Fidelity Security Life Insurance Company - Marketing Financial
Fidelity Security Life Insurance Company - Marketing Financial
Fidelity Security Life Insurance Company - Marketing Financial

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
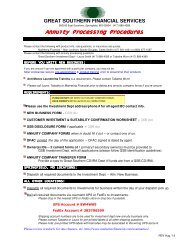
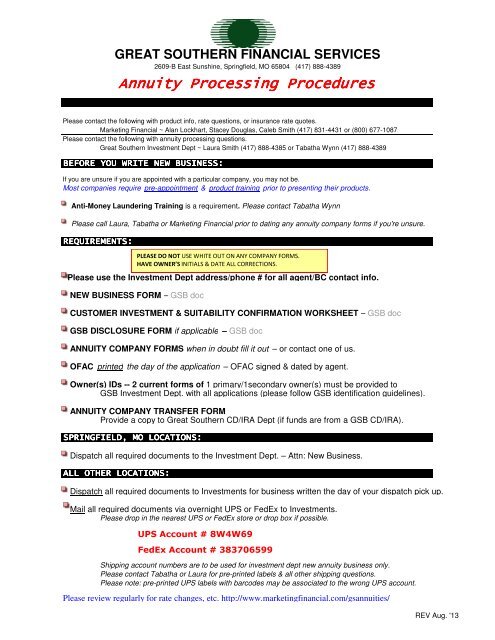
GREAT SOUTHERN FINANCIAL SERVICES<br />
2609-B East Sunshine, Springfield, MO 65804 (417) 888-4389<br />
Annuity Processing Procedures<br />
Please contact the following with product info, rate questions, or insurance rate quotes.<br />
<strong>Marketing</strong> <strong>Financial</strong> ~ Alan Lockhart, Stacey Douglas, Caleb Smith (417) 831-4431 or (800) 677-1087<br />
Please contact the following with annuity processing questions.<br />
Great Southern Investment Dept ~ Laura Smith (417) 888-4385 or Tabatha Wynn (417) 888-4389<br />
BEFORE YOU WRITE NEW BUSINESS:<br />
If you are unsure if you are appointed with a particular company, you may not be.<br />
Most companies require pre-appointment & product training prior to presenting their products.<br />
Anti-Money Laundering Training is a requirement. Please contact Tabatha Wynn<br />
Please call Laura, Tabatha or <strong>Marketing</strong> <strong>Financial</strong> prior to dating any annuity company forms if you're unsure.<br />
REQUIREMENTS:<br />
Please use the Investment Dept address/phone # for all agent/BC contact info.<br />
NEW BUSINESS FORM – GSB doc<br />
CUSTOMER INVESTMENT & SUITABILITY CONFIRMATION WORKSHEET – GSB doc<br />
GSB DISCLOSURE FORM if applicable – GSB doc<br />
ANNUITY COMPANY FORMS when in doubt fill it out – or contact one of us.<br />
OFAC printed the day of the application – OFAC signed & dated by agent.<br />
Owner(s) IDs -- 2 current forms of 1 primary/1secondary owner(s) must be provided to<br />
GSB Investment Dept. with all applications (please follow GSB identification guidelines).<br />
ANNUITY COMPANY TRANSFER FORM<br />
Provide a copy to Great Southern CD/IRA Dept (if funds are from a GSB CD/IRA).<br />
SPRINGFIELD, MO LOCATIONS:<br />
Dispatch all required documents to the Investment Dept. – Attn: New Business.<br />
ALL OTHER LOCATIONS:<br />
PLEASE DO NOT USE WHITE OUT ON ANY COMPANY FORMS.<br />
HAVE OWNER’S INITIALS & DATE ALL CORRECTIONS.<br />
Dispatch all required documents to Investments for business written the day of your dispatch pick up.<br />
Mail all required documents via overnight UPS or FedEx to Investments.<br />
Please drop in the nearest UPS or FedEx store or drop box if possible.<br />
UPS Account # 8W4W69<br />
FedEx Account # 383706599<br />
Shipping account numbers are to be used for investment dept new annuity business only.<br />
Please contact Tabatha or Laura for pre-printed labels & all other shipping questions.<br />
Please note: pre-printed UPS labels with barcodes may be associated to the wrong UPS account.<br />
Please review regularly for rate changes, etc. http://www.marketingfinancial.com/gsannuities/<br />
REV Aug. '13
2609-B East Sunshine, Springfield, MO 65804 (417) 888-4389<br />
New Business Form<br />
Client Name(s): _________________________________<br />
Owner's age(s): _______________<br />
BC #/State: ____/______<br />
Writing Agent Name: _____________________________<br />
Split Commission with: (if applicable): ________________<br />
Referred by: _______________________________________<br />
Commission Split %: ________________________________<br />
Funds Info:<br />
Internal Funds (GSB)<br />
External Funds<br />
Check Enclosed: $_______________________________<br />
Qualified (CD/IRA, 401K, etc)<br />
Non-Qualified (Checking, CD, etc)<br />
Transfer(s) Approx: $_____________________________<br />
Qualified (CD/IRA, 401K, etc)<br />
Non-Qualified (Checking, Annuity, CD, etc)<br />
<strong>Company</strong> Name _________________________<br />
ex: Sagicor<br />
Product Name __________________________<br />
ex: Sage Choice SPDA<br />
Surrender Charge Period (years) ____________<br />
1035 Exchange (NQ life/annuity) Approx: $_______________________<br />
Agent Check List:<br />
New Business<br />
Non-Qualified - <strong>Life</strong>/Annuity to <strong>Life</strong>/Annuity<br />
Application<br />
1035 Exchange Form<br />
Disclosures<br />
State Replacement Form<br />
Owner's ID<br />
Original Policy or Lost Policy Affidavit<br />
Owner's OFAC<br />
Cashier's/Personal Check Payable to <strong>Company</strong> IRA Annuity to IRA Annuity<br />
