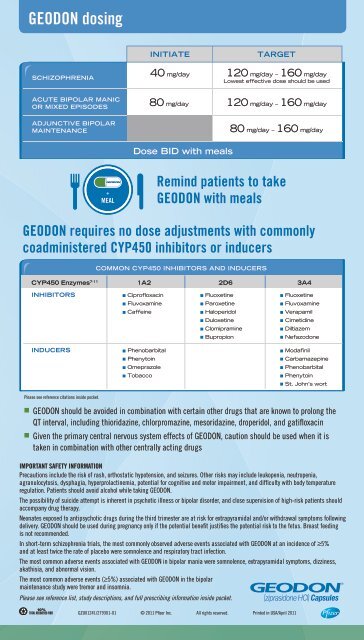
<strong>GEODON</strong> <strong>dosing</strong>INITIATETARGETSCHIZOPHRENIA40 mg/day 120 mg/day – 160 mg/dayLowest effective dose should be usedACUTE BIPOLAR MANICOR MIXED EPISODES80 mg/day120 mg/day – 160 mg/dayADJUNCTIVE BIPOLARMAINTENANCE80 mg/day – 160 mg/dayDose BID with mealsRemind patients to take<strong>GEODON</strong> with meals<strong>GEODON</strong> requires no dose adjustments with commonlycoadministered CYP450 inhibitors or inducersCOMMON CYP450 INHIBITORS AND INDUCERSCYP450 Enzymes 7-111A22D63A4INHIBITORSCiprofloxacinFluoxetineFluoxetineFluvoxamineParoxetineFluvoxamineCaffeineHaloperidolVerapamilDuloxetineCimetidineClomipramineDiltiazemBupropionNefazodoneINDUCERS PhenobarbitalModafinilPlease see <strong>reference</strong> citations inside pocket.PhenytoinOmeprazoleTobaccoCarbamazepinePhenobarbitalPhenytoinSt. John’s wortn <strong>GEODON</strong> should be avoided in combination with certain other drugs that are known to prolong theQT interval, including thioridazine, chlorpromazine, mesoridazine, droperidol, and gatifloxacinn Given the primary central nervous system effects of <strong>GEODON</strong>, caution should be used when it istaken in combination with other centrally acting drugsImportant Safety InformationPrecautions include the risk of rash, orthostatic hypotension, and seizures. Other risks may include leukopenia, neutropenia,agranulocytosis, dysphagia, hyperprolactinemia, potential for cognitive and motor impairment, and difficulty with body temperatureregulation. Patients should avoid alcohol while taking <strong>GEODON</strong>.The possibility of suicide attempt is inherent in psychotic illness or bipolar disorder, and close supervision of high-risk patients shouldaccompany drug therapy.Neonates exposed to antipsychotic drugs during the third trimester are at risk for extrapyramidal and/or withdrawal symptoms followingdelivery. <strong>GEODON</strong> should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Breast feedingis not recommended.In short-term schizophrenia trials, the most commonly observed adverse events associated with <strong>GEODON</strong> at an incidence of ≥5%and at least twice the rate of placebo were somnolence and respiratory tract infection.The most common adverse events associated with <strong>GEODON</strong> in bipolar mania were somnolence, extrapyramidal symptoms, dizziness,akathisia, and abnormal vision.The most common adverse events (≥5%) associated with <strong>GEODON</strong> in the bipolarmaintenance study were tremor and insomnia.Please see <strong>reference</strong> list, study descriptions, and full prescribing information inside pocket.GZU01241/279301-01 © 2011 Pfizer Inc. All rights reserved. Printed in USA/April 2011
STUDY DESCRIPTIONSKeck 2004<strong>GEODON</strong> vs placebo (2 pooled, 3-week bipolar mania studies)(retrospective data are a mixed-model, repeated-measures analysis)Results from 2 pooled, multicenter, double-blind, randomized, fl exible-dose, 21-day studies of<strong>GEODON</strong> vs placebo in 415 inpatients with a primary diagnosis of Bipolar I Disorder with amanic or mixed episode. Patients had Mania Rating Scale (MRS) scores ≥14 at baseline. In thefi rst study, the starting dose was 80 mg on Day 1, increased to 160 mg on Day 2 and adjustedthereafter by a maximum of 40 mg/day to between 80 mg/day and 160 mg/day. In the secondstudy, the starting dose was 80 mg on Day 1 and could be adjusted starting on Day 2 by amaximum of 40 mg/day to between 80 mg/day and 160 mg/day. Effi cacy measures includedMRS, Manic Syndrome Subscale, Behavior and Ideation Subscale, and the 17-item HamiltonDepression Rating Scale (HAM-D), as well as Clinical Global Impression of Severity (CGI-S),Clinical Global Impression of Improvement (CGI-I), Positive and Negative Syndrome Scale(PANSS), and Global Assessment of Functioning (GAF). Data were analyzed using lastobservation carried forward (LOCF). All double-blind study medications were administeredtwice daily with food.Daniel 1999<strong>GEODON</strong> vs placebo (6-week schizophrenia study)Results from a 6-week, double-blind, placebo-controlled, parallel-group, fixed-dose, multicenterstudy of 302 inpatients with an acute exacerbation of schizophrenia or schizoaffective disorder.The primary efficacy assessments for this study were Positive and Negative Syndrome Scale(PANSS) total score, PANSS negative subscale score, the derived Brief Psychiatric Rating Scale(BRPS) total score, BPRS core items score, and Clinical Impression of Severity (CGI-S). Secondaryefficacy assessments included Clinical Global Impression of Improvement (CGI-I) and Montgomery-Asberg Depression Rating Scale (MADRS). Data were analyzed using last observation carriedforward (LOCF). After a 3- to 7-day washout period, patients were randomized to receive <strong>GEODON</strong>80 mg/day on Days 1 and 2, followed by 80 mg/day or 160 mg/day on Days 3 to 42; or placebo.All double-blind study medications were administered twice daily with food.Bowden 2010<strong>GEODON</strong> plus lithium or valproate vs lithium or valproate alone(6 month bipolar maintenance study)Results from a 6-month, placebo-controlled, double-blind, randomized trial in patients diagnosedwith bipolar I disorder, whose current or most recent episode was manic or mixed. This study had 2phases: an open-label stabilization phase of 10-16 weeks and a double-blind maintenance phaseof up to 6 months. In the open-label phase, patients were required to be stabilized on <strong>GEODON</strong> pluslithium or valproate for at least 8 weeks in order to be randomized. In the double-blind phase,stabilized patients were randomized and treated with <strong>GEODON</strong> combined with lithium or valproate(n=127) or placebo combined with lithium or valproate (n=112). One patient in the placebo armdid not have at least one post-randomization observation and was therefore excluded from the ITTanalysis. Generally, in the maintenance phase, patients continued on the same dose on which theywere initially stabilized, within the range of 80 mg/day to 160 mg/day. The primary end point wasthe time to recurrence of a mood episode requiring intervention during the double-blind phase.Mood episodes were classified as manic, mixed, or depressive. Recurrence of a mood episoderequiring intervention (relapse) was defined as one or more of the following: investigator decideddiscontinuation was in the best interest of the patient; a loss of effect and/or requirement for analteration to the treatment regimen (investigator judgment); patient was hospitalized for diseaseunder study; MRS rating was ≥18 for 2 consecutive visits scheduled no more than 10 days apart;MADRS rating was ≥18 for 2 consecutive visits scheduled no more than 10 days apart. The keysecondary end point was the time to discontinuation for any reason during the double-blind phase.Please see full prescribing information inside pocket.