Cutaneous T-cell lymphoma - Lymphoma Association
Cutaneous T-cell lymphoma - Lymphoma Association
Cutaneous T-cell lymphoma - Lymphoma Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Freephone helpline 0808 808 5555information@<strong>lymphoma</strong>s.org.ukwww.<strong>lymphoma</strong>s.org.uk<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>Skin <strong>lymphoma</strong>s are uncommon and only around 10 people out of every million of thepopulation will develop a skin <strong>lymphoma</strong> each year in the UK. Before being diagnosedwith this condition or before being close to someone who has it, you might nevereven have heard of it.In this article we are aiming to answer the most common questions people ask aboutthese <strong>lymphoma</strong>s:●What is skin <strong>lymphoma</strong>? (page 2)●What causes skin <strong>lymphoma</strong>? (page 3)●What are the symptoms of skin <strong>lymphoma</strong>? (page 3)●How is skin <strong>lymphoma</strong> diagnosed? (page 5)●What tests might I need to assess the <strong>lymphoma</strong>? (page 5)●What do the tests tell the medical team? (page 7)●What do the 'stages' mean? (page 8)●Are skin <strong>lymphoma</strong>s curable? (page 9)We will then concentrate on the most common form of skin <strong>lymphoma</strong>, cutaneousT-<strong>cell</strong> <strong>lymphoma</strong> or CTCL. We will give information on these types of CTCL:● mycosis fungoides (page 10)● Sézary syndrome (page 12)● primary cutaneous CD30-positive lymphoproliferative disorders (page 13):– primary cutaneous anaplastic large-<strong>cell</strong> <strong>lymphoma</strong>– <strong>lymphoma</strong>toid papulosis (LyP)● rare types of CTCL (page 14):– subcutaneous panniculitis-like T-<strong>cell</strong> <strong>lymphoma</strong>– primary cutaneous CD4-positive small/medium T-<strong>cell</strong> <strong>lymphoma</strong>– primary cutaneous gamma/delta T-<strong>cell</strong> <strong>lymphoma</strong>– primary cutaneous CD8-positive aggressive epidermitropic cytotoxic T-<strong>cell</strong><strong>lymphoma</strong>.Lastly we will have some information on:● taking part in a clinical trial (page 15)● going for hospital check-ups (page 15).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v31/18
What is skin <strong>lymphoma</strong>?<strong>Lymphoma</strong> is a cancer that starts in <strong>cell</strong>s called ‘lymphocytes’, which are a vital part ofour immune system. These <strong>cell</strong>s are normally found in parts of the body where theycan be ready to fight off infections, such as in our lymph nodes (glands). They are alsofound in other ‘lymphoid tissues’, for example in the spleen, the gut and the skin.If lymphocytes start to grow out of control or don’t die off after their normal lifespan,they can build up in the lymph nodes or in these other places and form a cancerouscollection of <strong>cell</strong>s called a ‘<strong>lymphoma</strong>’. If the <strong>lymphoma</strong> starts in the lymphocytes inthe skin it is called a ‘cutaneous <strong>lymphoma</strong>’ because ‘cutaneous’ means anythingrelating to the skin.There are over 60 different kinds of <strong>lymphoma</strong> and they have been grouped into twomain types, Hodgkin <strong>lymphoma</strong> and non-Hodgkin <strong>lymphoma</strong>. These are different inhow they first become apparent, how they behave and in how they are treated. Skin<strong>lymphoma</strong>s are non-Hodgkin <strong>lymphoma</strong>s.Only around 1 in 40 non-Hodgkin <strong>lymphoma</strong>s start in the skin and these ‘primary’ skin<strong>lymphoma</strong>s are therefore quite rare cancers. A <strong>lymphoma</strong> that starts somewhere else,such as in the lymph nodes, and then spreads to the skin is not considered to be a skin<strong>lymphoma</strong>.There are two types of lymphocyte – T lymphocytes (usually just called ‘T <strong>cell</strong>s’)and B lymphocytes (B <strong>cell</strong>s) and both kinds of lymphocyte can start to accumulateuncontrollably in the skin. Skin <strong>lymphoma</strong>s can therefore develop from either T <strong>cell</strong>s orfrom B <strong>cell</strong>s:● Over three-quarters of all skin <strong>lymphoma</strong>s develop from T <strong>cell</strong>s. These are knownas primary cutaneous T-<strong>cell</strong> <strong>lymphoma</strong> or CTCL for short. These skin <strong>lymphoma</strong>soften appear as eczema-like skin rashes and can affect widespread parts of the body.The most common type of CTCL is mycosis fungoides.●Primary cutaneous B-<strong>cell</strong> <strong>lymphoma</strong>s (CBCLs) more commonly causes lumps inthe skin that are found in one or two discrete areas of the body.We have more information available on skin <strong>lymphoma</strong>s. The treatments thatwe will describe briefly in this article are explained in much greater detail in theinformation sheet:● Treatments for skin <strong>lymphoma</strong>.The practicalities of day-to-day living with skin <strong>lymphoma</strong> are discussed in theinformation sheet:● Living with skin <strong>lymphoma</strong>.We also have information on cutaneous B-<strong>cell</strong> <strong>lymphoma</strong>. If you haven’t receivedall the articles that you think would be suitable for you and would like these, orif you would like to talk to someone about your skin <strong>lymphoma</strong>, please ring ourhelpline (0808 808 5555). Alternatively, the information can be downloaded fromour website (www.<strong>lymphoma</strong>s.org.uk).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v32/18