IRA Trsf Form<br />
IRA Trsf/Rollover<br />
Replacement Form<br />
IRA Trsf Form<br />
Original Policy or Lost Policy Affidavit<br />
<strong>Company</strong> Specific Forms (401K) W-9 (funds coming from Lincoln Benefit <strong>Life</strong> )<br />
Agent's Report - Source of Funds: (MUST BE COMPLETED)<br />
1. Provide your detailed explanation regarding how this purchase meets the client's stated investment goal.<br />
Attach additional sheet if necessary.<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________<br />
Agent Signature: ________________________________________<br />
Approver Signature (Laura M. Smith): _____________________________<br />
Date: _____________________<br />
Date: _____________________<br />
REV 05-2013
2609-B East Sunshine, Springfield, MO 65804 (417) 888-4389<br />
Date:<br />
Owner Name:<br />
Joint Owner Name:<br />
<strong>Company</strong>/Product:<br />
Owner(s) Initials<br />
Disclosures<br />
Not FDIC Insured.<br />
Not a deposit or other obligation of Great Southern Bank.<br />
It is understood that if the contract is prematurely ended by the client,<br />
surrender charges will apply for the first ______ years.<br />
Any money taken out of this contract in excess of the penalty free<br />
withdrawal amount provided in the contract during the surrender<br />
charge period will incur a penalty.<br />
The minimum guaranteed interest rate for the contract is ______%.<br />
The first year rate is ______ % which includes a bonus of ______%.<br />
(Does not apply to indexed annuities)<br />
If there are any surrender charges or penalties of any kind associated<br />
with the money used to purchase this annuity please list the amount of<br />
penalty: $______.<br />
This contract was purchased with Qualified or Non-Qualified funds.<br />
(Please circle which applies)<br />
Signatures<br />
Owner:<br />
Joint Owner:<br />
Representative:<br />
REV 05-2013
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway, Kansas City, Missouri 64111-2406<br />
TaxVantage TM Annuity Application<br />
Underwritten by <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong>, Kansas City, Missouri<br />
Plan Type:<br />
❏ Traditional IRA<br />
❏ Roth IRA<br />
Premium Type: ❏ Flexible Premium ❏ Single Premium<br />
Print Full Name__________________________________________________________________ SSN________________________<br />
Last First Middle<br />
Mailing Address_______________________________________________________________________________________________<br />
Street City State Zip<br />
Residential Address____________________________________________________________________________________________<br />
Street City State Zip<br />
E-Mail Address________________________________________________________________________________________________<br />
Home Phone _______________________________________<br />
Work Phone ____________________________________________<br />
Date of Birth ______/______/______ (Mo/Day/Yr) ❏ Male ❏ Female<br />
❏ Primary<br />
❏ Contingent<br />
❏ Primary<br />
❏ Contingent<br />
❏ Primary<br />
❏ Contingent<br />
❏ Primary<br />
❏ Contingent<br />
Beneficiary Allocation Relationship SS#<br />
___________________________________ ________ % ________________________ ______________________<br />
___________________________________ ________ % ________________________ ______________________<br />
___________________________________ ________ % ________________________ ______________________<br />
___________________________________ ________ % ________________________ ______________________<br />
Primary Beneficiary Allocation total must equal 100%. Contingent Beneficiary Allocation total must equal 100%.<br />
Do you have any existing annuity or life insurance contracts?<br />
❏ Yes ❏ No<br />
Is any annuity or life insurance contract being replaced with this purchase?<br />
❏ Yes ❏ No<br />
If Yes to either question, please provide the name of the insurance company(ies) and contract or policy number for each product<br />
being replaced. Please complete the replacement form.<br />
Owner Signature X______________________________________________________ Date ______/______/______ (Mo/Day/Yr)<br />
To your knowledge and belief does the applicant have any existing annuity or life insurance contracts?<br />
To your knowledge and belief is any annuity or insurance contract being replaced with this purchase?<br />
If yes, Replacement Notice must be completed.<br />
