Bending the Curve? Implications for Anesthesia - The University of ...
Bending the Curve? Implications for Anesthesia - The University of ...
Bending the Curve? Implications for Anesthesia - The University of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
THE DEPARTMENT OF<br />
ANESTHESIOLOGY AT<br />
THE UNIVERSITY OF<br />
TENNESEEE IN<br />
KNOXVILLE<br />
FEATURES<br />
<strong>Curve</strong> 1<br />
Class <strong>of</strong> 2011 2<br />
ASAPAC 2<br />
Class <strong>of</strong> 2013 3<br />
2011 ASA 4<br />
2011 IARS 4<br />
Man Run 5<br />
Awards 6<br />
NAC 7<br />
LIfe 8—11<br />
Research<br />
12<br />
Bagley 12<br />
Teaching 13<br />
Brutane<br />
V O L U M E 1 , I S S U E 3<br />
National Debt<br />
<strong>The</strong> “cloud <strong>of</strong> doom” <strong>of</strong> an an‐<br />
nual federal deficit exceeding $2<br />
trillion per year <strong>for</strong> <strong>the</strong> <strong>for</strong>esee‐<br />
able future has caused <strong>the</strong> na‐<br />
tion and, hopefully, Congress<br />
and <strong>the</strong><br />
Administra‐<br />
tion to take<br />
a hard look<br />
at where<br />
our nation<br />
spends <strong>the</strong><br />
taxpayer’s<br />
money. <strong>The</strong><br />
primary<br />
areas <strong>of</strong><br />
focus re‐<br />
main Social<br />
Security,<br />
Medicare /<br />
Medicaid,<br />
defense /<br />
war spending, and interest pay‐<br />
ments on <strong>the</strong> national debt.<br />
While it is true that <strong>the</strong> deficit<br />
could be reduced by limiting<br />
“discretionary spending,” Sut‐<br />
ton’s law remains true to this<br />
day. Willie Sutton, <strong>the</strong> infamous<br />
bank robber when asked why he<br />
robbed banks stated, "because<br />
that's where <strong>the</strong> money is". <strong>The</strong><br />
funded and under‐funded enti‐<br />
tlement programs such as Medi‐<br />
care and Medicaid on which so<br />
many Americans have come to<br />
depend remain one <strong>of</strong> <strong>the</strong> pri‐<br />
mary targets <strong>for</strong> deficit reduc‐<br />
tion.<br />
Health Care Spending and <strong>the</strong><br />
GDP<br />
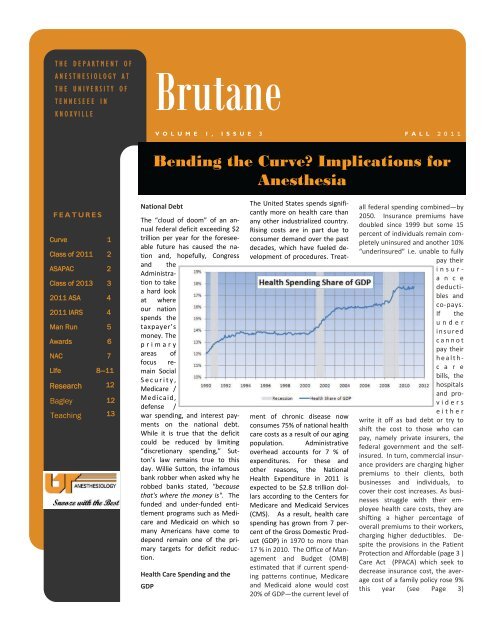
<strong>The</strong> United States spends signifi‐<br />
cantly more on health care than<br />
any o<strong>the</strong>r industrialized country.<br />
Rising costs are in part due to<br />
consumer demand over <strong>the</strong> past<br />
decades, which have fueled de‐<br />
velopment <strong>of</strong> procedures. Treat‐<br />
ment <strong>of</strong> chronic disease now<br />
consumes 75% <strong>of</strong> national health<br />
care costs as a result <strong>of</strong> our aging<br />
population. Administrative<br />
overhead accounts <strong>for</strong> 7 % <strong>of</strong><br />
expenditures. For <strong>the</strong>se and<br />
o<strong>the</strong>r reasons, <strong>the</strong> National<br />
Health Expenditure in 2011 is<br />
expected to be $2.8 trillion dol‐<br />
lars according to <strong>the</strong> Centers <strong>for</strong><br />
Medicare and Medicaid Services<br />
(CMS). As a result, health care<br />
spending has grown from 7 per‐<br />
cent <strong>of</strong> <strong>the</strong> Gross Domestic Prod‐<br />
uct (GDP) in 1970 to more than<br />
17 % in 2010. <strong>The</strong> Office <strong>of</strong> Man‐<br />
agement and Budget (OMB)<br />
estimated that if current spend‐<br />
ing patterns continue, Medicare<br />
and Medicaid alone would cost<br />
20% <strong>of</strong> GDP—<strong>the</strong> current level <strong>of</strong><br />
F A L L 2 0 1 1<br />
<strong>Bending</strong> <strong>the</strong> <strong>Curve</strong>? <strong>Implications</strong> <strong>for</strong><br />
Anes<strong>the</strong>sia<br />