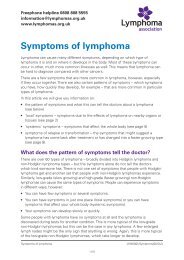
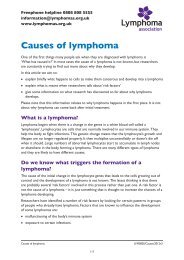
What causes skin <strong>lymphoma</strong>?The cause of skin <strong>lymphoma</strong> is not known. It cannot be inherited and it cannot becaught or passed on to other people. Nothing you have done will have caused the<strong>lymphoma</strong>.Research has shown that the lymphocytes become cancerous because of changes inthe chemical coding or DNA of the <strong>cell</strong>’s genes and in how the gene collections (thechromosomes) are arranged. These changes are not genetic in the sense of beinginherited from your parents – they happen to the lymphocyte <strong>cell</strong>s after birth. It is notreally understood why they happen, but increasing age is probably a factor, whichexplains why most skin <strong>lymphoma</strong>s happen in people in their 50s or 60s, or later.Although the cause of a skin <strong>lymphoma</strong> developing in any one person is not known,there are a few things that make them a bit more likely to develop. These are knownas ‘risk factors’. As we explained in the last paragraph, older age is one risk factor.In addition, many types of skin <strong>lymphoma</strong>s are more common in men. In the UnitedStates skin <strong>lymphoma</strong> is also more common in Afro-Caribbean people than it is in thewhite population, but it is not known why this is.Skin <strong>lymphoma</strong>s have been found to be more common if the body’s immune systemis not working properly. This can happen as a result of the drugs people have totake to prevent rejection after they have had a kidney, heart or liver transplant. Itcan also happen in people with AIDS (acquired immune deficiency syndrome) andin people with certain rare inherited diseases of the immune system such as ataxiatelangiectasia.In some parts of the world, in the Caribbean and Asia for example, it is thought that aninfection with a virus called human lymphotropic virus 1 (HTLV-1) might be involved inthe development of CTCL.What are the symptoms of skin <strong>lymphoma</strong>?Figure 1: Patches of mycosis fungoides, showingareas of dry red skinMost types of CTCL begin asflat, red patches on the skin. Thepatches might not be irritating atall (unlike patches of eczema) butthey can sometimes be itchy. Theytend to be dry and are sometimesscaly (see figures 1 and 2). At thisstage it can look very like muchmore common skin conditionssuch as dermatitis, eczema orpsoriasis.<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v33/18
If there are abnormal <strong>lymphoma</strong> <strong>cell</strong>s (sometimes called ‘Sézary <strong>cell</strong>s’) circulating inthe bloodstream your whole body can feel intensely itchy. If there are large numbersof these <strong>cell</strong>s this can decrease your immunity and make you more prone to developinfections such as chest infections.A small number of people with a CTCL will experience more general symptoms suchas unexplained weight loss, fevers or night sweats.How is skin <strong>lymphoma</strong> diagnosed?You would normally first go to your GP if you have red or itchy patches of skin or ifyou have developed lumps anywhere. Many skin <strong>lymphoma</strong>s look very like otherskin conditions such as eczema or psoriasis, which are much more common. Manyof them also develop very slowly, some over as long as 10–40 years. It can thereforebe months or even years before you are referred to a dermatologist, a specialist inskin diseases, or to a haematologist, who specialises in diseases of the blood andlymphatic system.In the hospital clinic, the consultant will ask you about how the skin problemdeveloped and about how it affects you – the history of the skin complaint. They willexamine the skin, looking carefully at the skin patches or lumps, and they might aska medical photographer to take photographs of your skin. They will also ask you aboutyour general health and about any other symptoms such as weight loss or fevers.Though the doctor might have a suspicion of what the problem is at this stage,the diagnosis would have to be confirmed by a skin biopsy. This short and simpleprocedure involves taking a small sample of an affected area of skin after it has beennumbed using a local anaesthetic. The sample will be examined under a microscope.It will also be sent for specialised tests to look at the <strong>cell</strong>s and the genes and proteinsin them in great detail. These tests sometimes have to be done in a laboratory inanother centre and results can take up to 2–3 weeks to come back.Making a diagnosis of skin <strong>lymphoma</strong> is not always straightforward, even once youhave been referred to a dermatologist or a <strong>lymphoma</strong> specialist. You might need morethan one skin biopsy over a period of several weeks or months. In some people theskin rash does not look typical of <strong>lymphoma</strong> and it is not unheard of for people to haveseveral biopsies taken over a number of years before a diagnosis is finally reached.This can be a frustrating and anxious time, but it is important that the doctors make anaccurate diagnosis and find out as much as possible about your particular <strong>lymphoma</strong>so that the most suitable treatment can be chosen.What tests might I need to assess the <strong>lymphoma</strong>?The history of how the skin problem developed and the examination of the skin,together with the results of the skin biopsy (or biopsies) will help the medical teamto make the diagnosis. In order to find out more about the <strong>lymphoma</strong> and how it isaffecting your body, you will also have a full physical examination and blood tests.This process of fuller assessment is known as ‘staging’ the <strong>lymphoma</strong> (the stages ofCTCL are described in more detail on page 8).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v35/18
