SLETTO & ASSOCIATES, P - CHG Healthcare Services
SLETTO & ASSOCIATES, P - CHG Healthcare Services
SLETTO & ASSOCIATES, P - CHG Healthcare Services

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
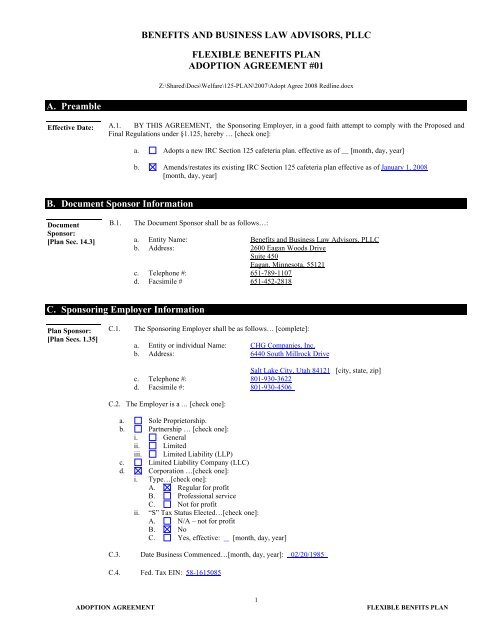
BENEFITS AND BUSINESS LAW ADVISORS, PLLC<br />
FLEXIBLE BENEFITS PLAN<br />
ADOPTION AGREEMENT #01<br />
Z:\Shared\Docs\Welfare\125-PLAN\2007\Adopt Agree 2008 Redline.docx<br />
A. Preamble<br />
Effective Date: A.1. BY THIS AGREEMENT, the Sponsoring Employer, in a good faith attempt to comply with the Proposed and<br />
Final Regulations under §1.125, hereby … [check one]:<br />
a. Adopts a new IRC Section 125 cafeteria plan. effective as of [month, day, year]<br />
b. Amends/restates its existing IRC Section 125 cafeteria plan effective as of January 1, 2008<br />
[month, day, year]<br />
B. Document Sponsor Information<br />
Document<br />
Sponsor:<br />
[Plan Sec. 14.3]<br />
B.1.<br />
The Document Sponsor shall be as follows…:<br />
a. Entity Name: Benefits and Business Law Advisors, PLLC<br />
b. Address: 2600 Eagan Woods Drive<br />
Suite 450<br />
Eagan, Minnesota, 55121<br />
c. Telephone #: 651-789-1107<br />
d. Facsimile # 651-452-2818<br />
C. Sponsoring Employer Information<br />
Plan Sponsor:<br />
[Plan Secs. 1.35]<br />
C.1.<br />
The Sponsoring Employer shall be as follows… [complete]:<br />
a. Entity or individual Name: <strong>CHG</strong> Companies, Inc.<br />
b. Address: 6440 South Millrock Drive<br />
Salt Lake City, Utah 84121 [city, state, zip]<br />
c. Telephone #: 801-930-3622<br />
d. Facsimile #: 801-930-4506<br />
C.2. The Employer is a … [check one]:<br />
a. Sole Proprietorship.<br />
b. Partnership … [check one]:<br />
i. General<br />
ii. Limited<br />
iii. Limited Liability (LLP)<br />
c. Limited Liability Company (LLC)<br />
d. Corporation …[check one]:<br />
i. Type…[check one]:<br />
A. Regular for profit<br />
B. Professional service<br />
C. Not for profit<br />
ii. “S” Tax Status Elected…[check one]:<br />
A. N/A – not for profit<br />
B. No<br />
C. Yes, effective: [month, day, year]<br />
C.3. Date Business Commenced…[month, day, year]: 02/20/1985<br />
C.4. Fed. Tax EIN: 58-1615085<br />
ADOPTION AGREEMENT<br />
1<br />
FLEXIBLE BENFITS PLAN
C.5.<br />
Fiscal Year-End of Employer: December<br />
C.6. Employer’s Principal Trade or Business…[enter same as on IRS Form 5500]:<br />
C.7.<br />
C.8.<br />
Business Code # … [enter same as on Employer’s IRS Tax Return]:<br />
Predecessor Employers … [check one and enter information if applicable]:<br />
a. N/A - no Predecessor Employer(s) existed<br />
b. See attached Predecessor Employer Addendum<br />
c. Enter entity name(s) and information:<br />
Entity Name: Entity Type: Fed. Tax EIN:<br />
Entity Name: Entity Type: Fed. Tax EIN:<br />
C.9. Affiliated Employers … [check one and enter information if applicable]:<br />
a. N/A - no Affiliated Employer(s) existed<br />
b. See attached Affiliated Employer Addendum<br />
c. Enter entity name(s) and information:<br />
Entity Name: CompHealth Associates, Inc. Entity Type: Corp Fed. Tax EIN: 06-0878058<br />
Entity Name: <strong>CHG</strong> Medical Staffing, Inc. Entity Type: Corp Fed. Tax EIN: 87-0502658<br />
Entity Name: <strong>CHG</strong> Management, Inc. Entity Type: Corp Fed. Tax EIN: 51-0343802<br />
Entity Name: Weatherby Locums, Inc. Entity Type: Corp Fed. Tax EIN: 65-0592339<br />
Entity Name: Entity Type: Fed. Tax EIN:<br />
Entity Name: Entity Type: Fed. Tax EIN:<br />
Note:<br />
Affiliated Employers may participate in this Plan by executing the Plan’s Adoption Agreement Participating<br />
Employer Addendum. "Affiliated Employer" means the Sponsoring Employer and those Employers<br />