❏ Yes ❏ No<br />
❏ Yes ❏ No<br />
I have verified the applicant’s identity by viewing: ❏ Drivers License Drivers License # _______________________________<br />
❏ Other________________________________________________________<br />
Agent Signature X_______________________________________________________ Date ______/______/______ (Mo/Day/Yr)<br />
A-01142NE For Office Use Only 95-32524 #5533 0313
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway, Kansas City, Missouri 64111-2406<br />
TaxVantage TM Annuity Application<br />
Underwritten by <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong>, Kansas City, Missouri<br />
Plan Type:<br />
❏ Non-Qualified<br />
❏ Other _________________________<br />
Premium Type: ❏ Flexible Premium ❏ Single Premium<br />
OWNER INFORMATION (Natural Person):<br />
Print Full Name__________________________________________________________________ SSN________________________<br />
Last First Middle<br />
Mailing Address_______________________________________________________________________________________________<br />
Street City State Zip<br />
Residential Address____________________________________________________________________________________________<br />
Street City State Zip<br />
E-Mail Address________________________________________________________________________________________________<br />
Home Phone _______________________________________<br />
Work Phone ____________________________________________<br />
Date of Birth ______/______/______ (Mo/Day/Yr) ❏ Male ❏ Female<br />
❏ Primary<br />
❏ Contingent<br />
❏ Primary<br />
❏ Contingent<br />
❏ Primary<br />
❏ Contingent<br />
❏ Primary<br />
❏ Contingent<br />
Beneficiary Allocation Relationship SS#<br />
___________________________________ ________ % ________________________ ______________________<br />
___________________________________ ________ % ________________________ ______________________<br />
___________________________________ ________ % ________________________ ______________________<br />
___________________________________ ________ % ________________________ ______________________<br />
Primary Beneficiary Allocation total must equal 100%. Contingent Beneficiary Allocation total must equal 100%.<br />
OWNER INFORMATION: (Non-natural Person for Non-qualified plans only):<br />
Trust* Name_________________________________________________________________________________________________<br />
Mailing Address_______________________________________________________________________________________________<br />
Street City State Zip<br />
Tax ID Number _____________________________________ Date of Trust ___________________________________________<br />
Name of Trustee(s)____________________________________________________________________________________________<br />
Mailing Address_______________________________________________________________________________________________<br />
Street City State Zip<br />
Phone Number _____________________________ Email Address ___________________________________________________<br />
IMPORTANT: A copy of the Trust title page and signature page must be submitted with the application.<br />
A-01142NE For Office Use Only 95-32524 #5533 0313
JOINT OWNER INFORMATION:<br />
Print Full Name__________________________________________________________________ SSN________________________<br />
Last First Middle<br />
Mailing Address_______________________________________________________________________________________________<br />
Street City State Zip<br />
E-Mail Address________________________________________________________________________________________________<br />
Home Phone _______________________________________<br />
Work Phone ____________________________________________<br />
Date of Birth ______/______/______ (Mo/Day/Yr) ❏ Male ❏ Female<br />
ANNUITANT INFORMATION (if different from the Owner):<br />
Print Full Name__________________________________________________________________ SSN________________________<br />
Last First Middle<br />
Mailing Address_______________________________________________________________________________________________<br />
Street City State Zip<br />
E-Mail Address________________________________________________________________________________________________<br />
Home Phone _______________________________________<br />
Work Phone ____________________________________________<br />
Date of Birth ______/______/______ (Mo/Day/Yr) ❏ Male ❏ Female<br />