all federal spending combined—by<br />
2050. Insurance premiums have<br />
doubled since 1999 but some 15<br />
percent <strong>of</strong> individuals remain com‐<br />
pletely uninsured and ano<strong>the</strong>r 10%<br />
“underinsured” i.e. unable to fully<br />
pay <strong>the</strong>ir<br />
insur‐<br />
a n c e<br />
deducti‐<br />
bles and<br />
co‐pays.<br />
If <strong>the</strong><br />
under<br />
insured<br />
cannot<br />
pay <strong>the</strong>ir<br />
health‐<br />
c a r e<br />
bills, <strong>the</strong><br />
hospitals<br />
and pro‐<br />
viders<br />
ei<strong>the</strong>r<br />
write it <strong>of</strong>f as bad debt or try to<br />
shift <strong>the</strong> cost to those who can<br />
pay, namely private insurers, <strong>the</strong><br />
federal government and <strong>the</strong> self‐<br />
insured. In turn, commercial insur‐<br />
ance providers are charging higher<br />
premiums to <strong>the</strong>ir clients, both<br />
businesses and individuals, to<br />
cover <strong>the</strong>ir cost increases. As busi‐<br />
nesses struggle with <strong>the</strong>ir em‐<br />
ployee health care costs, <strong>the</strong>y are<br />
shifting a higher percentage <strong>of</strong><br />
overall premiums to <strong>the</strong>ir workers,<br />
charging higher deductibles. De‐<br />
spite <strong>the</strong> provisions in <strong>the</strong> Patient<br />
Protection and Af<strong>for</strong>dable (page 3 )<br />
Care Act (PPACA) which seek to<br />
decrease insurance cost, <strong>the</strong> aver‐<br />
age cost <strong>of</strong> a family policy rose 9%<br />
this year (see Page 3)
PAGE 2<br />
“Well…….I’m not sure<br />
that I would have done<br />
that!!!!<br />
Rocuronium-<br />
cyclodextrincom- plex<br />
BRUTANE<br />
Adios Class <strong>of</strong> 2011<br />
<strong>The</strong> following residents graduated from <strong>the</strong> <strong>University</strong> <strong>of</strong> Tennessee Department <strong>of</strong> Anes<strong>the</strong>siology<br />
in 2011: Carrie Francisco, Michael Godbold, John Gold, Robert McGee, Brigitte Messenger, and<br />
Wayne Smith. Three <strong>of</strong> our <strong>for</strong>mer residents are practicing anes<strong>the</strong>siology in Tennessee, Drs. McIlrath,<br />
Smith and Messenger. Wayne is in private practice in Johnson City while Brigitte has joined<br />
<strong>University</strong> Anes<strong>the</strong>siologists and will be completing a fellowship in Cardiac Anes<strong>the</strong>sia at Vanderbilt.<br />
Tim joined several <strong>of</strong> our <strong>for</strong>mer residents in private practice at ParkWest in Knoxville. Carrie,<br />
Robert and John returned “home” to Richmond, VA ; Indianapolis, IN and Savannah, GA. Michael<br />
elected to fur<strong>the</strong>r his education as fellow in Pediatric Anes<strong>the</strong>sia at Emory <strong>University</strong>. <strong>The</strong> Department<br />
<strong>of</strong> Anes<strong>the</strong>siology is very proud <strong>of</strong> <strong>the</strong>se graduates and <strong>the</strong>ir accomplishments!!!!!<br />
Last year <strong>the</strong> Residents and Faculty <strong>of</strong> <strong>the</strong> Department <strong>of</strong> Anes‐<br />
<strong>the</strong>siology <strong>of</strong> <strong>the</strong> <strong>University</strong> <strong>of</strong> Tennessee set a milestone that<br />
many thought was unreachable, namely 100% participation in<br />
contributions to <strong>the</strong> ASAPAC. Once again, <strong>the</strong> Department<br />
reached this goal and was joined by <strong>the</strong> <strong>University</strong> <strong>of</strong> Miami and<br />
<strong>the</strong> <strong>University</strong> <strong>of</strong> Chicago in this accomplishment.