required to be aggregated with the Sponsoring Employer under sections 414(b), (c), (m) or (o) of the Code.<br />
Such Employers will immediately cease to be a Participating Employer as of the date it ceases to be an<br />
Affiliated Employer.<br />
D. Plan Information<br />
Plan Name and<br />
Number:<br />
[Plan Secs. 1.30]<br />
D.1.<br />
The Plan’s name and number are as follows…[complete]:<br />
a. Current Name of Plan: <strong>CHG</strong> Companies, Inc. Staff Flexible Benefits Plan<br />
b. Previous Name of Plan:<br />
c. Plan Number: 506<br />
Note:<br />
This is the three-digit identifying number [e.g., 501] that the Sponsoring Employer assigns for<br />
Government filing purposes [e.g., Form 5500].<br />
Plan Year:<br />
[Plan Secs. 1.31]<br />
D.2.<br />
Plan Year is as follows…[check each that applies and complete]:<br />
a. The Plan Year is the twelve-consecutive-month period ending each December 31 [month, day]<br />
b. A short Plan Year occurs as follows … [check each that applies]:<br />
i.. The first Plan Year is a short year that began on the Effective Date and ended [month, day,<br />
year]<br />
ii. The Plan Year has been amended. The last Plan Year before the amendment ended<br />
[month, day, year] and the short Plan Year resulting from the amendment began the next day and<br />
ended [month, day, year]<br />
c. The Plan’s Initial Effective Date is as follows: January 1, 2004 [month, day, year]<br />
Note:<br />
Note:<br />
If two or more plans have been merged, or consolidated, insert the original effective date<br />
of the plan shown as the surviving plan for Federal filing purposes (e.g, Form 5500)]<br />
The Plan Anniversary Date is the last day of the applicable Plan Year.<br />
ADOPTION AGREEMENT<br />
2<br />
FLEXIBLE BENFITS PLAN
Plan<br />
Administrator:<br />
[Plan Secs. 1.1<br />
and 13.1]<br />
D.3.<br />
The Plan Administrator is the … [check one]:<br />
Note: To delegate administrative authority to an individual or committee, check item b. or c.<br />
and enter information.<br />
a. Sponsoring Employer, using its address as shown on Item C.1. and the following contact person:<br />
b. The following individual or entity … [complete]:<br />
i. Name:<br />
ii. Address:<br />
[city, state, zip]<br />
iii. Telephone #:<br />
iv. Facsimile #:<br />
v. Fed. I.D. #<br />
c. The following committee or individuals … [check one]:<br />
i. Name of committee:<br />
ii. Committee member(s) … [complete]:<br />
Note:<br />
Either enter the name of the committee or list the individual committee members.<br />
Trust Agreement:<br />
[Plan Secs.16.6]<br />
D.4.<br />
The Plan Trustee(s), if applicable, shall be as follows… [check one]:<br />
a. N/A - Plan assets are not maintained in a Trust [skip to E.1.]<br />
b. Plan assets are maintained in a Trust … [attach Trust Agreement and indicate type of Trustee<br />
and enter information]:<br />
i. Corporate Trustee:<br />
A. Name:<br />
B. Address:<br />
C. Telephone #:<br />
D. Facsimile #:<br />
E. Fed. I.D. #<br />
[city, state, zip]<br />
ii.<br />
Individual Trustee(s) [complete]:<br />
A. Name(s):<br />
B. Address:<br />
1. Use address/telephone/facsimile of Sponsoring Employer<br />
2. Use address/telephone/facsimile of Plan Administrator<br />
3. Use the following address/telephone/facsimile:<br />
a. Address:<br />
b. Telephone #:<br />
c. Facsimile #:<br />
[city, state, zip]<br />
iii.<br />
Unless the Trust Agreement specifically states otherwise, the State law that governs the<br />
Trust is [enter name of state] to the extent that such laws are not preempted by<br />
ERISA<br />
ADOPTION AGREEMENT<br />
3<br />
FLEXIBLE BENFITS PLAN