Do you have any existing annuity or life insurance contracts?<br />
❏ Yes ❏ No<br />
Is any annuity or life insurance contract being replaced with this purchase?<br />
❏ Yes ❏ No<br />
If Yes to either question, please provide the name of the insurance company(ies) and contract or policy number for each product<br />
being replaced. Please complete the replacement form.<br />
Owner Signature X______________________________________________________ Date ______/______/______ (Mo/Day/Yr)<br />
Joint Owner Signature X__________________________________________________ Date ______/______/______ (Mo/Day/Yr)<br />
To your knowledge and belief does the applicant have any existing annuity or life insurance contracts?<br />
To your knowledge and belief is any annuity or insurance contract being replaced with this purchase?<br />
If yes, Replacement Notice must be completed.<br />
❏ Yes ❏ No<br />
❏ Yes ❏ No<br />
I have verified the applicant’s identity by viewing: ❏ Drivers License Drivers License # _______________________________<br />
❏ Other________________________________________________________<br />
Agent Signature X_______________________________________________________ Date ______/______/______ (Mo/Day/Yr)<br />
A-01142NE For Office Use Only 95-32524 #5533 0313
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway<br />
Kansas City, MO 64111<br />
Direct Rollover/Transfer Form<br />
Please read and complete sections 1 - 6 of this form, then sign and date where indicated. You may give the form to your agent or mail it directly to<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> at the address shown at the top of this form. Make sure you first complete all forms required by the employer maintaining your plan.<br />
Part 1: Name and Address Information (Please Print)<br />
Name ____________________________________________________ Social <strong>Security</strong> Number ________________________________<br />
Address __________________________________________________ Your Home Phone ____________________________________<br />
City _____________________________ State ______ ZIP__________ Your Work Phone ____________________________________<br />
Part 2: Your Existing Account/Plan (Current <strong>Company</strong>/Custodian)<br />
Name of <strong>Company</strong> __________________________________________<br />
Address __________________________________________________<br />
________________________________________________________<br />
City _____________________________ State ______ ZIP__________<br />
Account/Plan Number __________________________________<br />
Plan Name __________________________________________<br />
Plan Administrator Name ________________________________<br />
Contact Number ______________________________________<br />
Part 3: FROM Account Type (check one): ❑ IRA ❑ 403(b) ❑ 401(k) ❑ 401(a) ❑ 457<br />
❑ Roth IRA ❑ Roth 403(b) ❑ Roth 401(k) ❑ Other____________________<br />
Part 4: TO Account Type (check one): ❑ IRA ❑ 403(b) ❑ 401(k) ❑ 401(a) ❑ 457<br />
❑ Roth IRA ❑ Roth 403(b) ❑ Roth 401(k) ❑ Other____________________<br />
Part 5: Select Type: ❑ Plan to Plan Transfer ❑ Direct Rollover ❑ Vendor to Vendor<br />
Qualification for Direct Rollover (check one):<br />
❑ Age 59 1 ⁄2 (70 1 ⁄2 for 457) ❑ Retirement ❑ Separation from Service<br />
Part 6: TO: (Resigning <strong>Company</strong>/Custodian) How Much to Rollover/Transfer:<br />
❑<br />
❑<br />
The entire balance of my account; or<br />
A partial surrender of $ ____________________ or ___________ % from my Account/Plan.<br />
Owner Signature X ________________________________________________________________ Date ____/____/_______<br />
Employer/Third Party Administrator X ____________________________________________________ Date ____/____/_______<br />
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
Part 7: Instructions to Current Carrier:<br />
Please make proceeds payable to:<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> FBO ________________________________________________________ and forward to:<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> • Attn: Annuity Department • P.O. Box 418131 • Kansas City, MO 64141-8131<br />
ACCEPTANCE BY FIDELITY SECURITY LIFE INSURANCE COMPANY (FSL)<br />
This is to certify that <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> (FSL) has an approved contract and that we hereby accept the Transfer or Direct<br />