When you are examined the doctor will feel your neck, under your arms and inyour groin area to detect any enlarged lymph nodes. You won’t need any internalexaminations. The blood tests will include blood <strong>cell</strong> counts and measurements of thelevels of some chemical substances that are found in the blood, including a chemicalcalled lactate dehydrogenase (LDH).The choice of which further tests you will have will depend on exactly which type of<strong>lymphoma</strong> the early tests show you have and on your general health. If you have themost common skin <strong>lymphoma</strong>, mycosis fungoides, and your physical examination andblood tests are normal the only other test you will have is a chest X-ray (and perhaps anultrasound examination).Scans are not done as commonly as they are in people with other non-Hodgkin<strong>lymphoma</strong>s. They might be done if other investigations suggest there are <strong>lymphoma</strong><strong>cell</strong>s in the blood or lymph nodes. The most common scan is computed tomography(CT) of the chest, abdomen and pelvis. Another scan called ‘positron-emissiontomography’ (PET), which is often combined with CT into a PET/CT scan, is done veryoccasionally. These scans show up your internal organs in great detail and can takeanything from 30 minutes to 2 hours to do. They are usually done as an outpatient,but they might have to be done at a larger medical centre than your local hospital. Youwould be given detailed instructions on all aspects of where to go and on preparing forand having these tests.A few people with suspected skin <strong>lymphoma</strong> will have a bone marrow biopsy,although this is more usual in people with cutaneous B-<strong>cell</strong> <strong>lymphoma</strong>s. In this testa small sample of bone marrow is taken from your hip bone using a needle. The skinover the bone is numbed first using a local anaesthetic and you will be given painkillersto help with any discomfort afterwards. The sample will be examined under themicroscope to see if it contains any <strong>lymphoma</strong> <strong>cell</strong>s.If enlarged lymph nodes are found when you are examined or if they are seen on thescans, a node might be removed so that it can be examined under the microscope – alymph node biopsy (sometimes called an ‘excision biopsy’). The node is removed in ashort operation under local anaesthetic or sometimes under general anaesthetic.All these tests are done to find out which parts of your body the <strong>lymphoma</strong> is affecting.They are also done to make sure that the <strong>lymphoma</strong> has definitely started in the skinitself and that it hasn't spread there from somewhere else. This is important because<strong>lymphoma</strong>s that start elsewhere, for example in the internal lymph nodes, behave quitedifferently and require different treatment. Once all the results are back, the medicalteam can decide on the best course of treatment for you.If you would like to talk to someone about your tests or would like moreinformation on blood tests, scans or bone marrow biopsy, please ring our helpline(0808 808 5555). Alternatively the information can be downloaded from ourwebsite (www.<strong>lymphoma</strong>s.org.uk).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v36/18
What do the tests tell the medical team?The appearance of your skin, together with the physical examination and all the testresults will usually provide:● a diagnosis of what type of skin <strong>lymphoma</strong> you have – whether it is a T-<strong>cell</strong> or aB-<strong>cell</strong> skin <strong>lymphoma</strong>, for example, and exactly which one● information on how the <strong>lymphoma</strong> is behaving – whether it is slow growing(low grade or 'indolent') or faster growing (high grade)● an indication of how much the <strong>lymphoma</strong> is affecting the body – the ‘stage’ of the<strong>lymphoma</strong>.It is important to know the type, grade and stage of a <strong>lymphoma</strong> so that the doctorswill have an idea of how it might behave in future and of how best to treat you.What do ‘low grade’ and ‘high grade’ mean?The skin biopsy will help the specialist to know how fast the lymphocytes are dividingand multiplying. Slow-growing <strong>lymphoma</strong>s are described as ‘low grade’ and fastergrowing <strong>lymphoma</strong>s as ‘high grade’. Most skin <strong>lymphoma</strong>s are slow growing. Thetable below divides the different types of CTCL into those that are slow growing andthose that develop and grow more rapidly. How fast the <strong>lymphoma</strong> is developing willbe an important factor in deciding which treatments would be most suitable and howsoon the treatment should be started.Slow-growing types of CTCL● Classic mycosis fungoides● Rarer types of mycosis fungoides:– folliculotropic mycosis fungoides– pagetoid reticulosis– granulomatous slack skin● Primary cutaneous CD30-positivelymphoproliferative disorders:●– primary cutaneous anaplasticlarge-<strong>cell</strong> <strong>lymphoma</strong>– <strong>lymphoma</strong>toid papulosisSubcutaneous panniculitis-like T-<strong>cell</strong><strong>lymphoma</strong>● Primary cutaneous CD4-positivesmall/medium T-<strong>cell</strong> <strong>lymphoma</strong>Faster growing types of CTCL● Sézary syndrome● Adult T-<strong>cell</strong> leukaemia/<strong>lymphoma</strong>● Extranodal NK/T-<strong>cell</strong> <strong>lymphoma</strong>, nasaltype● Primary cutaneous peripheral T-<strong>cell</strong><strong>lymphoma</strong>, unspecified● Primary cutaneous CD8-positiveaggressive epidermitropic cytotoxicT-<strong>cell</strong> <strong>lymphoma</strong>● Primary cutaneous gamma/delta T-<strong>cell</strong><strong>lymphoma</strong>You will find information about the different types of CTCL on pages 10–14.<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v37/18