E. Participation<br />
Eligibility:<br />
[Plan Sec. 2.1]<br />
E.1 In order to be eligible to participate in the following Plan components, an Employee must meet the following<br />
eligibility requirements… [check each that applies]:<br />
Employee<br />
Salary<br />
Reductions<br />
Employer<br />
Contributions<br />
Eligibility<br />
Requirements<br />
N/A – Plan does not provide for this<br />
component<br />
a. AGE: i. N/A – no AGE requirement<br />
ii.<br />
Age<br />
b. SERVICE: i. N/A – no SERVICE requirement<br />
ii.<br />
Days(s) of Service<br />
iii. 1 1 Month(s) of Service<br />
iv.<br />
Year(s) of Service<br />
c. CLASSES:<br />
N/A – no CLASSES included/excluded<br />
included included<br />
The following CLASSES are to be:<br />
excluded excluded<br />
i. Highly Compensated Employee<br />
ii.<br />
iii.<br />
iv.<br />
vi.<br />
vii.<br />
viii.<br />
ix.<br />
Employees whose employment is governed by<br />
the terms of a collective bargaining agreement<br />
[Code § 7701(a)(46)] under which retirement<br />
benefits were the subject of good faith<br />
bargaining<br />
Key Employees<br />
Leased Employees<br />
Salaried Employees<br />
Hourly-wage Employees<br />
Employees paid primarily on a commission<br />
basis<br />
Employees eligible to participate in the<br />
Following Employee benefits plan or program<br />
[enter plan or program name]<br />
x. Employees classified as temporary<br />
xi.<br />
xii.<br />
xiii.<br />
xiv.<br />
Employees classified as seasonal<br />
All except Employees whose employment is<br />
governed by the terms of a collective<br />
bargaining agreement [Code § 7701(a)(46)]<br />
Employees expected to work less than<br />
Hours of Service per [week; pay period;<br />
calendar month; Plan Year quarter; Plan Year;<br />
other]<br />
Other…[enter CLASS included/excluded]<br />
ADOPTION AGREEMENT<br />
d. EXCEPTION: i.<br />
4<br />
N/A - no EXCEPTION<br />
FLEXIBLE BENFITS PLAN
ii.<br />
iii.<br />
iv.<br />
Employees employed as of the effective date<br />
of the most recent Plan amendment<br />
Employees employed as of the Anniversary<br />
Date of the most recent Plan amendment<br />
Other…[enter EXCEPTION]<br />
Date of Entry:<br />
[Plan Sec. 2.2]<br />
E.2 An Employee who meets the above eligibility requirements and who is not an excluded Employee,<br />
shall become a Participant effective as of… [check one and complete]:<br />
a. The date on which the Employee meets the requirements<br />
b. The first day of the pay period [week; pay period; calendar month; Plan Year quarter; other] that<br />
coincides with or next follows the date on which the Employee meets the requirements<br />
c. Same date that the Employee becomes eligible to participate in the Employer’s group<br />
medical plan<br />
d. Same date that the Employee becomes eligible to participate in the following employee<br />
benefits plan or program maintained by the Employer: Group health plan<br />
e. Other:<br />
Service<br />
Determinations:<br />
[Plan Sec. 2.1]<br />
Service with<br />
Other<br />
Employers:<br />
[Plan Sec. 2.3]<br />
E.3 Service will be determined as follows for eligibility purposes, using the … [check one]:<br />
a. N/A – no service requirement for participation in either the Salary Reduction or<br />
Employer Contribution component(s) of the Plan [skip to item F.1.]<br />
b. Elapsed time method<br />
c. Actual hours method<br />
i. An Employee must complete at least Hours of Service during the<br />
ii.<br />
applicable Computation Period for it to count as a of Service.<br />
An Employee for whom a record of actual hours is not maintained or available [e.g., salaried<br />
