Sample physician query form - Acumentra Health
Sample physician query form - Acumentra Health
Sample physician query form - Acumentra Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
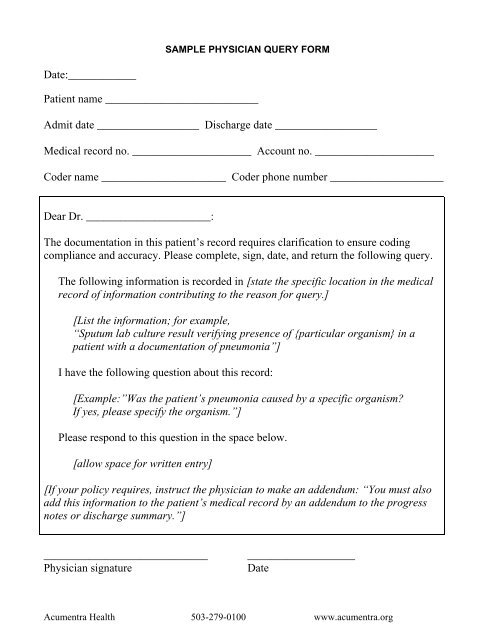
SAMPLE PHYSICIAN QUERY FORM<br />
Date:____________<br />
Patient name ___________________________<br />
Admit date __________________ Discharge date __________________<br />
Medical record no. _____________________ Account no. _____________________<br />
Coder name ______________________ Coder phone number ____________________<br />
Dear Dr. ______________________:<br />
The documentation in this patient’s record requires clarification to ensure coding<br />
compliance and accuracy. Please complete, sign, date, and return the following <strong>query</strong>.<br />
The following in<strong>form</strong>ation is recorded in [state the specific location in the medical<br />
record of in<strong>form</strong>ation contributing to the reason for <strong>query</strong>.]<br />
[List the in<strong>form</strong>ation; for example,<br />
“Sputum lab culture result verifying presence of {particular organism} in a<br />
patient with a documentation of pneumonia”]<br />
I have the following question about this record:<br />
[Example:”Was the patient’s pneumonia caused by a specific organism?<br />
If yes, please specify the organism.”]<br />
Please respond to this question in the space below.<br />
[allow space for written entry]<br />
[If your policy requires, instruct the <strong>physician</strong> to make an addendum: “You must also<br />
add this in<strong>form</strong>ation to the patient’s medical record by an addendum to the progress<br />
notes or discharge summary.”]<br />
_____________________________<br />
Physician signature<br />
___________________<br />
Date<br />
<strong>Acumentra</strong> <strong>Health</strong> 503-279-0100 www.acumentra.org
PHYSICIAN QUERY AND MEDICAL RECORD ADDENDUM<br />
Date:____________<br />
Patient name ___________________________<br />
Admit date __________________ Discharge date __________________<br />
Medical record no. _____________________ Account no. _____________________<br />
Coder name ______________________ Coder phone number ____________________<br />
Dear Dr. ______________________:<br />
The documentation in this patient’s record requires clarification to ensure coding<br />
compliance and accuracy. Please complete, sign, date, and return the following<br />
<strong>query</strong>, as it will become part of the patient’s medical record.<br />
The following in<strong>form</strong>ation is recorded in ______________________________.<br />
I have the following question about this record:<br />
Please respond to this question in the space below.<br />
_____________________________<br />
Physician signature<br />
___________________<br />
Date<br />
<strong>Acumentra</strong> <strong>Health</strong> 503-279-0100 www.acumentra.org
PHYSICIAN QUERY<br />
Date:____________<br />
Patient name ___________________________<br />
Admit date __________________ Discharge date __________________<br />
Medical record no. _____________________ Account no. _____________________<br />
Coder name ______________________ Coder phone number ____________________<br />
Dear Dr. ______________________:<br />
The documentation in this patient’s record requires clarification to ensure coding<br />
compliance and accuracy. Please complete, sign, date, and return the following <strong>query</strong>.<br />
The following in<strong>form</strong>ation is recorded in ______________________________.<br />
I have the following question about this record:<br />
Please respond to this question in the space below.<br />
Important: You must also add this in<strong>form</strong>ation to the patient’s medical record<br />
by a separate addendum to the progress notes or discharge summary.<br />
_____________________________<br />
Physician signature<br />
___________________<br />
Date<br />
<strong>Acumentra</strong> <strong>Health</strong> 503-279-0100 www.acumentra.org
This material was prepared by <strong>Acumentra</strong> <strong>Health</strong>, Oregon’s Medicare Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an<br />
agency of the U.S. Department of <strong>Health</strong> and Human Services. The contents presented do not necessarily reflect CMS policy.<br />
8SOW-OR-REV-07-06<br />
10/10/07<br />
<strong>Acumentra</strong> <strong>Health</strong> 503-279-0100 www.acumentra.org