Newsletter of the Hypertension Initiative & ASH Carolinas-Georgia ...
Newsletter of the Hypertension Initiative & ASH Carolinas-Georgia ...
Newsletter of the Hypertension Initiative & ASH Carolinas-Georgia ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Newsletter</strong> <strong>of</strong> <strong>the</strong><br />
<strong>Hypertension</strong> <strong>Initiative</strong> &<br />
<strong>ASH</strong> <strong>Carolinas</strong>-<strong>Georgia</strong>-<br />
Florida Chapter<br />
F o c u s 2 0 0 9 :<br />
I m p r o v i n g B P<br />
i n R e s i s t a n t<br />
H y p e r t e n s i o n<br />
& M u l t i p l e R i s k<br />
F a c t o r C o n t r o l<br />
S P E C I A L P O I N T S<br />
O F I N T E R E S T :<br />
• A “STITCH” in time saves .<br />
. . An option for better BP<br />
control<br />
• ACCOMPLISHing better<br />
patient outcomes with FDC<br />
I N S I D E T H I S<br />
I S S U E :<br />
HTN Specialists vs<br />
Renin-Guided Rx in<br />
Resistant HTN<br />
<strong>ASH</strong> <strong>Hypertension</strong><br />
Specialists<br />
2<br />
2<br />
V O L U M E 2 # 1<br />
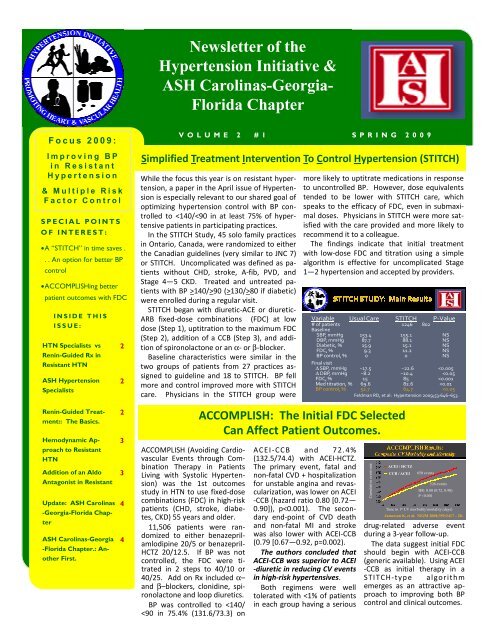
Simplified Treatment Intervention To Control <strong>Hypertension</strong> (STITCH)<br />
While <strong>the</strong> focus this year is on resistant hypertension,<br />
a paper in <strong>the</strong> April issue <strong>of</strong> <strong>Hypertension</strong><br />
is especially relevant to our shared goal <strong>of</strong><br />
optimizing hypertension control with BP controlled<br />
to 90 (>130/>80 if diabetic)<br />
were enrolled during a regular visit.<br />
STITCH began with diuretic-ACE or diuretic-<br />
ARB fixed-dose combinations (FDC) at low<br />
dose (Step 1), uptitration to <strong>the</strong> maximum FDC<br />
(Step 2), addition <strong>of</strong> a CCB (Step 3), and addition<br />
<strong>of</strong> spironolactone or an α- or β-blocker.<br />
Baseline characteristics were similar in <strong>the</strong><br />
two groups <strong>of</strong> patients from 27 practices assigned<br />
to guideline and 18 to STITCH. BP fell<br />
more and control improved more with STITCH<br />
care. Physicians in <strong>the</strong> STITCH group were<br />
S P R I N G 2 0 0 9<br />
more likely to uptitrate medications in response<br />
to uncontrolled BP. However, dose equivalents<br />
tended to be lower with STITCH care, which<br />
speaks to <strong>the</strong> efficacy <strong>of</strong> FDC, even in submaximal<br />
doses. Physicians in STITCH were more satisfied<br />
with <strong>the</strong> care provided and more likely to<br />
recommend it to a colleague.<br />
The findings indicate that initial treatment<br />
with low-dose FDC and titration using a simple<br />
algorithm is effective for uncomplicated Stage<br />
1—2 hypertension and accepted by providers.<br />
Variable Usual Care STITCH P-Value<br />
# <strong>of</strong> patients 1246 802<br />
Baseline<br />
SBP, mmHg 153.4 155.1 NS<br />
DBP, mmHg 87.7 88.1 NS<br />
Diabetic, % 15.9 15.1 NS<br />
FDC, % 9.3 11.2 NS<br />
BP control, % 0 0 NS<br />
Final visit<br />
∆ SBP, mmHg −17.5 −22.6
P A G E 2<br />
In treated, but uncontrolled<br />
HTN,<br />
renin-guided Rx<br />
(RGT) improves control<br />
and lowers BP<br />
equally well or better<br />
than HTN Specialists,<br />
indicating<br />
that RGT provides a<br />
reasonable strategy<br />
in <strong>the</strong>se patients<br />
HTN Specialists vs Renin-Guided Rx<br />
in Resistant <strong>Hypertension</strong><br />
As noted in <strong>the</strong> previous newsletter, clinical<br />
trials suggest that >20% <strong>of</strong> hypertensives are<br />
treatment resistant, which is close to <strong>the</strong><br />
16% rate among practices in <strong>the</strong> <strong>Initiative</strong>.<br />
Highly scalable and effective strategies are<br />
needed that can be applied in primary care.<br />
With this in mind, we teamed with Drs.<br />
Laragh and Sealey to compare HTN Specialists<br />
(Basile, Rehman, Egan) to renin-guided<br />
Rx in patients in 77 patients with treated and<br />
uncontrolled hypertension. Renin samples<br />