Rollover of assets requested above. Please send the funds to the address listed directly above.<br />
Authorized (FSL) Signature X ____________________________________<br />
Title __________________________ Date ____/____/_______<br />
Agent/Advisor Signature<br />
X ____________________________________________________________________ Date ____/____/_______<br />
95-32284 #4347 1109
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway<br />
Kansas City, MO 64111<br />
1035 Exchange Form<br />
(Non-Qualified Annuity to Annuity)<br />
Please read and complete sections 1 - 5 of this form, then sign and date where indicated. You may give the form to your agent or mail it directly to<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> at the address shown at the top of this form. Make sure you first complete all forms required by the employer maintaining<br />
your plan.<br />
Part 1: Name and Address Information (Please Print)<br />
Name ____________________________________________________ Social <strong>Security</strong> Number ________________________________<br />
Address __________________________________________________ Your Home Phone ____________________________________<br />
City _____________________________ State ______ ZIP__________<br />
Part 2: Your Existing Account/Plan (Current <strong>Company</strong>/Custodian)<br />
Name of <strong>Company</strong> __________________________________________<br />
Address __________________________________________________<br />
________________________________________________________<br />
City _____________________________ State ______ ZIP__________<br />
Part 3: To (Resigning <strong>Company</strong>/Custodian):<br />
Please Liquidate:<br />
q<br />
q<br />
The entire balance of my account; or<br />
A partial surrender of $ ____________________ or ___________ % from my Account/Plan.<br />
Part 4: *If age 85 has been attained:<br />
q<br />
q<br />
Please process my Required Minimum Distribution prior to exchange.<br />
I will satisfy my Required Minimum Distribution from another non-qualified source.<br />
Your Work Phone ______________________________________<br />
Account/Plan Number __________________________________<br />
Plan Name __________________________________________<br />
Plan Administrator Name ________________________________<br />
Contact Number ______________________________________<br />
I hereby irrevocably assign the contract or certificate represented in exchange for a new non-qualified annuity contract or certificate issued by<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong>, as part of a single integrated exchange of annuity contracts intended to satisfy the requirements under section 1035(a) of<br />
the Internal Revenue Code.<br />
Owner Signature X ________________________________________________________________ Date ____/____/_______<br />
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .<br />
Part 5: Instructions to Current Carrier:<br />
Please provide cost basis information and make proceeds payable to:<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> FBO ________________________________________________________ and forward to:<br />
(name of account holder)<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
Attn: Annuity Administration Department<br />
P.O. Box 418131<br />
Kansas City, MO 64141-8131<br />
ACCEPTANCE BY FIDELITY SECURITY LIFE INSURANCE COMPANY<br />
This is to certify that <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> has an approved contract and hereby accept the assets requested above.<br />
Authorized Signature X ____________________________________________ Title ________________________________________<br />
Date ____/____/_______<br />
95-32283 #5529 611
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway, Kansas City, Missouri 64111-2406<br />
TaxVantage TM Annuitization Request Form<br />
1 Please provide personal information: Please print in ink or type all answers.<br />
Name:<br />
________________________________________________________________________________________________________________<br />
First Middle Last<br />
Address:________________________________________________________________________________________________________________<br />
Street City State ZIP<br />
ID No. ______________________________________________________ Contract(s)________________________________________________<br />
Social <strong>Security</strong> No. ___________________________ Date of Birth ____/____/_______ Telephone No. ( ______ ) ________________________<br />
