

Iatrogenic Duodenal Injuries - Department of Surgery at SUNY ...
Iatrogenic Duodenal Injuries - Department of Surgery at SUNY ...
Iatrogenic Duodenal Injuries - Department of Surgery at SUNY ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
www.downst<strong>at</strong>esurgery.org<br />
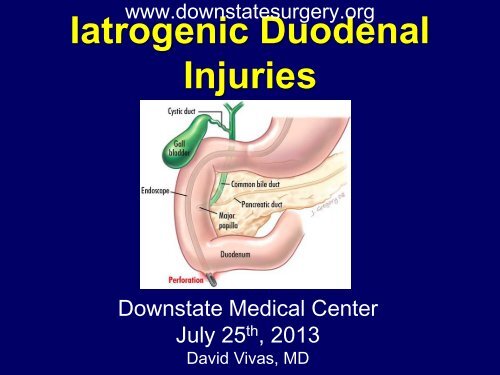
<strong>I<strong>at</strong>rogenic</strong> <strong>Duodenal</strong><br />
<strong>Injuries</strong><br />
Downst<strong>at</strong>e Medical Center<br />
July 25 th , 2013<br />
David Vivas, MD
History<br />
Case<br />
• 71 y/o female who was seen by her PMD c/o 2 h/o<br />
RUQ pain radi<strong>at</strong>ed to the back. P<strong>at</strong>ient denied fevers,<br />
nausea or vomiting. Was found to have elev<strong>at</strong>ed LFT’s<br />
and was referred to the ED.<br />
• P<strong>at</strong>ient was admitted to our service for further work up.<br />
• PMH: Depression, Thalassemia, Reynaud’s<br />
• PSH: Myomectomy<br />
• NKDA<br />
www.downst<strong>at</strong>esurgery.org
Physical Exam<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• P<strong>at</strong>ient in NAD, AAOx3<br />
• Mild jaundice<br />
• C-V: RRR, S1-S2<br />
• Pulm: CTA b/l<br />
• Abdomen: Non distended, s<strong>of</strong>t, tender to palp<strong>at</strong>ion in<br />
RUQ, neg Murphy’s sign. No masses.
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
Labs:<br />
• CBC: 10.45>10.0/30.2
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
HD #1<br />
• P<strong>at</strong>ient had significant improvement in pain. No<br />
fevers, nausea or vomiting<br />
• Started on clear liquid diet<br />
• P<strong>at</strong>ient was assessed by GI<br />
• MRCP<br />
• Trend LFT’s<br />
• Abx<br />
• Plan for possible ERCP
www.downst<strong>at</strong>esurgery.org<br />
MRCP
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
HD #2<br />
• P<strong>at</strong>ient denied abdominal pain<br />
• Toler<strong>at</strong>ing clear liquid diet<br />
• Plan for ERCP next day<br />
• LFT’s trending down
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
HD #3<br />
• ERCP:<br />
• Unsuccessful<br />
• Incidental perfor<strong>at</strong>ion <strong>of</strong> duodenum diverticulum<br />
opposite to ampulla during difficult small bowel<br />
intub<strong>at</strong>ion<br />
• 2 unsuccessful <strong>at</strong>tempts for Hemoclip<br />
placement
www.downst<strong>at</strong>esurgery.org<br />
Case
HD #3<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• P<strong>at</strong>ient transferred to PACU in stable condition<br />
• NGT in place<br />
• <strong>Surgery</strong> notified <strong>of</strong> complic<strong>at</strong>ion<br />
• On initial assessment:<br />
• In NAD<br />
• AVSS<br />
• Abdomen s<strong>of</strong>t, non tender
HD #3<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• Plan:<br />
• CT abdomen with PO/IV contrast<br />
• Transfer to Step-down surgical unit<br />
• NGT/NPO<br />
• IV Abx<br />
• Serial abdominal exams
www.downst<strong>at</strong>esurgery.org
www.downst<strong>at</strong>esurgery.org
HD #3<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• P<strong>at</strong>ient was transferred to Step Down unit<br />
• Multiple assessments during the following<br />
hours<br />
• P<strong>at</strong>ient in NAD, denied abdominal pain<br />
• AVSS<br />
• Abdomen s<strong>of</strong>t, non tender
HD #3<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• Approxim<strong>at</strong>ely 9 hrs. post <strong>at</strong>tempted ERCP:<br />
• P<strong>at</strong>ient now complains <strong>of</strong> RUQ abdominal<br />
pain<br />
• On physical exam:<br />
• AVSS<br />
• Abdomen diffusely tender, particularly in<br />