PAGE 3<br />
“Well…….I’m not sure<br />
that I would have done<br />
that!!!!<br />
Rocuronium-<br />
cyclodextrincom- plex<br />
BRUTANE<br />
(from Page 1) exceeding $15,000 ‐‐‐ that's <strong>the</strong> largest increase<br />
in cost in 6 years.<br />
PPACA<br />
<strong>The</strong> Patient Protection and Af<strong>for</strong>dable Care Act, (PPACA) was<br />
signed into law by President Obama on March 23, 2010. <strong>The</strong><br />
complex law expands coverage with insurance market man‐<br />
dates: beginning in 2014 and bars insurance companies from<br />
denying coverage based on preexisting medical condi‐<br />
tions. <strong>The</strong> act also requires citizens to purchase federally ap‐<br />
proved insurance or pay a fine, with <strong>the</strong> goal <strong>of</strong> maintaining a<br />
financially sustainable risk pool <strong>for</strong> insurance firms. PPACA<br />
increases af<strong>for</strong>dability through almost $1 trillion in subsidies<br />
over 10 years to fund state‐level health insurance exchanges<br />
and expand Medicaid programs. By 2014, each state will have<br />
created an exchange in which families and employers can pur‐<br />
chase private insurance plans that comply with federal guide‐<br />
lines. <strong>The</strong> federal government will provide refundable ‘tax<br />
credits’ to families below 400% <strong>of</strong> <strong>the</strong> national poverty line.<br />
<strong>The</strong> Congressional Budget Office estimates that <strong>the</strong> exchanges<br />
will extend coverage to 24 million Americans. By 2014, indi‐<br />
viduals not eligible <strong>for</strong> Medicare with incomes below 133 per‐<br />
cent <strong>of</strong> <strong>the</strong> poverty level will be eligible <strong>for</strong> Medicaid, which<br />
will cover ano<strong>the</strong>r 16 million citizens.<br />
Who Pays <strong>for</strong> <strong>the</strong> Expansion?<br />
<strong>The</strong> PPCA will pay <strong>for</strong> @ one‐half <strong>of</strong> this expansion in coverage<br />
through new taxes. An excise tax on high‐cost “Cadillac”<br />
health plans which begins in 2018 is projected to raise $32<br />
billion through 2019. An annual fee on health care providers<br />
will raise $60 billion, and surcharges on individuals earning<br />
over $200,000 annually will raise $210 billion. <strong>The</strong>se and o<strong>the</strong>r<br />
taxes are planned to generate $410 billion through 2019. <strong>The</strong><br />
rest <strong>of</strong> <strong>the</strong> cost is covered by reductions in Medicare reim‐<br />
bursements to care providers, reducing spending by $491 bil‐<br />
lion through 2019. O<strong>the</strong>r pilot programs <strong>of</strong> unproven success<br />
are also counted on to decrease cost such as investments in<br />
medical in<strong>for</strong>mation technology and penalties <strong>for</strong> hospitals<br />
with high readmissions regardless <strong>of</strong> <strong>the</strong> cause <strong>of</strong> readmission<br />
after discharge.<br />
IPAB<br />
<strong>The</strong> PPCA established an Independent Payment Advisory Board<br />
(IPAB) with <strong>the</strong> explicit task <strong>of</strong> reducing <strong>the</strong> rate <strong>of</strong> growth in<br />
Medicare without affecting coverage or quality. Under previ‐<br />
ous law, changes to Medicare reimbursement rates were rec‐<br />
Welcome to <strong>the</strong> Class <strong>of</strong> 2014<br />
ommended by MedPac but required an Act <strong>of</strong><br />
Congress to take effect. Now <strong>the</strong> IPAB will deter‐<br />