What do the ‘stages’ mean?The stage of the <strong>lymphoma</strong> is an indication of how much the <strong>lymphoma</strong> is affecting thebody. Most CTCLs are at an early stage when they are diagnosed.Staging of mycosis fungoidesTo decide on the stage of mycosis fungoides the doctors will assess:● how the skin is affected – are there patches, plaques or swellings in the skin?● how much skin is affected● whether and how much the lymph nodes are affected● whether the <strong>lymphoma</strong> is present in any internal organs● whether abnormal <strong>lymphoma</strong> <strong>cell</strong>s (‘Sézary <strong>cell</strong>s’) can be detected circulating in thebloodstream and how many there are.Stages of mycosis fungoides and Sézary syndromeStage IThe <strong>lymphoma</strong> only affects the skin (patches or plaques):● stage IA means that less than a tenth of the skin is affected● stage IB means that a tenth or more of the skin is affectedStage IIStage II is divided into two, IIA and IIB:● stage IIA means that there are patches or plaques on the skin and thelymph nodes are enlarged but do not contain abnormal <strong>lymphoma</strong> <strong>cell</strong>s● stage IIB means that there are one or more raised lumps or ‘tumours’in the skin (the lymph nodes may or may not be enlarged but do notcontain <strong>lymphoma</strong> <strong>cell</strong>s)Stage IIIFour-fifths or more of the skin is affected, with general redness, swelling,itching and sometimes pain (erythroderma).The lymph nodes can beenlarged, but don't contain abnormal <strong>lymphoma</strong> <strong>cell</strong>s. Divided into:● stage IIIA if there are few or no <strong>lymphoma</strong> <strong>cell</strong>s in the bloodstream(erythrodermic mycosis fungoides)● stage IIIB if there are moderate numbers of <strong>lymphoma</strong> <strong>cell</strong>s in thebloodstream (Sézary syndrome)Stage IVIn stage IV disease there are skin problems and, in addition:● in stage IVA there are numerous abnormal <strong>lymphoma</strong> <strong>cell</strong>s inthe bloodstream (Sezary syndrome) or the lymph nodes contain<strong>lymphoma</strong> <strong>cell</strong>s● in stage IVB there is <strong>lymphoma</strong> in other organs<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v38/18
Stages IA, IB and IIA are considered to be ‘early stage’. Most people have thisstage of skin <strong>lymphoma</strong> when they are diagnosed. For others, the <strong>lymphoma</strong> is firstdetected at the more advanced tumour stages (stages IIB, III and IV) or, very rarely,when the blood is affected (stages IIIB or IVA, which is also called Sézary syndrome).The outlook or ‘prognosis’ depends on your age and general health and on how muchof your skin is affected. If less than a tenth of the skin is affected (ie stage IA) this isnot a life-threatening condition. Although it is rare for people with stage IA mycosisfungoides to remain completely and permanently clear after treatment, as long asthe <strong>lymphoma</strong> is controlled reasonably well it is unlikely to spread beyond the skin oraffect your life expectancy.If more than a tenth of the skin is involved or the <strong>lymphoma</strong> has involved the lymphnodes or other organs, remission is less likely to be so prolonged or permanent. The<strong>lymphoma</strong> can often be controlled for many years with treatment, however.Staging of other CTCLsThere are no recognised staging systems for the other, rarer CTCLs, but if youhave one of these other types of CTCL you might find that the medical team usesomething called the TNM system to describe your <strong>lymphoma</strong> stage. In this systemthey describe how much of the body is affected by assessing:● how many areas of changed skin there are, how big they are and which parts of thebody are affected (this is denoted by a ‘T’ and a number between 1 and 3)● how many lymph nodes are involved (if any) and which ones are involved (this isdenoted by an ‘N’ and a number between 0 and 3)● whether any other parts of the body are involved (ie parts that are not skin or lymphnodes, denoted by an ‘M’ and either 0 or 1).Changes in the TNM stage can help the medical team assess how well you areresponding to your treatment.Are skin <strong>lymphoma</strong>s curable?The grade of <strong>lymphoma</strong> – whether it is a slow-growing or a fast-growing type – andthe stage it is judged to be at when it is diagnosed are the two main factors that willdetermine how the <strong>lymphoma</strong> will behave, what kind of treatment you will need andhow the <strong>lymphoma</strong> is likely to respond to treatment. The table on page 7 listed whichCTCLs are considered to be slow-growing and which ones are usually faster growingand the stages were described on page 8.Strictly speaking, skin <strong>lymphoma</strong>s are not considered to be curable, but most skin<strong>lymphoma</strong>s never progress beyond the early stages. This is because they are often atan early stage when they are diagnosed, because they are slow-growing and becausethey respond well to treatment. If you have one of these skin <strong>lymphoma</strong>s the skinproblems will come and go and only need treatment some of the time. Having one ofthese types of <strong>lymphoma</strong> does not usually affect your life expectancy.<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v39/18