RUQ<br />
• Decision was made to proceed with emergent<br />
surgical explor<strong>at</strong>ion
HD #3<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• Explor<strong>at</strong>ory laparotomy<br />
• Gush <strong>of</strong> air<br />
• Large infiltr<strong>at</strong>ion <strong>of</strong> air in the<br />
retroperitoneum, colonic mesentery and<br />
small bowel<br />
• Transverse colon intermittently adherent to<br />
duodenum without distinctive demarc<strong>at</strong>ion<br />
between the 2 structures
HD #3<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• Explor<strong>at</strong>ory laparotomy<br />
• 5 mm perfor<strong>at</strong>ion l<strong>at</strong>eral aspect <strong>of</strong> 2 nd portion <strong>of</strong><br />
duodenum with active leak <strong>of</strong> bile and air<br />
• GB appeared thickened and inflamed<br />
• Primary closure and omentoplasty<br />
• JP drain
POD #1-4<br />
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
• P<strong>at</strong>ient NPO<br />
• NGT to LCS<br />
• Abx<br />
• P<strong>at</strong>ient with no mayor complaints, afebrile,<br />
VSS
POD #5<br />
Case<br />
• Afebrile<br />
• NGT with min output discontinued<br />
• + Gas<br />
• No abdominal pain,<br />
• JP drain cont serous output<br />
POD #6<br />
www.downst<strong>at</strong>esurgery.org<br />
• P<strong>at</strong>ient started on clear liquids diet<br />
• Toler<strong>at</strong>ed well
www.downst<strong>at</strong>esurgery.org<br />
Case<br />
POD #8<br />
• Advanced to low f<strong>at</strong> diet<br />
• Toler<strong>at</strong>ed<br />
POD #9<br />
• P<strong>at</strong>ient discharged home
www.downst<strong>at</strong>esurgery.org
www.downst<strong>at</strong>esurgery.org<br />
Questions?
www.downst<strong>at</strong>esurgery.org<br />
<strong>I<strong>at</strong>rogenic</strong> <strong>Duodenal</strong> <strong>Injuries</strong><br />
• ERCP was first introduced in 1968 by McCune et al<br />
and has evolved over the decades<br />
• Currently, it is a valuable, widely used diagnostic<br />
and therapeutic tool in hep<strong>at</strong>o-biliary-pancreas<br />
diseases<br />
• ERCP has a rel<strong>at</strong>ively high complic<strong>at</strong>ion r<strong>at</strong>e <strong>of</strong><br />
nearly 10% and a mortality r<strong>at</strong>e <strong>of</strong> 0.1 to 1%
www.downst<strong>at</strong>esurgery.org<br />
<strong>I<strong>at</strong>rogenic</strong> <strong>Duodenal</strong> <strong>Injuries</strong><br />
• Therapeutic aspects <strong>of</strong> ERCP are becoming more<br />
important<br />
• Endoscopists take on increasingly more complex<br />
cases the risk <strong>of</strong> complic<strong>at</strong>ion is increasing<br />
• Pancre<strong>at</strong>itis, cholangitis, and hemorrhage are more<br />
frequent ERCP complic<strong>at</strong>ions<br />
• ERCP-rel<strong>at</strong>ed perfor<strong>at</strong>ion is one <strong>of</strong> the most feared,<br />
due to its potentially lethal n<strong>at</strong>ure
www.downst<strong>at</strong>esurgery.org<br />
<strong>I<strong>at</strong>rogenic</strong> <strong>Duodenal</strong> <strong>Injuries</strong><br />
Classific<strong>at</strong>ion<br />
• Retroperitoneal duodenal perfor<strong>at</strong>ion<br />
• The most common<br />
• Usually occur as a result <strong>of</strong> a sphincterotomy th<strong>at</strong><br />
extends beyond the intramural portion <strong>of</strong> bile duct<br />
• Perfor<strong>at</strong>ion <strong>of</strong> the bile ducts<br />
• Usually occurs following dil<strong>at</strong>ion <strong>of</strong> strictures, forceful<br />
cannul<strong>at</strong>ion, guidewire insertion, or stent migr<strong>at</strong>ion<br />