mine reimbursement rates and an Act <strong>of</strong> Congress<br />
will be needed to overturn <strong>the</strong> decisions made.<br />
Impact <strong>of</strong> IPAB & PPACA on Payment <strong>of</strong> Anes<strong>the</strong>‐<br />
sia Services<br />
As documented by <strong>the</strong> Government Accountability<br />
Office, Medicare payments to anes<strong>the</strong>sia providers<br />
falls at @ 33 cents to <strong>the</strong> dollar as opposed to 80<br />
cents to <strong>the</strong> dollar <strong>for</strong> o<strong>the</strong>r specialties. <strong>The</strong> perils<br />
to anes<strong>the</strong>sia providers becomes readily apparent<br />
when <strong>the</strong> aging population, <strong>the</strong> expansion <strong>of</strong><br />
Medicaid (whose payments to anes<strong>the</strong>sia provid‐<br />
ers are two‐thirds <strong>of</strong> <strong>the</strong> Medicare rate in Tennes‐<br />
see), and payment <strong>for</strong> <strong>the</strong> PPCA through reduc‐<br />
tions in Medicare payments to as well as an annual<br />
fee on health care providers are considered. Most<br />
physician specialty groups have voiced opposition<br />
to <strong>the</strong> Sustainable Growth Rate <strong>for</strong>mula that was<br />
intended to limit <strong>the</strong> increases in Medicare spend‐<br />
ing. <strong>The</strong> PPACA wrapped one <strong>for</strong>mula inside <strong>the</strong><br />
o<strong>the</strong>r, meaning that if <strong>for</strong> any given year starting in<br />
2014 going <strong>for</strong>ward <strong>the</strong> rate <strong>of</strong> Medicare growth is<br />
lower than <strong>the</strong> SGR cut, <strong>the</strong>n <strong>the</strong> SGR cut would<br />
apply. In <strong>the</strong> past, Congress has passed last‐<br />
minute legislation to <strong>of</strong>f‐set <strong>the</strong> mandated SGR<br />
decreases in provider payments. Remember that<br />
@ ½ <strong>of</strong> <strong>the</strong> financing <strong>for</strong> <strong>the</strong> PPACA comes in man‐<br />
datory cuts in Medicare payments to providers. If<br />
<strong>the</strong> cut mandated by <strong>the</strong> PPACA law under <strong>the</strong><br />
IPAB mechanism exceeds <strong>the</strong> cuts required by <strong>the</strong><br />
SGR <strong>for</strong>mula, <strong>the</strong>n this new Independent Board<br />
must recommend cuts to reach <strong>the</strong> statutorily<br />
stated target to reduce Medicare spending. No<br />
discretion in <strong>the</strong> PPACA law exists and, even if<br />
Congress were to intervene, our legislative body<br />
must do so during a narrow 60‐day review period.<br />
As a result, most physician groups particularly<br />
anes<strong>the</strong>sia providers are dedicated to IPAB repeal<br />
and re<strong>for</strong>m.<br />
<strong>The</strong> Department <strong>of</strong> Anes<strong>the</strong>siology would like to welcome <strong>the</strong> Class <strong>of</strong> 2014 who started <strong>the</strong>ir residency in July<br />
2011. <strong>The</strong> members include: Brian Adams (Indiana <strong>University</strong> School <strong>of</strong> Medicine), David Dahl (East Tennessee<br />
State <strong>University</strong>), Mary Ellen Graham (), Melissa House (Indiana <strong>University</strong> School <strong>of</strong> Medicine), Benton Pitkanen<br />
(<strong>University</strong> <strong>of</strong> Tennessee), Zachary Rose (Wake Forest) and Christopher Strock (<strong>University</strong> <strong>of</strong> South<br />
Florida).
