations<br />
• Check if tissue has been submitted for flow cytometry and confirm m a monoclonal population<br />
• Tissue for cytogenetics<br />
• Immunoperoxidase sta<strong>in</strong>s CD20, CD79a, CD21 and possibly CD43 would d be expected the positive<br />
<strong>in</strong> a MALT lymphoma and CD5, CD10 and Bcl6 would be expected to be negative. CD10 positivity<br />
comb<strong>in</strong>ed with Bcl2 positive sta<strong>in</strong><strong>in</strong>g would favour <strong>in</strong>volvement by follicular lymphoma (however<br />
no follicular structures can be identified <strong>in</strong> the slide exam<strong>in</strong>ed) ) and positive sta<strong>in</strong><strong>in</strong>g for CD5 <strong>in</strong><br />
comb<strong>in</strong>ation with cycl<strong>in</strong>D1 positivity would favour a Mantle cell lymphoma. If the lymphoma is<br />
CD5 and CD23 positive small lymphocytic lymphoma is likely.<br />
• SUMMARY<br />
• Orbit: : Favour small B-cell B<br />
lymphoma; await further characterization
“At some po<strong>in</strong>t ….. Genu<strong>in</strong>e regard must be given to the<br />
supervisors assessment of the candidate’s s qualities….”<br />
“So far it appears scant regard has been given ….. To the<br />
op<strong>in</strong>ions of those who have worked closely with the candidate….”<br />
• Supervisor’s s reports are considered <strong>in</strong> borderl<strong>in</strong>e cases and at<br />
the oral exam<strong>in</strong>ations.<br />
• However:<br />
– The practical exam may highlight deficiencies not previously<br />
appreciated, but later accepted by the supervisor as be<strong>in</strong>g an area of<br />
concern.<br />
– With the present exam<strong>in</strong>ation system, a candidate who has clearly failed<br />
the practical cannot be granted a pass on the say so of the supervisor and<br />
yet some supervisors have lobbied the previous Chief Exam<strong>in</strong>ers <strong>in</strong> this<br />
way<br />
– Many supervisor reports are cursory, and therefore not helpful, <strong>in</strong> their<br />
approach despite the new format of the report<br />
– Through personality clashes and supervision from a distance, some<br />
supervisors reports are unfair to and may be biased aga<strong>in</strong>st the<br />
candidate.<br />
10.3.06
What’s s under consideration?<br />
• Supervisors reports/ongo<strong>in</strong>g <strong>in</strong> house assessment<br />
• Tra<strong>in</strong>ee Diary – can this be used as an objective<br />
measure of some areas of competence?<br />
• Discussion of % weight<strong>in</strong>g of cont<strong>in</strong>u<strong>in</strong>g assessment<br />
towards the overall results for the exam<strong>in</strong>ations is<br />
underway. A figure of 25% of the total assessment has<br />
been proposed but the content and objective criteria to<br />
be used are still under discussion.<br />
10.3.06
What’s s under consideration?<br />
• It must be acknowledged that, if this system is<br />
implemented, <strong>in</strong> any <strong>in</strong>dividual case where there is a<br />
marked discrepancy between an <strong>in</strong>dividual’s “<strong>in</strong><br />
house” assessments and the results of formal<br />
exam<strong>in</strong>ations, the matter should be referred for<br />
appraisal to a panel formed by the Chief Exam<strong>in</strong>er and<br />
chaired by the Chairman of the BoC. . Similarly, if there<br />
was cont<strong>in</strong>ued significant discrepancy between the <strong>in</strong><br />
house assessments from a s<strong>in</strong>gle <strong>in</strong>stitution and the<br />
results of candidates <strong>in</strong> the formal exam<strong>in</strong>ations, then<br />
the <strong>in</strong>stitution and their assessment process should be<br />
formally reviewed.<br />
10.3.06
What’s s under consideration?<br />
• Accreditation of supervisors –<br />
In l<strong>in</strong>e with AMC requirements consideration has to<br />
be given to formal accreditation of supervisors – the<br />
mechanism is under discussion but would necessarily<br />
<strong>in</strong>clude cont<strong>in</strong>u<strong>in</strong>g updates to ensure familiarity with<br />
supervisors role/requirements and the assessment<br />
process.<br />
10.3.06
References for relevant <strong>in</strong>formation<br />
• Refer to the Latest Tra<strong>in</strong>ee Handbook, and<br />
all the other documents available on the<br />
College Web Site<br />
10.3.06