employees] will be credited with … [check one]:<br />
A. 10 Hours of Service for each day<br />
B. 45 Hours of Service for each week<br />
C. 95 Hours of Service for each semi-monthly payroll period<br />
D. 190 Hours of Service for each month<br />
… in which he/she has one or more Hour(s) of Service.<br />
iii. An Employee for whom a record of actual hours is maintained and available [e.g. hourly employees]<br />
will be credited using … [check one]:<br />
A. Actual hours method<br />
B. The same equivalency as specified in Item E.3.c.ii. above.<br />
iv. The Plan shall use the following computation periods for eligibility purposes… [check one]:<br />
A. N/A – no eligibility service period is specified<br />
B. Employment anniversary shifting to Plan Year<br />
C. Employment anniversary for all years<br />
E.4 An Employee’s service with the following employer(s) will be recognized for eligibility purposes… [check one]:<br />
a. N/A – no other service recognized<br />
b. All entities listed on the Affiliated Employers Addendum<br />
c. Service with the following employer(s) will be recognized…[enter employer’s name(s):<br />
F. Plan Compensation<br />
Plan<br />
Compensation:<br />
[Plan Sec. 1.8]<br />
F.1.<br />
Plan Compensation means earnings … [check one]:<br />
a. Wages, Tips, other Compensation [as reported on the Participant's IRS Form W-2 as required under<br />
sections 6041 and 6051 of the Code]<br />
b. Wages [as that term is defined in section 3401 of the Code for purposes of federal income tax<br />
withholding at the source]<br />
c. 415 (c)(3) Safe-Harbor Compensation<br />
ADOPTION AGREEMENT<br />
5<br />
FLEXIBLE BENFITS PLAN
F.2.<br />
Applicable Period means…[check one]:<br />
a. Plan Year<br />
b. Fiscal Year coinciding with or ending within the Plan Year<br />
c. Calendar Year coinciding with or ending within the Plan Year<br />
F.3.<br />
Plan Compensation exclusions … [check each that applies]:<br />
Employee<br />
Salary<br />
Reduction<br />
Employer<br />
Contribution<br />
Exclusions:<br />
N/A – Plan does not provide for this component<br />
a. N/A – No exclusions<br />
b. N/A Remunerations prior to Date of Entry<br />
c.<br />
Participant Code § 402(a)(8), 402(h)(1)(B) and/or 403(b) Elective<br />
N/A<br />
Deferrals<br />
d. N/A Participant Code § 125 salary reductions (cafeteria plan)<br />
e.<br />
N/A<br />
Reimbursements or other expense allowances, fringe benefits (cash and<br />
non-cash), moving expenses, deferred compensation and welfare benefits<br />
f. Severance pay due to Termination of Service<br />
g. Non-discretionary bonuses<br />
h. Discretionary bonuses<br />
i. Overtime<br />
j. Commissions.<br />
k. Other… [specify]:<br />
G. Benefit Election Period<br />
Benefit<br />
Election<br />
Period:<br />
[Plan Secs. 3.2<br />
and 3.3]<br />
G.1.<br />
The Benefit Election Period prior to the first payroll period that coincides with or next follows the Participant’s<br />
effective date of participation will be…[check one and complete]:<br />
a. A period of [enter number] [day(s), week(s), month(s), other] prior to the Participant’s entry date<br />
b. A period of 30 [enter number] days [day(s), week(s), month(s), other] prior to the first payroll period that<br />
coincides with or next follows the Participant’s effective date of participation<br />
c. A period determined annually at the Administrator's discretion and applied in a<br />
non-discriminatory manner<br />
d. Other… [specify]:<br />
G.2.<br />
The Benefit Election Period prior to each Plan Year for subsequent Plan Year’s of participation will be…[check<br />
one and complete]:<br />
a. A period of 30 [enter number] days [day(s), week(s), month(s), other]<br />