Dr. Patteson<br />
PAGE 4<br />
Rocuronium-<br />
cyclodextrincom- plex<br />
Drs. Bustamante & McIlrath<br />
Drs. Messenger & Craft<br />
BRUTANE<br />
Several members <strong>of</strong> <strong>the</strong> Department <strong>of</strong> Anes<strong>the</strong>siology<br />
were active participants in <strong>the</strong> Annual Meeting<br />
<strong>of</strong> <strong>the</strong> American Society <strong>of</strong> Anes<strong>the</strong>siology held in<br />
Chicago from October 15—19, 2011. Dr. Kip Robinson<br />
again led two ‘sold-out’ Problem Based Learning<br />
Sessions about <strong>the</strong> “<strong>The</strong> Irregular Patient: Atrial<br />
Fibrillation in <strong>the</strong> Perioperative Setting”. Dr. Russ<br />
Langdon served as an abstract moderator <strong>for</strong> sessions<br />
in Clinical Neuroscience and Critical Care.<br />
Several residents and faculty were featured in <strong>the</strong><br />
Medically Challenging Cases section: “Management<br />
<strong>of</strong> Unanticipated Airway Obstruction during Bronchoscopy”.<br />
S. K. Patteson ,B. Messenger and N. Doi-<br />
ron; “Common Variable Immunodeficiency Disorder in<br />
a Trauma Patient Undergoing Massive Transfusion”. C.<br />
L. Greene and D. R. Bustamante; ”A Difficult Airway in a<br />
Patient with Moebius Syndrome and Gingiva Hyperplasia”.<br />
M. Kimball and R. Craft; “Critical Intrathoracic<br />
Tracheal Stenosis Treated by Vascular Balloon Dilatation”.<br />
L. M. Pittman, W. Smith and R. Craft; “Urgent<br />
Surgery with Acute Anterior MI on EKG”; S. M. Strevels.<br />
Our Department and state were also well represented<br />
by two <strong>of</strong> our faculty, Dr. Eric Cox and Dr.<br />
Daniel Bustamante who served in <strong>the</strong> House <strong>of</strong> Delegates<br />
<strong>of</strong> <strong>the</strong> American Society <strong>of</strong> Anes<strong>the</strong>siologists.<br />
<strong>The</strong> Department <strong>of</strong> Anes<strong>the</strong>siology was well represented at <strong>the</strong> 2011 Annual Meeting <strong>of</strong> <strong>the</strong> International<br />
Anes<strong>the</strong>sia Research Society in Vancouver, British Columbia. Drs. Daniel Bustamante and Robert Craft again<br />
served as moderators <strong>for</strong> several academic sessions as well as <strong>the</strong> faculty sponsors <strong>of</strong> resident poster presentations<br />
such as: “Does a Consensus Exist in <strong>the</strong> Treatment <strong>of</strong> Peri-Operative Corneal Abrasions?” T. McILrath,<br />
J. Ollis & D. Bustamante; “Acute Encephalopathy in Parturient with TTP/HUS”. N. Dorion, R. Langdon;<br />
“TEG-Guided Massive Transfusion in Trauma Patients”. B. Messenger, R. Craft. “Malignant Hyper<strong>the</strong>rmia in a<br />
Patient with Pre-Existing Fever”. S. Patteson , M. Godbold.
VOLUME 1, ISSUE 3<br />
<strong>The</strong> Man Run 2011<br />
PAGE 5<br />
55 members <strong>of</strong> U. T. Anes<strong>the</strong>siology participated in <strong>the</strong> 4 th Annual Man Run 5K to raise awareness <strong>for</strong> Prostate Cancer. Team<br />
U. T. Anes<strong>the</strong>siology “smoked” <strong>the</strong> team competition in winning first place with a with a combined time <strong>of</strong> 1:22.04 beating 2nd<br />
place SunTrust by over 21 seconds. Special congratulations are in order <strong>for</strong> Bob Adam (husband <strong>of</strong> Lally Lehmann, MD) who<br />
repeated as <strong>the</strong> Overall Male Open Division winner with a time <strong>of</strong> 17:10. Lally Lehmann finished in first place in <strong>the</strong> 25 to 29<br />
age division. A special thanks to David Ratliff <strong>for</strong> his tireless ef<strong>for</strong>ts as <strong>the</strong> Captain <strong>of</strong> Team U. T. Anes<strong>the</strong>siology and who finished<br />
third in his age division (Older than Dirt) in a time <strong>of</strong> 24:58 .<br />
Overall winner, Bob Adams, with Lally<br />
Lehmann and Team Captain, Dave Ratliff
PAGE 6<br />
PAT Wins Award<br />
At <strong>the</strong> annual meeting <strong>of</strong> <strong>the</strong> Centricity Perioperative National<br />
User’ Group, GE healthcare named <strong>the</strong> Department <strong>of</strong> Anes-<br />
<strong>the</strong>siology at <strong>the</strong> <strong>University</strong> <strong>of</strong> Tennessee Medial center a<br />
winner <strong>of</strong> its 2011 Customer Innovation Award. <strong>The</strong> award,<br />