Some slow-growing <strong>lymphoma</strong>s do not become obvious until they are more advancedand the lymph nodes, blood or internal organs are affected. However, with treatment,many people with more advanced disease will also have long periods in remission,when they are free of symptoms of the disease.There are some skin <strong>lymphoma</strong>s that are faster growing and more aggressive intheir behaviour from the outset. These develop more rapidly and they require moreintense treatment, more urgently. In addition, some slow-growing skin <strong>lymphoma</strong>soccasionally change into a faster-growing type. This is called transformation and itis something the medical team check for when you attend the clinic. The treatmentwill become more intense if symptoms or follow-up tests have shown that this hashappened.The rest of the information sheet will describe the symptoms and treatments of thedifferent types of CTCL, starting with the most common type, mycosis fungoides.Mycosis fungoidesMost skin <strong>lymphoma</strong>s develop from T <strong>cell</strong>s and almost two-thirds of people with aT-<strong>cell</strong> skin <strong>lymphoma</strong> will have mycosis fungoides. This is therefore the most commonskin <strong>lymphoma</strong> overall. This <strong>lymphoma</strong> is a slow-growing or low-grade <strong>lymphoma</strong>and for many people it will not greatly affect their quality of life or alter their lifeexpectancy.Mycosis fungoides got its odd name because when it was first described at thebeginning of the 19th century the spots were thought to resemble a mushroom-likefungal disease. This is quite wrong of course because it is not caused by a fungus at all,but the name has stuck. The cause of mycosis fungoides is not known.This <strong>lymphoma</strong> occurs most commonly in people aged between 40 and 60 and itusually develops and progresses slowly over many years or even decades. Abouttwice as many men are affected as women. Most people with mycosis fungoides(about three-quarters) will have early-stage disease when they are first diagnosed.Most people have the ‘classic’ type (see below) and there are three other, rarer forms(see page 12).Classic mycosis fungoidesClassic mycosis fungoides starts as irregularly shaped, oval or annular (ring-like), dryor scaly patches, which are usually flat (see figures 1 and 2, pages 3 and 4). They canbe either discoloured or pale. They can disappear spontaneously, stay the same orslowly enlarge. These are most common on the trunk or buttocks but they can occuranywhere. They are often mistaken for other, more common skin conditions such aseczema or psoriasis, sometimes for many years. The face is only rarely affected.Sometimes similar but thicker and slightly raised areas of skin develop – plaques (seefigure 3, page 4). These plaques can be itchy and they sometimes ulcerate. The mostcommon places for plaques to appear on are the buttocks, in folds of skin and on theface. If they form in areas where there is hair, the hair can be lost. Mycosis fungoidescommonly never progresses beyond this early patch and plaque stage.<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v310/18
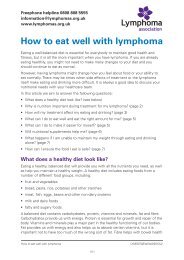
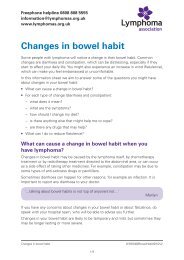
In a small proportion of people, raised lumps appear on the skin (tumours). Tumourscan ulcerate and weep and this can be painful (see figure 4, page 4).Figure 5: ErythrodermaIn a very few people the skincan become red, thickenedand sore all over. This is callederythroderma (see figure 5). If thishas happened it is likely that therewill be some <strong>lymphoma</strong> in thelymph nodes too, but mycosisfungoides does not usually involveother internal organs and is rarelyfound in the bone marrow.How is classic mycosis fungoides treated?Mycosis fungoides can be very effectively treated and well controlled, but it has atendency to come back when treatment is stopped. A few people need no treatmentat all at first but a good skincare regime with regular use of moisturisers will help toprevent dryness and irritation. This is all that will be required for some people withstage I disease.If larger areas of skin are affected or the itch is troublesome, mycosis fungoidescan be treated with treatments applied directly to the skin, such as steroid creams,phototherapy with PUVA (a psoralen tablet plus ultraviolet A light) or narrow-band UVB(ultraviolet B light) or topical chemotherapy drugs such as carmustine (BCNU). If tumourshave developed, these can be treated with radiotherapy.If the lymph nodes are involved, if the plaques and tumours are more extensive or ifthe topical treatments are not effective in early-stage disease, a combination of PUVAphototherapy and a drug called interferon alpha (injected just under the skin) or acombination of PUVA phototherapy and a retinoid drug such as bexarotene (Targretin ® )in tablet form might be given. Alternatively, total skin electron beam therapy (TSEBT)might be considered.If mycosis fungoides doesn’t respond to these treatments or if it is at a more advancedstage when it is diagnosed, the following treatments might be considered:● chemotherapy drugs such as methotrexate, chlorambucil, liposomal doxorubicin(Caelyx ® ) or gemcitabine● newer drugs such as the fusion toxin, denileukin diftitox (Ontak ® ) or the histonedeacetylase (HDAC) inhibitor, vorinostat● a combination of chemotherapy drugs (such ‘CHOP’, which is a combination oftenused for people with other types of <strong>lymphoma</strong>).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v311/18