• Free bowel-wall perfor<strong>at</strong>ion:<br />
• Rare, usually occurring in p<strong>at</strong>ients with a stricture or<br />
anomalous an<strong>at</strong>omy, such as Billroth II gastrectomy
www.downst<strong>at</strong>esurgery.org<br />
<strong>I<strong>at</strong>rogenic</strong> <strong>Duodenal</strong> <strong>Injuries</strong><br />
Classific<strong>at</strong>ion<br />
• Also reported, but rare following ERCP and<br />
sphincterotomy:<br />
• Gastric and esophageal perfor<strong>at</strong>ions<br />
• Pneumomediastinum without evidence <strong>of</strong><br />
perfor<strong>at</strong>ion<br />
• Intestinal perfor<strong>at</strong>ion rel<strong>at</strong>ed to biliary stents
www.downst<strong>at</strong>esurgery.org<br />
Incidence <strong>of</strong> Retroduodenal<br />
Perfor<strong>at</strong>ion<br />
• Retroduodenal perfor<strong>at</strong>ion was reported in 0.5 to<br />
2.1% <strong>of</strong> sphincterotomies in older large series<br />
• More recently, the incidence <strong>of</strong> perfor<strong>at</strong>ion has<br />
appeared to decrease to less than 0.5%,<br />
probably because <strong>of</strong> improvement in experience<br />
and skill <strong>of</strong> the endoscopists<br />
• Severe and f<strong>at</strong>al cases continue to occur
www.downst<strong>at</strong>esurgery.org<br />
Risk Factors for <strong>Duodenal</strong><br />
Perfor<strong>at</strong>ion<br />
• Risk factors for overall perfor<strong>at</strong>ion:<br />
• P<strong>at</strong>ient rel<strong>at</strong>ed<br />
• Sphincter <strong>of</strong> Oddi dysfunction<br />
• Common bile duct dil<strong>at</strong>ion<br />
• Procedure rel<strong>at</strong>ed<br />
• Performance <strong>of</strong> a sphincterotomy<br />
• Longer dur<strong>at</strong>ion <strong>of</strong> the procedure<br />
• Biliary stricture dil<strong>at</strong>ion
www.downst<strong>at</strong>esurgery.org<br />
Risk Factors for <strong>Duodenal</strong><br />
Perfor<strong>at</strong>ion<br />
• Risk factors for bowel wall perfor<strong>at</strong>ion:<br />
• Stenosis in the upper GI tract or bile ducts<br />
• Abnormal GI an<strong>at</strong>omy (s/p gastrectomy, s/p<br />
pancre<strong>at</strong>icoduodenectomy and situs inversus)<br />
• Particular caution required with use <strong>of</strong> sideviewing<br />
scope in p<strong>at</strong>ients with Billroth II<br />
reconstruction
www.downst<strong>at</strong>esurgery.org<br />
Risk Factors for <strong>Duodenal</strong><br />
Perfor<strong>at</strong>ion<br />
• Risk factors for retroperitoneal perfor<strong>at</strong>ion:<br />
• Precut and larger sphincterotomies<br />
(particularly if cuts cre<strong>at</strong>ed outside the usual<br />
landmarks)<br />
• Small caliber bile duct<br />
• Presence <strong>of</strong> periampullary diverticulum<br />
• Intramural injection <strong>of</strong> contrast
www.downst<strong>at</strong>esurgery.org<br />
Clinical Manifest<strong>at</strong>ions and<br />
Diagnosis<br />
• Perfor<strong>at</strong>ion is rarely evident endoscopically<br />
• Free abdominal perfor<strong>at</strong>ion:<br />
• Almost always recognized immedi<strong>at</strong>ely based upon<br />
clinical symptoms, physical signs and fluoro findings<br />
• Retroduodenal perfor<strong>at</strong>ion:<br />
• Usually determined by the presence <strong>of</strong> air or contrast<br />
in the retroperitoneal space outside the confines <strong>of</strong><br />
the bile ducts and duodenum during CT ordered for<br />
post ERCP pain
www.downst<strong>at</strong>esurgery.org<br />
Clinical Manifest<strong>at</strong>ions and<br />
Diagnosis<br />
• P<strong>at</strong>ients with undetected leaks can present<br />