b. From the [enter number] to the [enter number] [day, week, month, other] period<br />
c. A period determined annually at the Administrator's discretion and applied in a<br />
non-discriminatory manner<br />
d. Other… [specify]:<br />
G.3.<br />
The extended Benefit Election Period for Participants who fail to elect during their initial Benefit Election Period<br />
will be…[check one and complete]:<br />
a. N/A – no extended Benefit Election Period<br />
b. A day period prior to [each; the next; other] payroll period(s)<br />
c. From the day of the day period prior to [each; the next; other] payroll period(s)<br />
d. A period prior to [each; the next; other] payroll period(s) determined annually at the<br />
Administrator's discretion and applied in a nondiscriminatory manner<br />
e. Other… [specify]: Thirty (30) days after the end of the Benefit Election Period, or such nondiscriminatory<br />
period determined by the Administrator.<br />
G.4.<br />
Participants who fail to make new Benefit elections during the subsequent Benefit Election Period(s) will [check<br />
one]:<br />
ADOPTION AGREEMENT<br />
a. Continue their prior year elections<br />
b. Continue their prior year elections, but only for insured Benefits<br />
c. Be deemed to have elected not to participate for the upcoming Plan Year<br />
d. Other… [specify]:<br />
6<br />
FLEXIBLE BENFITS PLAN
G.5.<br />
Participants will be automatically enrolled in the Insurance Premium Conversion Program to the extent of the<br />
premiums that they pay for insurance Benefits by payroll withholding… [check one]:<br />
a. N/A – Insurance Premium Conversion program is not available<br />
b. Yes - negative elections are allowed for Participants who do not wish to participate in the Insurance<br />
Premium Conversion program<br />
c. No - participation in the Insurance Premium Conversion program only by positive election<br />
H. Participant Salary Reductions<br />
Participant<br />
salary<br />
Reductions:<br />
[Plan Secs. 4.1<br />
and 4.2]<br />
H.1.<br />
Eligible Employees may elect to have their earnings reduced by… [check one and complete]:<br />
a. Not applicable [Employee Salary Reductions are not allowed - Skip to Section H.3.]<br />
b. By an amount sufficient to fund Benefits selected<br />
c. Percentage [check one or more and enter percentage amount(s)]:<br />
i. Minimum: % of Plan Compensation<br />
ii. Maximum: % of Plan Compensation<br />
d. Dollar [check one or more and enter dollar amount(s)] :<br />
i. Minimum: $ of Compensation<br />
ii. Maximum: $ of Compensation<br />
e. Percentage/Dollar [check one or more and enter dollar amount(s)]:<br />
i. Minimum: % of Plan Compensation or $ of Compensation<br />
ii. Maximum: % of Plan Compensation or $ of Compensation<br />
f. Other [specify]:<br />
H.2.<br />
The Salary Reduction period for the limitation(s) set forth in Item H.1. are as follows…[check one]:<br />
a. Payroll period<br />
b. Month<br />
c. Plan Year quarter<br />
d. Plan Year half<br />
e. Other [specify]:<br />
H.3.<br />
Participants may convert Paid Time Off into Plan contributions:…[check one]:<br />
a. N/A – Paid Time Off conversion not allowed<br />
b. Up to total available Paid Time Off<br />
c. Up to Days Paid Time Off<br />
d. Up to Dollars worth of Paid Time Off<br />
e. To the lesser of Days Paid Time Off or Dollars worth of Paid Time Off<br />
f. Other [specify]:<br />
I. Employer Credits<br />
Employer<br />
Contributions:<br />
[Plan Sec. 5.1]<br />
I.1.<br />
Employer Credits will be calculated as follows… [check one]:<br />
a. Not applicable [Skip to Item J.1.]<br />
b. At the Employer’s discretion<br />
c. dollars per Participant<br />