which recognizes a customer using GE’s perioperative tools<br />
to impact health outcomes or internal revenue stream in<br />
unique ways, was awarded to <strong>the</strong> Pre-Admission Testing Component<br />
to Centricity Perioperative Anes<strong>the</strong>sia in <strong>the</strong> category<br />
<strong>of</strong> Clinical Outcomes. Congratulations to Dr.<br />
Craft and Ms. Babis!!!!<br />
You are trying to correlate <strong>the</strong> amount <strong>of</strong> intra-operative fluid received<br />
with <strong>the</strong> later incidence <strong>of</strong> a surgical site infection (SSI). If you<br />
wanted to compare <strong>the</strong> mean intra-operative fluid received between<br />
<strong>the</strong> group <strong>of</strong> patients that developed a SSI (n = 101) and those that<br />
did not (n = 963), which test would you use if <strong>the</strong> groups were normally<br />
distributed? Choose <strong>the</strong> best answer. <strong>The</strong> answer and explanation<br />
are found on Page 11.<br />
A. Chi-squared test<br />
B. Fisher’s exact test<br />
C. Mann-Whitney U test<br />
D. Student’s t-test<br />
BRUTANE<br />
Sarah Nalle, a CRNA at <strong>the</strong> <strong>University</strong> <strong>of</strong> Tennessee recently received<br />
<strong>the</strong> “Excellence in Clinical Practice” Award from Sigma <strong>The</strong>ta Tau<br />
International (Honor Society <strong>of</strong> Nursing) <strong>for</strong> her outstanding contributions<br />
<strong>for</strong> promotion <strong>of</strong> high quality patient care. Congratulations and<br />
well deserved!!!<br />
Board Review<br />
UTMCK CRNA Honored<br />
Which <strong>of</strong> <strong>the</strong> following conditions would probably be present after 24<br />
hours <strong>of</strong> continued hyperventilation <strong>of</strong> an o<strong>the</strong>rwise normal patient?<br />
Choose <strong>the</strong> best answer. <strong>The</strong> answer and explanation are found on<br />
Page 11.<br />
A. PaCO2 < normal; CSF PCO2 < normal; CSF pH > normal;<br />
CBF < normal<br />
B. PaCO2 < normal; CSF PCO2 < normal; CSF pH > normal;<br />
CBF = normal<br />
C. PaCO2 < normal; CSF PCO2 < normal; CSF pH > normal;<br />
CBF = normal<br />
D. PaCO2 < normal; CSF PCO2 < normal; CSF pH = normal;<br />
CBF = normal<br />
E. PaCO2 = normal; CSF PCO2 = normal; CSF pH = normal;<br />
CBF = normal
PAGE 7<br />
Clinical Instructor <strong>of</strong><br />
<strong>the</strong> Year Award –<br />
Patrick McConville, MD<br />
Pr<strong>of</strong>essional Excellence<br />
– Catharine<br />
Hatcher & Angela<br />
McAmis<br />
Dr. John C. Preston<br />
Outstanding Graduate<br />
Award - Nell Smith<br />
BRUTANE<br />
CON Class <strong>of</strong> 2011<br />
Congratulations to <strong>the</strong> Class <strong>of</strong> 2011: Eric Atwood, Laura Black, Noelle Carter, Matt Clayton, Catharine<br />
Hatcher, Melissa Kelly, Angela McAmis, Jenny Palk, Allison Sheffey, Nell Smith, Shannon Still, Chad<br />
Tollett, Derrick White and Christy Woods. <strong>The</strong> Department <strong>of</strong> Anes<strong>the</strong>siology wishes you well in all <strong>of</strong><br />
your future endeavors! .<br />
Guatemala Medical Mission<br />
This past January, Noelle Carter, Angela<br />
McAmis and Shannurse<br />
anes<strong>the</strong>tists 2011<br />
non Still took part as student<br />
during a weeklong medical<br />
mission at <strong>the</strong> Obras Sociales Hermano<br />
Pedro Hospital and Orphanage in Antigua, Guatemala. <strong>The</strong> students provided anes<strong>the</strong>sia care as part<br />
<strong>of</strong> an anes<strong>the</strong>sia care team consisting <strong>of</strong> one anes<strong>the</strong>siologist, two CRNAs and our three SRNAs.<br />
<strong>The</strong>se volunteers provided general and monitored anes<strong>the</strong>sia care <strong>for</strong> <strong>of</strong> pediatric and (see page 13)<br />
Class <strong>of</strong> 2013: Welcome to <strong>the</strong> New SRNAs!!<br />
<strong>The</strong> Department <strong>of</strong> Anes<strong>the</strong>siology would like to<br />
welcome <strong>the</strong> following SRNAs to <strong>the</strong> <strong>University</strong> <strong>of</strong><br />
Tennessee Medical Center: Crystal Allen. Kaitlyn<br />
Boettcher, Andrea Bonnell. Kathy Foster, Maria<br />
Geswein, Jessica Kimball, Betsy Lee, Laura Long,<br />
Miranda Marsh, Phillip Reagan, Josh Rose, Bethany<br />
Seale, Tyson Summers, Darlyne Teran and<br />
Rachel White.