hours after the procedure with pain, fever and<br />
leukocytosis<br />
• Other findings:<br />
• Gas in the portal system<br />
• Pneumothorax<br />
• Pneumomediastinum<br />
• Pneumoretroperitoneum<br />
• Pneumoperitoneum<br />
• Subcutaneous emphysema
www.downst<strong>at</strong>esurgery.org<br />
Diagnosis- Abdominal CT<br />
• Should be obtained in p<strong>at</strong>ients suspected <strong>of</strong><br />
having a perfor<strong>at</strong>ion even if no evidence <strong>of</strong><br />
retroperitoneal air on plain films<br />
• CT is the most sensitive means <strong>of</strong> detecting<br />
perfor<strong>at</strong>ion
www.downst<strong>at</strong>esurgery.org<br />
Diagnosis- Abdominal CT<br />
• The clinical or radiographic amount <strong>of</strong> air:<br />
• Not always indic<strong>at</strong>es the size <strong>of</strong> the<br />
perfor<strong>at</strong>ion<br />
• Not always correl<strong>at</strong>es with the severity <strong>of</strong><br />
the complic<strong>at</strong>ion<br />
• The amount <strong>of</strong> air reflects the degree <strong>of</strong><br />
manipul<strong>at</strong>ion after the perfor<strong>at</strong>ion occurred
www.downst<strong>at</strong>esurgery.org<br />
Retroperitoneal Air<br />
• Typically associ<strong>at</strong>ed with perfor<strong>at</strong>ion<br />
• However, may develop in clinically<br />
asymptom<strong>at</strong>ic p<strong>at</strong>ients following<br />
sphincterotomy<br />
• These p<strong>at</strong>ients may not require intervention
www.downst<strong>at</strong>esurgery.org<br />
Retroperitoneal Air<br />
• Origin <strong>of</strong> retroperitoneal air in asymptom<strong>at</strong>ic<br />
p<strong>at</strong>ients:<br />
• Rel<strong>at</strong>ed to dissection through an injured or<br />
intact bowel (similar to th<strong>at</strong> described after<br />
colonoscopy)<br />
• Sealed microperfor<strong>at</strong>ions<br />
• Presence <strong>of</strong> retroperitoneal air in the absence <strong>of</strong><br />
symptoms should warrant careful observ<strong>at</strong>ion<br />
but may not require intervention
www.downst<strong>at</strong>esurgery.org<br />
Grading Post-ERCP Perfor<strong>at</strong>ion<br />
• Mild: Possible, or only very slight leak <strong>of</strong> fluid or<br />
contrast, tre<strong>at</strong>able by fluids and suction for three<br />
days or less<br />
• Moder<strong>at</strong>e: Any definite perfor<strong>at</strong>ion tre<strong>at</strong>ed<br />
medically for 4 to 10 days<br />
• Severe: Medical tre<strong>at</strong>ment for more than 10<br />
days or intervention (percutaneous or surgical)<br />
Cotton et al. Endoscopic sphincterotomy complic<strong>at</strong>ions and their management: an <strong>at</strong>tempt <strong>at</strong> consensus. Gastrointest Endosc<br />
1991; 37:383
www.downst<strong>at</strong>esurgery.org<br />
Clasific<strong>at</strong>ion Post-ERCP<br />
Perfor<strong>at</strong>ion<br />
• Coded in descending order <strong>of</strong> injury severity<br />
• Correl<strong>at</strong>es with the mechanism <strong>of</strong> injury and<br />
the an<strong>at</strong>omic loc<strong>at</strong>ion <strong>of</strong> damage<br />
• Used as a predictor for the need for surgical<br />
intervention<br />
• Graded from Type I-IV<br />
Miller et al. Perfor<strong>at</strong>ions following endoscopic retrograde cholangiopancre<strong>at</strong>ography: a single institution experience and<br />
surgical recommend<strong>at</strong>ions. Am J Surg. 2013 Aug;206(2):180-6
www.downst<strong>at</strong>esurgery.org<br />
Clasific<strong>at</strong>ion Post-ERCP<br />
Perfor<strong>at</strong>ion<br />
• Type I:<br />