❑ Check here if this is a new address. If address is different from above, please indicate where you would like your payments mailed.<br />
Address:________________________________________________________________________________________________________________<br />
Street City State ZIP<br />
For direct bank deposits, please enclose a voided check from the account to which you would like payment deposited.<br />
Please be sure to complete the beneficiary designation information on the back of this form.<br />
In accordance with the terms of the Annuity Contract and with respect to the Annuity Option, I hereby request — in lieu of all benefits otherwise<br />
payable to me — the option checked below. If any prior request or election has been made as to optional retirement benefits, I hereby revoke and<br />
cancel any such prior request or election.<br />
2 Please check only one option:<br />
❑ <strong>Life</strong> Annuity — Annuity payable to the Annuitant for as long as he/she lives.<br />
❑ Certain Annuity — Annuity payable for 5 through 20 years certain. Upon death of the Annuitant prior to the end of the certain period, any<br />
payments for the balance of such period will be paid to his/her beneficiary. Number of years desired __________.<br />
❑ Certain and <strong>Life</strong> Annuity — annuity payable for 5, 10, 15, or 20 years certain as long thereafter as the Annuitant is living. Upon the death of the<br />
Annuitant prior to the end of the certain period, any payments for the balance of such period will be paid to his/her beneficiary. Number of years<br />
desired __________.<br />
❑ Survivorship Annuity — Annuity payable to the Annuitant for as long as he/she lives. Upon his/her death, payment will continue at 100%, 75%,<br />
or 50% to the contingent (second) Annuitant for the life of the contingent (second) Annuitant. Please complete the section on the back for<br />
contingent Annuitant information. Percentage desired __________.<br />
If you chose any annuity except the Certain Annuity, please enclose a certified or notarized copy of your birth certificate. If you chose the Survivorship Annuity,<br />
please enclose certified or notarized copies of both your birth certificate and that of the contingent Annuitant.<br />
3 Please complete this section:<br />
❑ Full ❑ Partial Annuitization. If Partial, indicate amount $___________ OR ______% Date to begin receiving first payment ____/____/_______<br />
If Full Annuitization, your last contribution will be for the payroll period ending ____/____/_______<br />
❑ Do<br />
❑ Do Not withhold federal income tax from any annuity payment I receive.<br />
Annuity Income to be Paid ❑ Monthly ❑ Quarterly ❑ Semiannually ❑ Annually
4 For the Survivorship Annuity, complete this section:<br />
Please provide information on the contingent (second) Annuitant, and enclose a certified or notarized copy of his/her birth certificate.<br />
Name:<br />
________________________________________________________________________________________________________________<br />
First Middle Last<br />
Address:________________________________________________________________________________________________________________<br />
Street City State ZIP<br />
Social <strong>Security</strong> No. ___________________________ Date of Birth ____/____/_______ Relationship<br />
Telephone No. ( _______ ) ___________________________________________<br />
__________________________________<br />
5 For all other annuity options (except <strong>Life</strong> or Survivorship), complete this section:<br />
Beneficiary Designation: Print full names and entire addresses.<br />
I hereby request the beneficiary under the numbered contract shown on the front to take effect in accordance with the contract provisions as follows:<br />
Primary Beneficiary: This beneficiary designation supersedes any and all other beneficiary designations.<br />
Name: ________________________________________________________________________________________________________________<br />
First Middle Last<br />
Address:________________________________________________________________________________________________________________<br />
Street City State ZIP<br />
Social <strong>Security</strong> No. ___________________________ Date of Birth ____/____/_______ Relationship __________________________________<br />