Erythroderma can be treated by extracorporeal photopheresis (ECP). This is a typeof PUVA treatment where your blood (rather than your skin) is treated by ultraviolet Alight and then transfused back into you. Young, fit patients with advanced mycosisfungoides are sometimes treated with an allogeneic stem <strong>cell</strong> transplant.All these treatments and those mentioned below are described in much greaterdetail in the accompanying information sheet, ‘Treatments for skin <strong>lymphoma</strong>’.We also have information on allogeneic stem <strong>cell</strong> transplants. Please call thehelpline (0808 808 5555) if you would like this information or to talk about anyaspect of your skin <strong>lymphoma</strong>. Alternatively, you can download the informationfrom our website (www.<strong>lymphoma</strong>s.org.uk).Rarer forms of mycosis fungoides and how they are treatedApart from the classic form of mycosis fungoides there are three other, rarer formswhich behave slightly differently and look different when the skin biopsy is examinedunder the microscope:● Folliculotropic mycosis fungoides particularly affects hair follicles. This typecommonly affects the head and neck area and can cause some hair loss. It canappear as just one patch, plaque or tumour but most people have several. Inaddition people can have small cysts or blocked pore-like changes. This type ofmycosis fungoides is not very sensitive to topical therapies such as PUVA andtopical nitrogen mustard. Total-skin electron beam therapy, PUVA combined withretinoid drugs (eg Targretin ® ) or interferon might be considered, and radiotherapy issometimes used to treat tumours.● Pagetoid reticulosis (also known as Woringer–Kolopp disease): there is usually justone scaly plaque, often on an arm or leg, and this never spreads beyond the skin.Pagetoid reticulosis is treated by surgery or low doses of radiotherapy.● Granulomatous slack skin (GSS) is an extremely rare form of mycosis fungoidesin which loose folds of skin develop in the armpits and groins. There is no agreedstandard treatment regime for GSS, but surgery, radiotherapy, PUVA, steroidcreams and interferon can all be used to treat this condition.Sézary syndromeAbout 1 in 20 people with CTCL will have Sézary syndrome, which is closely related tomycosis fungoides but which affects the blood as well as the skin. Most people withSézary syndrome develop it without having had any milder form of skin <strong>lymphoma</strong>previously. Very few people with early-stage mycosis fungoides will go on to developSézary syndrome.Sézary syndrome is diagnosed if:● large areas of the skin are bright red, thickened, swollen and sore (erythroderma,see figure 5 on page 11),● there are abnormal lymphocytes in the lymph nodes (which might be enlarged), and● large numbers of abnormal lymphocytes (Sézary <strong>cell</strong>s) are found in the blood.<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v312/18
The skin can be extremely itchy and other problems that can occur are hair loss,ectropion (exposure of the inside surface of the lower eyelid) and thickening of theskin of the palms and the soles of the feet. The large number of <strong>lymphoma</strong> <strong>cell</strong>scirculating in the bloodstream means that the immune system doesn’t work as well asit should, so it is common for infections to develop.How is Sézary syndrome treated?Sézary syndrome does not just affect the skin – it affects the whole of the body. Thismeans that it needs to be treated with therapies that reach all parts of the body. Thefirst choice of treatment is usually extracorporeal photopheresis (ECP).Other treatments that can be given include low-dose methotrexate, bexarotene(Targretin ® ), interferon alpha, denileukin diftitox (Ontak ® ), the antibody alemtuzumab(Campath) and combination chemotherapy (eg CHOP). A combination of chlorambuciltablets and steroid tablets is sometimes prescribed. A topical treatment such as PUVAmight also be tried in addition to other treatments. Infections that develop are treatedwith antibiotics.There is more information on ECP and on the other treatments given for Sézarysyndrome in the article ‘Treatments for skin <strong>lymphoma</strong>’. Please call the helpline ifyou would like to receive this information (0808 808 5555) or download this fromour website (www.<strong>lymphoma</strong>s.org.uk).Primary cutaneous CD30-positive lymphoproliferativedisordersPrimary cutaneous anaplastic large-<strong>cell</strong> <strong>lymphoma</strong> and <strong>lymphoma</strong>toid papulosis aretwo slow-growing skin <strong>lymphoma</strong>s that together account for almost a third of all CTCLs.They are classed as 'primary cutaneous CD30-positive lymphoproliferative disorders'because the abnormal lymphocytes have a protein called CD30 on their surface.Primary cutaneous anaplastic large-<strong>cell</strong> <strong>lymphoma</strong> (ALCL)Primary cutaneous ALCL is most common in people in their 50s and 60s, though itcan occasionally occur in children. It is two or three times more common in men.It usually appears as just one single tumour on the skin, though sometimes thereis a collection of tumours on one area of skin. It usually appears on the trunk or onone limb and it can ulcerate. These <strong>lymphoma</strong>s can go away completely without anytreatment and it rarely spreads beyond the skin.If there is just one tumour, ALCL is usually treated by surgery or radiotherapy.Radiotherapy can also be used when there are a few tumours if they are confinedto one area. If there are more than this, methotrexate treatment or immunotherapydrugs might be advised. If it has affected nearby lymph nodes this can be treated withcombination chemotherapy.