• L<strong>at</strong>eral or the medial duodenal wall remote from the ampulla<br />
• Caused by acute angul<strong>at</strong>ion <strong>of</strong> the endoscope<br />
• Typically large with extensive contrast leakage<br />
• Requires immedi<strong>at</strong>e surgery<br />
• Type II:<br />
• Peri-V<strong>at</strong>erian<br />
• Variable in their severity<br />
• Consequent to a precut sphincterotomy or occurring near a<br />
periampullary diverticulum<br />
• Minimal or moder<strong>at</strong>e contrast leakage<br />
• Some may be able to be managed conserv<strong>at</strong>ively<br />
Miller et al. Perfor<strong>at</strong>ions following endoscopic retrograde cholangiopancre<strong>at</strong>ography: a single institution experience and<br />
surgical recommend<strong>at</strong>ions. Am J Surg. 2013 Aug;206(2):180-6
• Type III<br />
• Distal CBD<br />
www.downst<strong>at</strong>esurgery.org<br />
Clasific<strong>at</strong>ion Post-ERCP<br />
Perfor<strong>at</strong>ion<br />
• Secondary to wire manipul<strong>at</strong>ion or basket instrument<strong>at</strong>ion during<br />
stone retrieval<br />
• Often small and localized and may frequently be managed<br />
conserv<strong>at</strong>ively<br />
• Type IV<br />
• Reveal retroperitoneal air and result from insuffl<strong>at</strong>ion during ERCP<br />
• Typically managed nonoper<strong>at</strong>ively<br />
Miller et al. Perfor<strong>at</strong>ions following endoscopic retrograde cholangiopancre<strong>at</strong>ography: a single institution experience and<br />
surgical recommend<strong>at</strong>ions. Am J Surg. 2013 Aug;206(2):180-6
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
Management<br />
• Free abdominal duodenal perfor<strong>at</strong>ions usually<br />
require surgery<br />
• Conserv<strong>at</strong>ive approach to retroperitoneal<br />
perfor<strong>at</strong>ion following sphincterotomy has been<br />
adopted<br />
• Early surgical consult<strong>at</strong>ion and careful<br />
observ<strong>at</strong>ion is mand<strong>at</strong>ory<br />
• Outcome poor in p<strong>at</strong>ients who do not receive prompt and<br />
appropri<strong>at</strong>e tre<strong>at</strong>ment
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
• Endoscopic Therapy:<br />
• Endoclips<br />
• Over the scope clips<br />
• Fibrin glue<br />
• Covered stents<br />
• Nasobiliary tube<br />
Management<br />
• Percutaneous transhep<strong>at</strong>ic drainage
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
Management<br />
• NPO, IV hydr<strong>at</strong>ion, NG or nasoduodenal suction,<br />
IV antibiotics<br />
• Consider percutaneous drainage as altern<strong>at</strong>ive<br />
to surgical drainage <strong>of</strong> retroperitoneal collections<br />
• TPN if NPO st<strong>at</strong>us expected for more than one<br />
week
• <strong>Surgery</strong> if:<br />
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
Management<br />
• Persistent biliary obstruction, cholangitis, and<br />
if no improvement after brief nonoper<strong>at</strong>ive<br />
management<br />
• Overall surgery is required in 20 to 40 percent <strong>of</strong><br />
p<strong>at</strong>ients with perfor<strong>at</strong>ion<br />
• Type <strong>of</strong> surgical intervention depends upon<br />
clinicop<strong>at</strong>hological condition
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
Management<br />
• Simple Repair<br />
• Tube decompression<br />
– Gastrostomy<br />
– Duodenostomy<br />
– Feeding Jejunostomy<br />
• Serosal P<strong>at</strong>ch<br />
• <strong>Duodenal</strong> Diverticuliz<strong>at</strong>ion<br />
• Pyloric exclusion