Contingent Beneficiary: This beneficiary designation supersedes any and all other beneficiary designations.<br />
Name: ________________________________________________________________________________________________________________<br />
First Middle Last<br />
Address:________________________________________________________________________________________________________________<br />
Street City State ZIP<br />
Social <strong>Security</strong> No. ___________________________ Date of Birth ____/____/_______ Relationship __________________________________<br />
It is understood and agreed that proceeds will be paid in equal shares, unless otherwise designated, to any surviving beneficiaries; but if none survives,<br />
proceeds will be paid in equal shares to any surviving contingent (second) beneficiaries.<br />
6 Please sign here:<br />
I agree that the benefits as elected above are accepted in full settlement and complete satisfaction of any and all rights and benefits with respect to<br />
me under said Annuity Contract.<br />
Owner Signature X ________________________________________________________________________________<br />
Date ____/____/_______<br />
Witness<br />
________________________________________________________________________________________<br />
Annuitant Spouse’s Signature if Community Property state ________________________________________________<br />
For <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> Home Office Use Only:<br />
Completed by ____________________________________________________________________________________<br />
Date ____/____/_______<br />
Attention Annuitant: Notify <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> if this copy does not contain your desired requests or if it is incorrect in any way.<br />
As indicated by signature in this section, <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> has recorded your requested changes.<br />
93-32131 #6136 1112
Exhibit I – Annuity Suitability Questionnaire<br />
Yes, I agree to answer the questions below and I understand that my responses will be used to evaluate the suitability of an<br />
annuity contract. I understand that FSL may elect not to issue the annuity contract being applied for based on a<br />
reasonable determination that the product may not be suitable for me.<br />
Proposed Annuitant Primary <strong>Financial</strong> Objectives (Check all that apply)<br />
Name: Preservation of Capital Future Income<br />
Address: Wealth Accumulation Charitable Giving<br />
Tax Deferral<br />
Education Planning<br />
Home Phone No.:<br />
Social <strong>Security</strong> No.:<br />
Age at Last Birthday:<br />
Immediate Income<br />
Inheritance<br />
Time Frame for this Investment<br />
When will you need the money you are investing in this<br />
Marital Status: Married Single annuity? (Circle One)<br />
Widowed<br />
Divorced<br />
1 year or less 7 – 10 years<br />
Occupation: 1 – 3 years 10 years or more<br />
3 – 7 years Never (money is for<br />
charity/inheritance)<br />
<strong>Financial</strong> Information<br />
Annual Household Income $<br />
Existing Accounts<br />
Are you considering using funds from existing life<br />
insurance policies, annuity contracts, or certificates of<br />
Liquid Net Worth $ deposit to purchase this annuity?<br />
(Excluding residence and furnishings) Yes No<br />
Source of Income: (Check all that apply)<br />
How long has that policy(ies), contract(s), or certificate<br />
Employment Retirement Plans of deposit(s) been in force?<br />
Investments Other # of Years<br />
Social <strong>Security</strong><br />
Are there any surrender charges associated with the<br />
Tax Bracket: (Check one)<br />
above-mentioned existing policy(ies), contract(s), or<br />
10% 15% 25% 28% 33% 35% certificates of deposit?<br />
Yes No Not Applicable<br />
Proposed Annuity represents % of Net my Worth<br />
Do you have any funds available to you in case of<br />
emergency?<br />
If yes, what is/are the current surrender charge(s)?<br />
Other relevant information (financial constraints, health<br />
concerns, long-term care considerations, etc.)<br />
OWNER ACKNOWLEDGEMENT<br />
By signing below, I acknowledge that I reviewed with my agent the product-specific disclosure form and that I<br />
understand the costs and features of the annuity I am purchasing. In addition, I acknowledge the information I<br />
provided is complete and accurate to the best of my knowledge. I further acknowledge that neither <strong>Fidelity</strong> <strong>Security</strong><br />
<strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> nor its representatives offer legal or tax advice. I have been advised to consult my<br />
personal tax advisor or lawyer with any questions or concerns. I believe the annuity I am applying for is suitable<br />
based on my insurance needs and financial objectives.<br />
Owner Signature<br />
Date<br />
AGENT ACKNOWLEDGEMENT<br />
By signing below, I acknowledge that based on the information the Owner provided and based on all the<br />
circumstances known to me at the time the recommendation was made, the annuity being applied for is suitable<br />
based on insurance needs and financial objectives of the Owner. In addition, I have verified the identity of the<br />
Owner and believe that the identity information the Owner provided to me is true and accurate.<br />
Agent Signature<br />
Date<br />
N-00261 93-33293<br />
Shaded information indicates new material 08/01/12<br />
Page 7 SPM 100
Exhibit II A – Waiver of Annuity Suitability<br />
IMPORTANT!<br />
Your Coverage cannot be issued without your signature on either the Waiver below,<br />
or the attached Suitability Questionnaire.<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway, Kansas City, MO 64111<br />
Waiver of Annuity Suitability<br />
We appreciate your interest in an annuity contract from <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> ("FSL"). We are required<br />
by various states to ask for information that will help determine whether an annuity contract is suitable for your investment<br />
goals and financial situation. The questions pertain to your personal situation at the time of this application, and to your<br />
understanding of the features of the product for which you are applying. This information will not be used for any other<br />
purpose and will remain confidential.<br />
You have the legal right to decline to provide this information. If this is your wish, please read the following<br />
statement, sign, date, and return this form with your Application for Annuity.<br />
WAIVER of Annuity Suitability Questionnaire<br />
No, I will not answer the questions on the attached sheet, and I take full responsibility for determining whether the<br />
proposed annuity is suitable for me.<br />
(The Proposed Annuitant must sign in the "Signature" space below. Your policy cannot be issued without your signature on<br />
either this WAIVER or the attached Annuity Suitability Questionnaire.)<br />
Proposed Annuitant Signature<br />
Date<br />
N-00262 93-33294<br />
Shaded information indicates new material 08/01/12<br />
Page 9 SPM 100
Exhibit II B – Declination to Follow Recommendation<br />
IMPORTANT!<br />
Your Coverage cannot be issued without your signature on both the Declination below<br />
and the attached Suitability Questionnaire.<br />
<strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong><br />
3130 Broadway, Kansas City, MO 64111<br />
Declination to Follow Recommendation<br />
We appreciate your interest in an annuity contract from <strong>Fidelity</strong> <strong>Security</strong> <strong>Life</strong> <strong>Insurance</strong> <strong>Company</strong> ("FSL"). We are required<br />
by various states to ask for information that will help determine whether an annuity contract is suitable for your investment<br />
goals and financial situation. The questions pertain to your personal situation at the time of this application, and to your<br />
understanding of the features of the product for which you are applying. This information will not be used for any other<br />
purpose and will remain confidential.<br />
You also have the legal right to not follow any recommendation made. If this is your wish, please read the<br />
following statement, sign, date and return this form with your Application for Annuity.<br />
DECLINING to Follow Recommendation<br />
Based upon the information on the attached sheet, the annuity transaction was not recommended. I take full<br />
responsibility for determining whether the proposed annuity is suitable for me.<br />
(The Proposed Annuitant must sign in the "Signature" space below. Your policy cannot be issued without your signature on<br />
both this DECLINATION and the attached Annuity Suitability Questionnaire.)<br />
Proposed Annuitant Signature<br />
Date<br />
N-00260 93-33292<br />
Shaded information indicates new material 08/01/12<br />
Page 10 SPM 100