were drawn during a routine clinic visit, while<br />
patients were taking <strong>the</strong>ir usual medications.<br />
Without increasing <strong>the</strong> # <strong>of</strong> medications,<br />
SBP and DBP fell in both groups, although<br />
SBP fell more with renin-guided Rx. Thus,<br />
renin-guided Rx emerges as an option for <strong>the</strong> resistant<br />
HTN patient.<br />
Variable Renin-Guided Rx (39) HTN Specialist (38)<br />
Baseline BP<br />
#BP Meds<br />
Final BP<br />
#BP Meds<br />
Change BP<br />
Change Meds<br />
Renin-Guided Therapeutics in<br />
Rx, Uncontrolled Hypertensives<br />
157.0±2.6 / 87.1±2.0<br />
3.1±0.3<br />
127.9±2.3/73.1±1.8<br />
3.1±0.2<br />
−29.1±3.2/−14.1±1.9<br />
+0.0±0.2<br />
153.2±2.3 / 91.1±2.0<br />
2.7±0.2<br />
134.0±2.879.8±1.9<br />
3.0±0.2<br />
−19.2±3.2/−11.3±2.0<br />
+0.3±0.1<br />
p
V O L U M E 2 # 1 S P R I N G 2 0 0 9<br />
Hemodynamic Approach to Resistant HTN<br />
P A G E 3<br />
Hemodynamic Pr<strong>of</strong>ile and<br />
Treatment Options in <strong>Hypertension</strong><br />
Algorithm adapted from: Smith R, et al. <strong>Hypertension</strong>. 2006;47:769-775. Taler SJ, et al.<br />
<strong>Hypertension</strong>. 2002;39:982-988.<br />
Impedance cardiography (IC) has been used to successfully<br />
guide BP medication selection and improve control in<br />
treated, uncontrolled hypertension (references above).<br />
In brief, in uncontrolled hypertensives with a high cardiac<br />
index, >4.2 L/m 2 , beta-blockers or non-dihyrdropyridine<br />
CCBs (diltiazem, verapamil) are added or <strong>the</strong> doses increased.<br />
Conversely, if systemic vascular resistance index is >2580<br />
units/m 2 , <strong>the</strong>n ACE inhibitors, ARBs, non-dihyrdropyridine<br />
CCBs or o<strong>the</strong>r vasodilators are utilized.<br />
Diuretics are increased or added if thoracic fluid content (TFC)<br />
rises on non-diuretic <strong>the</strong>rapy or fails to decrease significantly<br />
on diuretic treatment as indicated in <strong>the</strong> algorithm above.<br />
Addition <strong>of</strong> an Aldo Antagonist in Resistant <strong>Hypertension</strong><br />
In 76 subjects with resistant HTN, including<br />
34 patients with 1 O aldo, lowdose<br />
spironolactone (12.5 – 50 mg/d)<br />
lowered BP 21±21/10±12 at 6 weeks<br />
and 25±20 / 12±12 at 3 months. BP fell<br />
similarly in subjects with and without 1 O<br />
aldo. The authors concluded that lowdose<br />
spironolactone provided significant<br />
BP reduction in African American and<br />
white subjects with resistant hypertension<br />
with and without 1 O aldo. This paper<br />
by Calhoun and colleagues was published<br />
in <strong>the</strong> Am J Hyperten 2003;16:92.<br />
In ASCOT, <strong>the</strong> effect <strong>of</strong> low-dose spironolactone<br />
was evaluated in 1411 participants<br />
with uncontrolled BP on three<br />
medications. During spironolactone<br />
<strong>the</strong>rapy (mean dose 25 mg), BP fell by<br />
21.9/9.5 mmHg, p
American Society <strong>of</strong><br />
<strong>Hypertension</strong><br />
<strong>Carolinas</strong>-<strong>Georgia</strong>-<br />
Florida Chapter<br />
Continuing Medical Education<br />
The <strong>ASH</strong> Carolina-<strong>Georgia</strong>-Florida Chapter is preparing<br />
an exciting slate <strong>of</strong> programs for 2009 and<br />
will provide a list <strong>of</strong> programs, topics, and dates<br />
to you as soon as planning is finalized.<br />
<strong>ASH</strong> <strong>Hypertension</strong> Specialist Exam<br />
The <strong>ASH</strong> Clinical <strong>Hypertension</strong> Specialist certifying<br />
examination will take place May 9, 2009. The Chapter<br />
will once again endeavor to maximize <strong>the</strong> number <strong>of</strong><br />
primary care and o<strong>the</strong>r physicians from <strong>the</strong> Sou<strong>the</strong>ast<br />
who take and successfully complete <strong>the</strong> certifying<br />
exam. Contact us or go to <strong>the</strong> <strong>ASH</strong> website (www.ashus.org)<br />