d. % of Compensation per eligible Participant<br />
e. Pursuant to the following formula…[enter contribution formula]:<br />
f. Other [specify]:<br />
ADOPTION AGREEMENT<br />
7<br />
FLEXIBLE BENFITS PLAN
I.2.<br />
The Employer Credit(s) shall be limited for each eligible Participant … [check one and complete]:<br />
a. Not applicable [no limit]<br />
b. By an amount sufficient to fund Benefits selected<br />
c. Percentage [check one or more and enter percentage amount(s)]:<br />
i. Minimum: % of Plan Compensation<br />
ii. Maximum: % of Plan Compensation<br />
d. Dollar [check one or more and enter dollar amount(s)] :<br />
i. Minimum: $ of Compensation<br />
ii. Maximum: $ of Compensation<br />
e. Percentage/Dollar [check one or more and enter dollar amount(s)]:<br />
i. Minimum: % of Plan Compensation or $ of Compensation<br />
ii. Maximum: % of Plan Compensation or $ of Compensation<br />
f. Other [specify]:<br />
I.3.<br />
The Employer Credit period applicable to Item I.1. and I.2. is as follows…[check one]:<br />
a. Payroll period<br />
b. Month<br />
c. Plan Year quarter<br />
d. Plan Year half<br />
e. Other [specify]:<br />
I.4.<br />
The Employer Credit(s) shall be submitted pro-rata each… [check one]:<br />
a. Pay period<br />
b. Month<br />
d. Plan Year quarter<br />
d. Plan Year half<br />
e. Other [specify]:<br />
Allocation<br />
Requirements:<br />
[Plan Sec. 5.4]<br />
I.5.<br />
To be eligible to receive an Employer Credit allocation for a Plan Year, the Participant<br />
must… [check one]:<br />
a. Not applicable [all Participants are eligible]<br />
b. Other [specify]:<br />
J. Insurance Premium Conversion<br />
Insurance<br />
Premium<br />
Conversion:<br />
[Plan Sec. 6.1]<br />
Dependent<br />
Coverage:<br />
[Plan Sec. 7.1]<br />
J.1.<br />
J.2.<br />
The following Insurance Benefits are available for payment through the Plan on a pre-tax basis… [check one]:<br />
a. N/A - Spending Accounts only [skip to Item J.2.]<br />
b. Accident or Health Insurance [IRC Section 106]<br />
i. Health Care<br />
ii. Accidental Death or Dismemberment<br />
iii. Dental Care<br />
iv. Vision Care<br />
v. Long-Term Disability<br />
vi. Other [specify]:<br />
c. Group-Term Life Insurance [IRC Section 79]<br />
d. Other [specify] :<br />
Dependent coverage may be elected by the Participant for… [check one]:<br />
a. Not applicable [only Participant coverage allowed]<br />
b. Health Care<br />
c. Accidental Death or Dismemberment<br />
d. Dental Care<br />
e. Vision Care<br />
f. Long-Term Disability<br />
g. Group-Term Life Insurance<br />
h. Other [specify] : ____________<br />
J.3.<br />
ADOPTION AGREEMENT<br />
Participants may, at the discretion of the Administrator, obtain individual policies for the following<br />
Insurance Benefits… [check one]:<br />
8<br />
FLEXIBLE BENFITS PLAN
a. Not applicable [no individual policies will be allowed]<br />
b. Health Care<br />
c. Dental Care<br />
d. Vision Care<br />
e. Long-Term Disability<br />
f. Other [specify] :<br />
J.4.<br />
In addition to legal limits, if any, Insurance Benefits will be limited as follows… [check one]:<br />
a. N/A [no additional limits]<br />
b. Other [Note: Group Term Life Insurance coverage over $50,000 of death benefit may result in taxation<br />
to the Participant.]<br />
K. Spending Accounts<br />
Spending<br />
Accounts:<br />
[Plan Sec. 6.2]<br />
K.1.<br />
Spending Accounts will be established for… [check one]:<br />
a. N/A [Insurance Premium Conversion only - skip to Item L.]<br />
b. Medical Reimbursement Expense [IRC Section 106]<br />
c. Dependent Care [IRC Section 129]<br />
d. Adoption Assistance [IRC Section 137]<br />
