Confidential Morbidity Report - California Department of Public Health
Confidential Morbidity Report - California Department of Public Health
Confidential Morbidity Report - California Department of Public Health

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
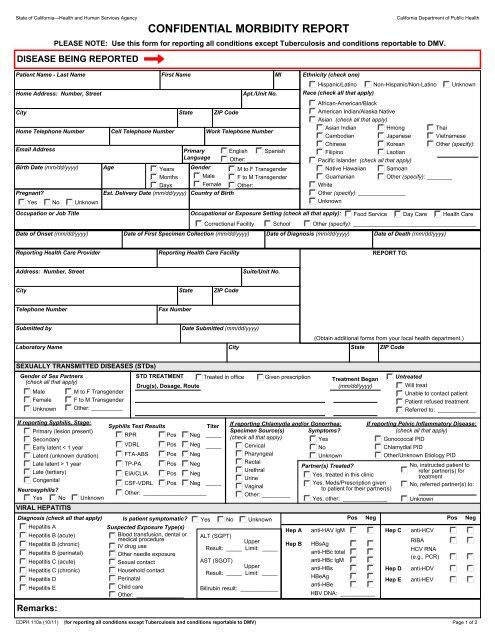
State <strong>of</strong> <strong>California</strong>—<strong>Health</strong> and Human Services AgencyDISEASE BEING REPORTEDPatient Name - Last NameCONFIDENTIAL MORBIDITY REPORT<strong>California</strong> <strong>Department</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>PLEASE NOTE: Use this form for reporting all conditions except Tuberculosis and conditions reportable to DMV.Home Address: Number, StreetCityHome Telephone NumberCell Telephone NumberFirst NameEmail Address Primary English SpanishLanguage Other: ______________Birth Date (mm/dd/yyyy) Age Years Gender M to F TransgenderMonths Male F to M TransgenderDaysFemale Other: ____________Pregnant?Est. Delivery Date (mm/dd/yyyy) Country <strong>of</strong> BirthYes No UnknownStateZIP CodeApt./Unit No.Work Telephone NumberMIEthnicity (check one)Hispanic/Latino Non-Hispanic/Non-Latino UnknownRace (check all that apply)African-American/BlackAmerican Indian/Alaska NativeAsian (check all that apply)Asian Indian Hmong ThaiCambodianJapanese VietnameseChineseKoreanOther (specify):FilipinoLaotianPacific Islander (check all that apply)Native Hawaiian SamoanGuamanianOther (specify): ________WhiteOther (specify): _______________UnknownOccupation or Job Title Occupational or Exposure Setting (check all that apply): Food Service Day Care <strong>Health</strong> CareCorrectional Facility School Other (specify): _______________________________________Date <strong>of</strong> Onset (mm/dd/yyyy) Date <strong>of</strong> First Specimen Collection (mm/dd/yyyy) Date <strong>of</strong> Diagnosis (mm/dd/yyyy) Date <strong>of</strong> Death (mm/dd/yyyy)<strong>Report</strong>ing <strong>Health</strong> Care Provider<strong>Report</strong>ing <strong>Health</strong> Care FacilityREPORT TO:Address: Number, StreetSuite/Unit No.CityStateZIP CodeTelephone NumberFax NumberSubmitted byDate Submitted (mm/dd/yyyy)(Obtain additional forms from your local health department.)Laboratory Name City State ZIP CodeSEXUALLY TRANSMITTED DISEASES (STDs)Gender <strong>of</strong> Sex Partners(check all that apply)MaleFemaleUnknownM to F TransgenderF to M TransgenderOther: __________STD TREATMENTDrug(s), Dosage, RouteTreated in <strong>of</strong>ficeGiven prescriptionTreatment Began(mm/dd/yyyy)UntreatedWill treatUnable to contact patientPatient refused treatmentReferred to: ____________If reporting Syphilis, Stage:Primary (lesion present)SecondaryEarly latent < 1 yearLatent (unknown duration)Late latent > 1 yearLate (tertiary)CongenitalSyphilis Test ResultsRPRPos NegTiter_____VDRL Pos Neg _____FTA-ABS Pos NegTP-PA Pos NegEIA/CLIA Pos NegCSF-VDRL Pos Neg _____Other: ____________________Neurosyphilis?Yes No UnknownVIRAL HEPATITISDiagnosis (check all that apply)Hepatitis ASuspected Exposure Type(s)Hepatitis B (acute)Blood transfusion, dental ormedical procedureHepatitis B (chronic)IV drug useHepatitis B (perinatal)Other needle exposureHepatitis C (acute)Sexual contactHepatitis C (chronic)Household contactHepatitis DPerinatalHepatitis EChild careOther: _______________Remarks:If reporting Chlamydia and/or Gonorrhea:Specimen Source(s) Symptoms?(check all that apply)YesCervicalNoPharyngealUnknownRectalPartner(s) Treated?UrethralUrineVaginalOther: _________Is patient symptomatic? Yes No Unknown Pos NegALT (SGPT)UpperResult: _____ Limit: _____AST (SGOT)UpperResult: _____ Limit: _____Bilirubin result: ____________anti-HAV IgMHBsAganti-HBc totalanti-HBc IgManti-HBsHBeAganti-HBeHBV DNA: ___________If reporting Pelvic Inflammatory Disease:(check all that apply)Gonococcal PIDChlamydial PIDOther/Unknown Etiology PIDanti-HCVRIBAHCV RNA(e.g., PCR)CDPH 110a (10/11) (for reporting all conditions except Tuberculosis and conditions reportable to DMV) Page 1 <strong>of</strong> 2Hep AHep BYes, treated in this clinicYes, Meds/Prescription givento patient for their partner(s)Yes, other: ______________Hep CHep DHep ENo, instructed patient torefer partner(s) fortreatmentNo, referred partner(s) to:Unknownanti-HDVanti-HEVPosNeg
State <strong>of</strong> <strong>California</strong>—<strong>Health</strong> and Human Services Agency<strong>California</strong> <strong>Department</strong> <strong>of</strong> <strong>Public</strong> <strong>Health</strong>CDPH 110a (10/11)Page 2 <strong>of</strong> 2