Caption<br />
describing<br />
picture or<br />
graphic.<br />
PAGE 10<br />
BRUTANE
VOLUME 1, ISSUE 3<br />
PAGE 11
PAGE 12<br />
BRUTANE<br />
Current Research Endeavors (See Page 14)<br />
�� TEG Screening <strong>of</strong> OBGYN Patients <strong>for</strong> Thrombotic Risk Jack J. Chavez, MD, Robert<br />
F. Elder, MD and Roger C. Carroll, PhD<br />
�� TEG (Thromboelastograph) Guided Transfusion <strong>for</strong> Trauma Patients Robert Craft, MD,<br />
Blaine Enderson, MD, Brigitte Messenger, MD, Roger Carroll, PhD<br />
�� Coagulation Pr<strong>of</strong>iles Using TEG (thromboelastograph) After Subarachnoid and<br />
Intraparenchymal Hemorrhages Russ Langdon, MD; Roger Carroll, Phd; Robert Craft, MD<br />
�� Bioimpedance <strong>for</strong> Identification <strong>of</strong> <strong>the</strong> Epidural Space Stephen K. Patteson, M.D.;<br />
Michael Doody, MD; Patrick McConville, MD; Mat<strong>the</strong>w Vance, MD; Crystal Greene, MD; Jeff Staack, MD;<br />
Lally Lehman, MD; Mark Murray, MD<br />
�� Measurement <strong>of</strong> Hemostasis by Thromboelastograph (TEG) during <strong>The</strong>rapeutic Hypo<strong>the</strong>r-<br />
mia After Cardiac Arrest Robert Craft, MD; Russ Langdon, MD; Roger Carroll, PhD, Tina Dudney,<br />
MD; Barry Faust, MD<br />
�� Epidural Fever Associated with Pyrogens Stephen K. Patteson M.D.<br />
�� Use <strong>of</strong> Ecarin Clotting Time (ECT) to Monitor Dabigatran (Pradaxa) <strong>The</strong>rapy Using<br />
Thromboelastograph® Roger Carroll, PhD; Robert Craft, MD, Dale Wortham, MD, Stuart Bresee, MD<br />
�� Validation <strong>of</strong> <strong>the</strong> RapidTEG MA Compared to Kaolin in Trauma Patients Robert Craft, MD;<br />
J Russ Langdon, MD, Roger Carroll, PhD, Brian Daley, MD<br />
�� An Outcome Comparison <strong>of</strong> Pacemaker Protocols Robert Craft, MD; N. Misulia<br />
�� Antihypertensive's Effect Upon Intraoperative Blood Pressure Variability Robert Craft,<br />
MD; Jason Buehler, MD<br />
�� PET Investigation <strong>of</strong> Anes<strong>the</strong>tic Effects on Progression <strong>of</strong> Alzheimer’s Disease in<br />
Mice Robert Craft, MD; Cody Rowan, MD<br />
�� Bioimpedance <strong>for</strong> Identification <strong>of</strong> <strong>the</strong> Intraperitoneal Space Stephen K. Patteson M.D.;<br />
Dr. Warren Bagley Memorial Clinical Excellence Award<br />
At <strong>the</strong> 2011 SRNA Graduation awards ceremony, <strong>the</strong> Clinical<br />
Excellence Award was presented to Allison Sheffey, <strong>the</strong> nurse<br />
anes<strong>the</strong>sia student who, in <strong>the</strong> opinion <strong>of</strong> clinical faculty, consistently<br />
demonstrated a superior level <strong>of</strong> clinical knowledge<br />
and expertise. <strong>The</strong> award was renamed as a memorial tribute
VOLUME 1, ISSUE 1<br />
Student's t-test is most commonly used to compare <strong>the</strong><br />
mean <strong>of</strong> two, normally distributed populations. <strong>The</strong> Chisquare<br />
test is typically employed to compare two (or more)<br />
proportions, as is Fisher's exact test. <strong>The</strong> Mann-Whitney test<br />
is a nonparametric test used to compare <strong>the</strong> mean <strong>of</strong> two<br />
populations that are NOT normally distributed.<br />
You are trying to correlate <strong>the</strong> amount <strong>of</strong> intraoperative<br />
fluid received with <strong>the</strong> later incidence <strong>of</strong> a<br />
surgical site infection (SSI). If you wanted to compare<br />
<strong>the</strong> mean intra-operative fluid received between <strong>the</strong><br />