e. Health Savings Account [IRC Section 223]<br />
d. 401(k) [IRC Section 401(k)]<br />
e. Paid Time Off<br />
f. Cash Payments<br />
g. Other [specify; must not provide benefits which are prohibited under Prop. Reg. 1.125-1(q)]:<br />
K.2.<br />
In addition to legal limits, if any, Spending Accounts will be limited as follows… [check one]:<br />
a. N/A [no additional limits]<br />
b. Medical Reimbursement Expense [IRC Section 106]<br />
i. N/A [no additional limits]<br />
ii. Other [specify]: $5,000<br />
c. Dependent Care [IRC Section 129]<br />
i N/A [no additional limits]<br />
ii. Other [specify]:<br />
d. Adoption Assistance [IRC Section 137]<br />
i. N/A [no additional limits]<br />
ii. Other [specify]:<br />
d. 401(k) [IRC Section 401(k)]<br />
i N/A [no additional limits]<br />
ii. Other [specify]:<br />
e. Paid Time Off<br />
i N/A [no additional limits]<br />
ii. Other [specify]:<br />
f. Cash Payments<br />
i N/A [no additional limits]<br />
ii. Other [specify]:<br />
g. Other [specify]:<br />
Note:<br />
Even if no limit is specified by the Sponsoring Employer, the applicable legal<br />
limits to maintain the tax-qualified status of the applicable Benefit shall apply.<br />
K.3.<br />
For Medical Reimbursement Expense Account reimbursements, new elections due to a Change In Status are:<br />
[check one]:<br />
a. Not applicable [Benefit not allowed]<br />
b. Not permitted<br />
c. Permitted without limitation<br />
d. Permitted, but only to increase Benefit elections<br />
e. Permitted, but not lower than the net amount of claims as of the election date<br />
f. Other [specify]:<br />
ADOPTION AGREEMENT<br />
9<br />
FLEXIBLE BENFITS PLAN
K.4. For Medical Reimbursement Expense, Dependent Care and Adoption Assistance Spending Account<br />
reimbursements, Participants must file Benefit claims… [check one]:<br />
a. Not applicable [No Benefit is allowed]<br />
b. Within days after Plan Year end for expenses incurred in the current Plan Year<br />
c. By March 31 [enter Month and day] of the following Plan Year for expenses incurred in the current<br />
Plan Year<br />
d. Other [specify]:<br />
K.5. The applicable Grace Period for Medical Reimbursement Expense, Dependent Care, and Adoption Assistance<br />
Spending Account reimbursements will be… [check one](not to exceed the time period in K.5.b):<br />
a. Not applicable [No Benefits is allowed]<br />
b. The fifteenth day of the third month following the end of the Plan Year<br />
c. Sixty days after the end of the Plan Year<br />
d. Thirty days after the end of the Plan Year<br />
e. Other [specify]:<br />
K.6.<br />
Spending Account Forfeitures shall be reallocated during the following Plan Year as follows… [check one]:<br />
a. Not applicable<br />
b. Pro-rata by Eligible Participant<br />
c. Used to reduce Employer Contributions<br />
d. Added to Employer Contributions<br />
e. Other [specify]: Used to defray administrative expenses.<br />
K.7. An Employee who becomes ineligible to participate in the plan with an unused salary reduction amount in their<br />
Dependent Care Spending Account will… [check one]:<br />
a. Forfeit the account balance to the Forfeiture Surplus Account.<br />
b. be allowed to “spend down” those funds as long as they satisfy IRC §129.<br />
ADOPTION AGREEMENT<br />
10<br />
FLEXIBLE BENFITS PLAN
L. COBRA Elections<br />
COBRA<br />
Elections:<br />
[Plan Sec. 19.1]<br />
L.1.<br />
For Medical Reimbursements, if Employee is eligible for COBRA coverage, terminated Participants will do one<br />
of the following[check one]:<br />
a. COBRA will be offered as required by federal law and Participant could only elect COBRA if<br />