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
Management<br />
• Prognosis <strong>of</strong> p<strong>at</strong>ients with a perfor<strong>at</strong>ion<br />
depends upon<br />
• Rapidity <strong>of</strong> diagnosis<br />
• Clinical setting<br />
• P<strong>at</strong>ient comorbidities
www.downst<strong>at</strong>esurgery.org<br />
Post-ERCP Perfor<strong>at</strong>ion<br />
Management<br />
• Overall mortality has decreased from 16% percent in<br />
older reports to 8% in a review th<strong>at</strong> considered major<br />
studies from the year 2000<br />
• Lower mortality noted in recent years may reflect<br />
benefits rel<strong>at</strong>ed to a conserv<strong>at</strong>ive team approach to<br />
the management <strong>of</strong> small retroperitoneal perfor<strong>at</strong>ions<br />
Machado NO. Management <strong>of</strong> duodenal perfor<strong>at</strong>ion post-endoscopic retrograde cholangiopancre<strong>at</strong>ography. When and whom to<br />
oper<strong>at</strong>e and wh<strong>at</strong> factors determine the outcome? A review article. JOP 2012; 13:18
www.downst<strong>at</strong>esurgery.org<br />
Management <strong>of</strong> endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions<br />
Dimitrios V. Avgerinos, Omar H. Llaguna, Andrew Y. Lo, Joseph Voli, I. Michael Leitman<br />
Surg Endosc (2009) 23:833–838<br />
• A retrospective review <strong>of</strong> ERCP-rel<strong>at</strong>ed<br />
perfor<strong>at</strong>ions to the duodenum (April 1999 to<br />
February 2008)<br />
• Incidence, Clinical outcomes<br />
• D<strong>at</strong>a included: ERCP indic<strong>at</strong>ion, Clinical<br />
present<strong>at</strong>ion, Diagnostic methods, Time to<br />
diagnosis and tre<strong>at</strong>ment, Type <strong>of</strong> injury,<br />
Management
www.downst<strong>at</strong>esurgery.org<br />
Management <strong>of</strong> endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions<br />
Dimitrios V. Avgerinos, Omar H. Llaguna, Andrew Y. Lo, Joseph Voli, I. Michael Leitman<br />
Surg Endosc (2009) 23:833–838<br />
• 4,358 ERCP<br />
• 15 (0.34%) resulted in perfor<strong>at</strong>ion to the<br />
duodenum<br />
• 4 <strong>of</strong> the perfor<strong>at</strong>ions were discovered during<br />
ERCP<br />
• 8 required CT abdomen or abdominal<br />
radiography<br />
• <strong>Surgery</strong> was performed for 13 (87%) p<strong>at</strong>ients<br />
• 2 p<strong>at</strong>ients died (15%)
www.downst<strong>at</strong>esurgery.org<br />
Management <strong>of</strong> endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions<br />
Dimitrios V. Avgerinos, Omar H. Llaguna, Andrew Y. Lo, Joseph Voli, I. Michael Leitman<br />
Surg Endosc (2009) 23:833–838<br />
• One p<strong>at</strong>ient was managed conserv<strong>at</strong>ively with a<br />
successful outcome<br />
• 9 p<strong>at</strong>ients underwent surgery within 24 h after the<br />
ERCP<br />
• 1 p<strong>at</strong>ient underwent surgery after 24 h<br />
• The overall mortality r<strong>at</strong>e was 20% (3 <strong>of</strong> 15<br />
p<strong>at</strong>ients)
www.downst<strong>at</strong>esurgery.org<br />
Management <strong>of</strong> endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions<br />
Dimitrios V. Avgerinos, Omar H. Llaguna, Andrew Y. Lo, Joseph Voli, I. Michael Leitman<br />
Surg Endosc (2009) 23:833–838<br />
• The interval between the perfor<strong>at</strong>ion and the oper<strong>at</strong>ion is<br />
<strong>of</strong> gre<strong>at</strong> significance<br />
• The mortality r<strong>at</strong>e increases dram<strong>at</strong>ically with l<strong>at</strong>e<br />
surgical management (>24 hours)<br />