to learn more about <strong>the</strong> Specialist’s Exam.<br />
Chapter Contact Information:<br />
<strong>Carolinas</strong>-<strong>Georgia</strong>-Florida Chapter<br />
American Society <strong>of</strong> <strong>Hypertension</strong><br />
135 Cannon Street, 3rd Floor<br />
Charleston, SC 29425<br />
Tel: 843.876.1141<br />
Fax: 843.876.1143<br />
email: Lackland@musc.edu<br />
A Partnership for Excellence in CV Health<br />
The <strong>Hypertension</strong> <strong>Initiative</strong> and <strong>ASH</strong> <strong>Carolinas</strong>-<br />
<strong>Georgia</strong>-Florida Chapter are partners with you<br />
to optimize management <strong>of</strong> hypertension, hyperlipidemia<br />
and diabetes. Through this collaborative<br />
effort, we can help transition our<br />
region from a leader in cardiovascular disease<br />
to a model <strong>of</strong> heart and vascular health.<br />
Key strategies include: (1) CME programs<br />
(2) ensuring that <strong>Hypertension</strong> Specialists are<br />
available in communities throughout <strong>the</strong> region<br />
(3) practice data audit and feedback reports to<br />
support your quality improvement efforts<br />
(4) targeted practice-based interventions and<br />
sharing <strong>of</strong> best practices.<br />
For information about <strong>the</strong> <strong>Initiative</strong> contact:<br />
Brent Egan, MD<br />
E-mail: eganbm@musc.edu<br />
Phone: 843-792-1715<br />
<strong>ASH</strong> <strong>Carolinas</strong>-<strong>Georgia</strong>-Florida Chapter: Ano<strong>the</strong>r first.<br />
One quality improvement strategy<br />
<strong>of</strong> <strong>the</strong> <strong>ASH</strong> <strong>Carolinas</strong>-<strong>Georgia</strong>-<br />
Florida Chapter has been to develop<br />
a cadre <strong>of</strong> <strong>ASH</strong> Clinical <strong>Hypertension</strong><br />
Specialists, so that <strong>the</strong>re is<br />
1 Specialist for every 20 primary<br />
care physicians. To fur<strong>the</strong>r ensure<br />
that <strong>the</strong> expertise is present in <strong>the</strong><br />
local community, a related goal is<br />
to have at least 1 <strong>Hypertension</strong><br />
Specialist in every county <strong>of</strong> Chapter<br />
States. We believe that this is<br />
<strong>the</strong> number and distribution <strong>of</strong> <strong>Hypertension</strong><br />
Specialists required to<br />
have a significant impact on BP<br />
control throughout <strong>the</strong> region encompassed<br />
by <strong>the</strong> Chapter.<br />
To realize this impact, <strong>Hypertension</strong><br />
Specialists would have a tripartite<br />
mission including excellence in: (1)<br />
patient care (2) education for o<strong>the</strong>r<br />
practitioners and <strong>the</strong> public (3)<br />
health-services research to develop,<br />
demonstrate and disseminate best<br />
practices (Am H Hypertens<br />
2002;15:372—379; J Clin Hypertens<br />
2006;12:879–886).<br />
The American Society <strong>of</strong> <strong>Hypertension</strong><br />
subsequently endorsed <strong>the</strong>se<br />
objectives as a priority for <strong>the</strong> country.<br />
With <strong>the</strong> leadership <strong>of</strong> Dr. Dan Lackland,<br />
Past-President <strong>of</strong> <strong>the</strong> Chapter,<br />
<strong>the</strong> <strong>ASH</strong> <strong>Hypertension</strong> Specialists<br />
have endorsed a pilot program in<br />
South Carolina. Qualified resident<br />
physicians in training can take <strong>the</strong><br />
examination prior to board certification.<br />
They can receive <strong>the</strong> designation<br />
as an <strong>ASH</strong> <strong>Hypertension</strong> Specialist<br />
concurrently with <strong>the</strong>ir<br />
Boards given a passing score on<br />
both exams.<br />
We look forward to a successful<br />
pilot that can be replicated<br />
throughout <strong>the</strong> entire <strong>Carolinas</strong>-<br />
<strong>Georgia</strong>-Florida Chapter and <strong>the</strong>n<br />
nationally. We’ll plan to provide<br />
updates as this pilot ‘unfolds’.