usage is less than contributions at the time of the Qualifying Event.<br />
b. At Participant’s election, contribution and reimbursements will continue for the remainder of the Plan Year<br />
to the extent initially elected, regardless of the usage at the time of the Qualifying Event.<br />
c. N/A; Medical Reimbursement is not offered under the Plan.<br />
M. FMLA Elections<br />
FMLA<br />
Elections:<br />
[Plan Sec. 20.1]<br />
M.1.<br />
Participants on unpaid FMLA Leave may elect from the following payment options to pay their Group Health<br />
Care Plan premiums… [check as appropriate]:<br />
a. Pay-as-you-go<br />
b. Pre-pay<br />
c. Catch-up<br />
d. Payments waived and paid by Employer with no repayment by the Participant<br />
Note:<br />
Pursuant to IRS Proposed Regulation Section 1.125-3 Q&A-3(b), the following exceptions apply:<br />
a. The pre-pay option cannot be the sole option offered to Eligible Employees on FMLA Leave. However,<br />
the Plan may include pre-payment as an option for Eligible Employees on FMLA Leave, even if<br />
such option is not offered to employees on non-FMLA Leave-without-pay.<br />
b. The catch-up option can be the sole option offered to Eligible Employees on FMLA Leave if and only if the<br />
catch-up option is the sole option offered to employees on non-FMLA Leave-without-pay.<br />
c. The Plan cannot offer Eligible Employees on FMLA Leave a choice of either the pre-pay option or the<br />
catch-up option without also offering the pay-as-you-go option, if the pay-as-you-go option is offered to<br />
employees on non-FMLA Leave-without-pay.<br />
M.2.<br />
Participants on non-FMLA Leave are entitled to, but not required to, continue the following non-health benefits…<br />
[check one]:<br />
a. N/A – non-FMLA Leave benefit continuation not allowed<br />
b. Life Insurance<br />
c. Dependent Care Spending Account<br />
d. Other…[specify] : As determined in Administrator’s discretion<br />
N. Other Elections<br />
N.1.<br />
The following additional Employer elections shall apply to the extent not in conflict with the qualification<br />
requirements of federal tax law or the provisions of the Plan… [check one]:<br />
a. Not applicable [no additional provisions elected]<br />
b. Other…[specify] :<br />
ADOPTION AGREEMENT<br />
11<br />
FLEXIBLE BENFITS PLAN
O. Employer Signatures<br />
IN WITNESS WHEREOF, the Sponsoring Employer has caused this Adoption Agreement to be adopted effective as of the date written on<br />
page 1.<br />
By executing this Adoption Agreement, the Sponsoring Employer certifies and warrants that it has relied on the advice of an attorney<br />
or other independent qualified advisor as to the legal and tax effect of adopting the Plan.<br />
Date signed: ________________________________<br />
Sponsoring Employer: <strong>CHG</strong> Companies, Inc.[same as Item<br />
C.1.A.]:<br />
By<br />
Name (Print)<br />
Its<br />
Trustee(s):<br />
N/A – Plan assets are not maintained in a Trust [Item<br />
D.4.a. elected]<br />
Date signed: ________________________________<br />
Corporate Trustee [Item D.4.b.i. elected - enter same as<br />
Item D.4.b.i.A.]:<br />
Note:<br />
Corporate Trustee signature only when Item D.4.b.1.<br />
of the Adoption Agreement has been completed and<br />
a Trust Agreement attached.<br />
By<br />
Name (Print)<br />
Its<br />
Date signed: ________________________________<br />
Individual Trustee(s) [Item D.4.b.ii. elected - enter same<br />
as Item D.4.b.ii.A.]:<br />
Note:<br />
Individual Trustee(s) signature only when Item<br />
D.4.b.2. of the Adoption Agreement has been<br />
completed and a Trust Agreement attached.<br />
ADOPTION AGREEMENT<br />
12<br />
FLEXIBLE BENFITS PLAN