• Clinical and radiographic fe<strong>at</strong>ures can be used to<br />
determine the surgical or conserv<strong>at</strong>ive tre<strong>at</strong>ment <strong>of</strong><br />
ERCP-rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions<br />
• P<strong>at</strong>ient age and intraoper<strong>at</strong>ive findings can determined<br />
the final outcome and morbidity or mortality
www.downst<strong>at</strong>esurgery.org<br />
Management <strong>of</strong> endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions<br />
Dimitrios V. Avgerinos, Omar H. Llaguna, Andrew Y. Lo, Joseph Voli, I. Michael Leitman<br />
Surg Endosc (2009) 23:833–838
www.downst<strong>at</strong>esurgery.org<br />
Perfor<strong>at</strong>ions following endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: a single institution experience<br />
and surgical recommend<strong>at</strong>ions<br />
Rafi Miller, M.D. ,Andrew Zbar, M.D.. Yoram Klein, M.D., Victor Buyeviz, M.D., Ehud<br />
Melzer, M.D., Bruce N. Mosenkis, M.D., Eli Mavor, M.D.<br />
The American Journal <strong>of</strong> <strong>Surgery</strong> (2013) 206, 180-186<br />
• Records <strong>of</strong> p<strong>at</strong>ients undergoing ERCP 16-year period<br />
(1995-2011)<br />
• Types <strong>of</strong> injuries, diagnosis, management, and p<strong>at</strong>ient<br />
outcome<br />
• <strong>Injuries</strong> classified from I to IV<br />
• 1,638 ERCP<br />
• 27 perfor<strong>at</strong>ions (1.6%)<br />
• Nearly 50% <strong>of</strong> the procedures were regarded as difficult
www.downst<strong>at</strong>esurgery.org<br />
Perfor<strong>at</strong>ions following endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: a single institution experience<br />
and surgical recommend<strong>at</strong>ions<br />
Rafi Miller, M.D. ,Andrew Zbar, M.D.. Yoram Klein, M.D., Victor Buyeviz, M.D., Ehud<br />
Melzer, M.D., Bruce N. Mosenkis, M.D., Eli Mavor, M.D.<br />
The American Journal <strong>of</strong> <strong>Surgery</strong> (2013) 206, 180-186<br />
• 70% performed for therapeutic indic<strong>at</strong>ions.<br />
• 5 type I, 12 type II, 5 type III, 5 type IV perfor<strong>at</strong>ions<br />
• 18 cases diagnosed <strong>at</strong> the time <strong>of</strong> ERCP<br />
• Delayed diagnosis <strong>of</strong> type I perfor<strong>at</strong>ions were f<strong>at</strong>al<br />
• Most type II perfor<strong>at</strong>ions required immedi<strong>at</strong>e surgery with<br />
pyloric exclusion<br />
• Delayed surgery with simple drainage had a high mortality<br />
r<strong>at</strong>e<br />
• Most type III and type IV injuries can successfully be<br />
managed conserv<strong>at</strong>ively
www.downst<strong>at</strong>esurgery.org<br />
Perfor<strong>at</strong>ions following endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: a single institution experience<br />
and surgical recommend<strong>at</strong>ions<br />
Rafi Miller, M.D. ,Andrew Zbar, M.D.. Yoram Klein, M.D., Victor Buyeviz, M.D., Ehud<br />
Melzer, M.D., Bruce N. Mosenkis, M.D., Eli Mavor, M.D.<br />
The American Journal <strong>of</strong> <strong>Surgery</strong> (2013) 206, 180-186<br />
• The mechanism <strong>of</strong> injury during ERCP predicts the<br />
need for surgical management<br />
• Type I and type II injuries require early diagnosis<br />
and aggressive surgery<br />
• Type III and type IV injuries may be managed<br />
conserv<strong>at</strong>ively
www.downst<strong>at</strong>esurgery.org<br />
Perfor<strong>at</strong>ions following endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography: a single institution experience<br />
and surgical recommend<strong>at</strong>ions<br />