group <strong>of</strong> patients that developed a SSI (n = 101) and<br />
those that did not (n = 963), which test would you use<br />
if <strong>the</strong> groups were normally distributed?<br />
A. Chi-squared test<br />
B. Fisher’s exact test<br />
C. Mann-Whitney U test<br />
D. Student’s t-test<br />
Board Review (See Page 6)<br />
Excellence in Teaching: Don Pearson, MD and Paddy McConville, MD<br />
<strong>The</strong> graduating anes<strong>the</strong>siology residents in <strong>the</strong> Class <strong>of</strong> 2010 awarded Dr.<br />
Russ Langdon and Dr. Jack Chavez <strong>the</strong> coveted “Excellence in Teaching”<br />
Award to <strong>the</strong> staff anes<strong>the</strong>siologist(s) who demonstrates great dedication,<br />
vast knowledge and immense skill in resident education. Our sincere congratulations<br />
to both <strong>of</strong> <strong>the</strong>m <strong>for</strong> <strong>the</strong>ir tireless ef<strong>for</strong>ts!!!<br />
PAGE 13<br />
After 24 hours <strong>of</strong> continuous hyperventilation, <strong>the</strong> patient’s<br />
PaCO2 would, by definition, be low. As <strong>the</strong> blood brain barrier<br />
(BBB) is freely permeable to CO2, <strong>the</strong> PCO2 <strong>of</strong> <strong>the</strong> CSF would also<br />
be low; however, <strong>the</strong> pH <strong>of</strong> <strong>the</strong> CSF would have normalized. This<br />
would result in normal cerebral blood flow, despite continued<br />
hyperventilation.<br />
Which <strong>of</strong> <strong>the</strong> following conditions would probably be present<br />
after 24 hours <strong>of</strong> continued hyperventilation <strong>of</strong> an o<strong>the</strong>rwise<br />
normal subject?<br />
A. PaCO2 < normal; CSF PCO2 < normal; CSF pH > normal;<br />
CBF < normal<br />
B. PaCO2 < normal; CSF PCO2 < normal; CSF pH > normal;<br />
CBF = normal<br />
C. PaCO2 < normal; CSF PCO2 < normal; CSF pH > normal;<br />
CBF = normal<br />
D. PaCO2 < normal; CSF PCO2 < normal; CSF pH = normal;<br />
CBF = normal<br />
adult patients undergoing orthopedic related surgeries such as congenital bone de<strong>for</strong>mities and traumatic injuries. Most <strong>of</strong> <strong>the</strong> Guatemalan<br />
population’s livelihood depends upon <strong>the</strong>ir ability to per<strong>for</strong>m manual labor. A broken bone which fails to heal properly may prevent <strong>the</strong>m<br />
from having adequate food and shelter <strong>for</strong> <strong>the</strong>mselves and <strong>the</strong>ir family. <strong>The</strong> Medical Mission Trip to Guatemala was not only an opportunity<br />
to give back but also a life-changing experience <strong>for</strong> <strong>the</strong> student nurse anes<strong>the</strong>tists.<br />
<strong>The</strong> Devil’s Causeway in Steamboat Springs, Colorado
<strong>The</strong> Department <strong>of</strong> Anes<strong>the</strong>siology<br />
<strong>The</strong> <strong>University</strong> <strong>of</strong> Tennessee Medical Center at Knoxville<br />
1924 Alcoa Highway<br />
Knoxville, TN 37902<br />
ADDRESS SERVICE REQUESTED<br />
Current Research Endeavors (See Page 9)<br />
Michael Doody, MD, Christal Greene, MD, Lally Lehmann, MD<br />
�� Algorithm Development <strong>for</strong> Cooling Ca<strong>the</strong>ter Use in<br />
Head Trauma Russell Langdon, MD; Christal Greene, MD<br />
Non-Pr<strong>of</strong>it Org.<br />
U. s. Postage<br />
PAID<br />
<strong>University</strong> <strong>of</strong> Tennessee<br />
Knoxville<br />
Fall 2011 Volume 1 Issue 4