<strong>Lymphoma</strong>toid papulosis (LyP)LyP is an indolent skin <strong>lymphoma</strong> that does not affect your life expectancy. It comesand goes and often does not require any treatment at all. It is seen in slightly younger<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v313/18
people, the average age being about 45. Again, it is more common in men. Crops ofpapules or bigger lumps (nodules), which are often ulcerated in the middle, appearover a period of a few days, usually on an arm or leg or on the trunk. They usually healup over a period of 3–12 weeks, but they can persist for longer than this, and they canleave behind superficial scars. About 1 in 20 people with LyP also develop anothertype of <strong>lymphoma</strong> as well (such as cutaneous ALCL, mycosis fungoides or Hodgkin<strong>lymphoma</strong>).No treatment has been shown to change the course of LyP but several of the topicaltreatments, including PUVA and steroid creams, can be used if the nodules areparticularly troublesome. If LyP ‘attacks’ are very frequent or severe, some centrestreat this <strong>lymphoma</strong> with low doses of methotrexate.Rarer cutaneous T-<strong>cell</strong> <strong>lymphoma</strong>sSubcutaneous panniculitis-like T-<strong>cell</strong> <strong>lymphoma</strong> (SPTCL) is a slow-growing<strong>lymphoma</strong> that can occur at any age. It is slightly more common in women than it isin men. It starts in the fatty layer of the skin, just below the surface, and shows upas one or more plaques or nodules, often on the legs. Some people will have othermore general symptoms and signs, such as fevers, low blood counts and weightloss. SPTCL is often treated successfully with steroid tablets. If additional treatmentis required, local radiotherapy or chemotherapy with doxorubicin can be used.Combination chemotherapy (eg with CHOP) or even a stem <strong>cell</strong> transplant might beconsidered if SPTCL is behaving in a more aggressive way.Primary cutaneous CD4-positive small/medium T-<strong>cell</strong> <strong>lymphoma</strong> usually appearsas a single plaque or nodule on the face, neck or upper trunk. It is a slow-growing<strong>lymphoma</strong> with a good outlook. The plaque or nodule is usually removed surgically ortreated with radiotherapy. If the <strong>lymphoma</strong> is more widespread, cyclophosphamide orinterferon alpha might be suggested as treatment.Primary cutaneous gamma/delta T-<strong>cell</strong> <strong>lymphoma</strong> is a faster growing type of skin<strong>lymphoma</strong> that usually shows up as patches and plaques, most commonly on thearms or legs. It usually occurs in adults. Many people with this <strong>lymphoma</strong> experiencenight sweats, fevers and weight loss. Sometimes the blood counts are low and theliver and spleen can become enlarged.Primary cutaneous CD8-positive aggressive epidermitropic cytotoxic T-<strong>cell</strong><strong>lymphoma</strong> is another faster growing <strong>lymphoma</strong>. It occurs mainly in adults. It appearsas widespread papules and plaques and tumours on the skin, which can ulcerate. Itcan also affect the lining of the mouth.These last two skin <strong>lymphoma</strong>s are often treated using a combination of chemotherapydrugs and sometimes a stem <strong>cell</strong> transplant is considered.There is more information on these treatments in the article, ‘Treatments forskin <strong>lymphoma</strong>’. We also have information on stem <strong>cell</strong> transplants. Please callthe helpline if you would like to receive this information (0808 808 5555) ordownload it from our website (www.<strong>lymphoma</strong>s.org.uk).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v314/18
Taking part in a clinical trialResearchers are continually trying to find out which treatment or combination oftreatments work best for <strong>lymphoma</strong>s. You might be asked to take part in a clinicalresearch trial. Clinical trials are very important because they allow new treatments tobe evaluated and compared with more established ones. Studying treatments like thisis the only way that new and hopefully better treatments can become available. Whenyou are enrolled into a clinical trial you can be assured that you will receive modernand appropriate treatments.There are advantages to taking part in a clinical trial and it is always worth asking yourconsultant if there might be a trial you could take part in. A major advantage is thatsome of the newer treatments are only available if you are in a clinical trial.You don’t have to take part in a trial if you are offered this, however. If you don’t feelcomfortable with the idea of taking part in a trial after discussing all the optionswith your medical team be assured that you will receive the best current standardtreatment available.We have booklet about taking part in clinical trials. If you would like a copy of thisor if you would like to talk to someone about entering a trial please phone thehelpline (0808 808 5555). The booklet can also be downloaded from our website(www.