Rafi Miller, M.D. ,Andrew Zbar, M.D.. Yoram Klein, M.D., Victor Buyeviz, M.D., Ehud<br />
Melzer, M.D., Bruce N. Mosenkis, M.D., Eli Mavor, M.D.<br />
The American Journal <strong>of</strong> <strong>Surgery</strong> (2013) 206, 180-186
www.downst<strong>at</strong>esurgery.org<br />
Summary<br />
• Retroduodenal perfor<strong>at</strong>ion has decreased<br />
from up to 2.1 percent <strong>of</strong> sphincterotomies to<br />
less than 0.5 percent in recent series<br />
• Free abdominal perfor<strong>at</strong>ion is almost always<br />
recognized immedi<strong>at</strong>ely based upon clinical<br />
symptoms, physical signs, and fluoroscopic<br />
findings
www.downst<strong>at</strong>esurgery.org<br />
Summary<br />
• Retroduodenal perfor<strong>at</strong>ion is usually<br />
determined by the radiologic evidence <strong>of</strong> air<br />
or contrast in the retroperitoneal space<br />
• Retroperitoneal air may also develop following<br />
sphincterotomy in p<strong>at</strong>ients who are clinically<br />
asymptom<strong>at</strong>ic. Such p<strong>at</strong>ients may not require<br />
intervention
www.downst<strong>at</strong>esurgery.org<br />
Summary<br />
• Abdominal CT scan should be obtained in<br />
p<strong>at</strong>ients who are suspected <strong>of</strong> having a<br />
perfor<strong>at</strong>ion. CT scan is the most sensitive<br />
means for detecting perfor<strong>at</strong>ion<br />
• P<strong>at</strong>ients with free abdominal duodenal<br />
perfor<strong>at</strong>ion usually require surgery
www.downst<strong>at</strong>esurgery.org<br />
Summary<br />
• By contrast, a conserv<strong>at</strong>ive approach to small<br />
retroperitoneal perfor<strong>at</strong>ion may be<br />
appropri<strong>at</strong>e<br />
• Early surgical consult<strong>at</strong>ion and careful<br />
observ<strong>at</strong>ion is mand<strong>at</strong>ory since the outcome<br />
may be poor in p<strong>at</strong>ients who do not receive<br />
prompt and appropri<strong>at</strong>e tre<strong>at</strong>ment
www.downst<strong>at</strong>esurgery.org<br />
References<br />
1. Proposal <strong>of</strong> an endoscopic retrograde cholangiopancre<strong>at</strong>ography-rel<strong>at</strong>ed perfor<strong>at</strong>ion management<br />
guideline based on perfor<strong>at</strong>ion type. Kwon W, Jang J, Ryu J, Kim Y, Yoon Y, Kang M, Kim S. J Korean<br />
Surg Soc 2012;83:218-226<br />
2. Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complic<strong>at</strong>ions and their<br />
management: an <strong>at</strong>tempt <strong>at</strong> consensus. Gastrointest Endosc 1991; 37:383<br />
3. Machado NO. Management <strong>of</strong> duodenal perfor<strong>at</strong>ion post-endoscopic retrograde<br />
cholangiopancre<strong>at</strong>ography. When and whom to oper<strong>at</strong>e and wh<strong>at</strong> factors determine the outcome? A<br />
review article. JOP 2012; 13:18<br />
4. Miller R, Zbar A, Klein Y, Buyeviz V, Melzer E, Mosenkis BN, Mavor E. Perfor<strong>at</strong>ions following<br />
endoscopic retrograde cholangiopancre<strong>at</strong>ography: a single institution experience and surgical<br />
recommend<strong>at</strong>ions. Am J Surg. 2013 Aug;206(2):180-6<br />
5. Loperfido S et al. Post-ERCP perfor<strong>at</strong>ion. In: UpToD<strong>at</strong>e, Basow, DS (Ed), UpToD<strong>at</strong>e, Waltham, MA,<br />
2013<br />
6. Dimitrios V. Avgerinos, Omar H. Llaguna, Andrew Y. Lo, Joseph Voli, I. Michael Leitman. Management<br />
<strong>of</strong> endoscopic retrograde cholangiopancre<strong>at</strong>ography: rel<strong>at</strong>ed duodenal perfor<strong>at</strong>ions. Surg Endosc<br />
(2009) 23:833–838