<strong>lymphoma</strong>s.org.uk).Going for hospital check-upsHow often you attend the clinic for check-ups will depend on what kind of <strong>lymphoma</strong>you have, the stage it is assessed to be at and how it is responding to treatment. Ifyou have a slow-growing <strong>lymphoma</strong> at an early stage and it is being observed, or if itis stable or in remission after treatment you would probably only be seen every 6 to12 months. This would probably be your experience if you have mycosis fungoides.If your <strong>lymphoma</strong> is a faster growing type or is continuing to grow (progressing) youmight be seen as often as every 4 to 6 weeks.At the clinic you will be asked about your symptoms and you will be examined.Always let the medical team know if there are any symptoms that have been troublingyou or about any changes in your skin or new swellings that have developed. Youwould only occasionally need blood tests, scans or further biopsies at these visits.You might like to read our other information sheets on skin <strong>lymphoma</strong>s,‘Treatments for skin <strong>lymphoma</strong>s’ and ‘Living with skin <strong>lymphoma</strong>’, whichdescribes ways of coping with the symptoms and other day-to-day practicalitiesof having skin <strong>lymphoma</strong>. If you would like these or if you have any concernsthat you would like to discuss, please phone our helpline (0808 808 5555).This information is also available on our website (www.<strong>lymphoma</strong>s.org.uk).<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v315/18
AcknowledgementsWe are very grateful to our expert advisors and to all the people with skin <strong>lymphoma</strong>who helped us in the development of this information, in particular:o Dr Eileen Parry, Consultant Dermatologist at Tameside Hospital NHS FoundationTrust, Manchestero Jane Gibson, <strong>Lymphoma</strong> Clinical Nurse Specialist at The Christie NHS FoundationTrust, Manchestero Professor Richard Cowan, Consultant in Clinical Oncology at The Christie NHSFoundation Trust, Manchestero Ashley Medicks of Skinship (UK).The clinical photographs used in the figures were courtesy of The Christie NHSFoundation Trust, Manchester.Useful organisationsBritish <strong>Association</strong> of DermatologistsProvides a range of patient information leaflets, including one on mycosis fungoidesand several on treatments for skin <strong>lymphoma</strong>s 0207 383 0266 admin@bad.org.ukwww.bad.org.ukCancerHelp UKCancerHelp UK is the patient information website of Cancer Research UK andprovides information on cancers and <strong>lymphoma</strong>s. 0808 800 4040 (Monday–Friday, 9am–5pm) via websitewww.cancerhelp.org.uk<strong>Cutaneous</strong> <strong>Lymphoma</strong> FoundationA US-based international organisation that provides support and comprehensiveinformation for anyone affected by cutaneous <strong>lymphoma</strong>.www.clfoundation.orgDermNet NZDermNet NZ is the website of the New Zealand Dermatological Society Incorporated.Produces detailed, illustrated information about skin conditions including skin<strong>lymphoma</strong>s for patients and health professionals. Endorsed by the British <strong>Association</strong>of Dermatologists.www.dermnetnz.orgLeukaemia & <strong>Lymphoma</strong> ResearchDedicated exclusively to researching blood cancers, including leukaemia, <strong>lymphoma</strong>and myeloma. 020 7504 2200 (Mon–Fri, 9am–5pm) info@beatingbloodcancers.org.ukwww.leukaemia<strong>lymphoma</strong>research.org.uk<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v316/18
Macmillan Cancer SupportProvides practical, medical, emotional and financial help, as well as comprehensiveinformation on all aspects of cancers, treatments and living with cancer. 0808 808 0000 via websitewww.macmillan.org.ukSkinship (UK)A confidential dermatology helpline that supports anyone affected by a skin conditionand lobbies for improved dermatology training in the UK. Run by Ashley Medicks, whohas had mycosis fungoides for over 40 years. 01387 760 567 amedicks321@btinternet.comwww.careinfoscotland.co.uk/system/full-record.aspx?id=414ReferencesPerry MC (editor). The Chemotherapy Source Book. 4th edition. 2008. Lippincott,Williams & Wilkins. Philadelphia, USA.Swerdlow SH, et al. World Health Organization classification of tumours: pathologyand genetics of tumours of haematopoietic and lymphoid tissues. 2008. IARC Press,Lyon, France.Marcus R, et al (eds). <strong>Lymphoma</strong>: pathology, diagnosis and treatment. 2007.Cambridge University Press, Cambridge, UK.Willemze R, Dreyling M, and the ESMO Guidelines Working Group. Primary cutaneous<strong>lymphoma</strong>s: ESMO Clinical Practice Guidelines for diagnosis, treatment and followup.Annals of Oncology, 2010. 21(Suppl 5): v177–v180. Available at: http://annonc.oxfordjournals.org/content/21/suppl_5/v177.full (accessed 5 April 2013).Prince HM, et al. How I treat mycosis fungoides and Sézary syndrome. Blood, 2009.114: 4337–4353.Scarisbrick J. Extracorporeal photopheresis: what is it and when should it be used?Clinical and Experimental Dermatology, 2009. 34:757–760.Kim YH, et al., ISCL/EORTC. TNM classification system for primary cutaneous<strong>lymphoma</strong>s other than mycosis fungoides and Sézary syndrome: a proposal of theIntenational Sociaty for <strong>Cutaneous</strong> <strong>Lymphoma</strong>s (ISCL) and the <strong>Cutaneous</strong> <strong>Lymphoma</strong>Study Group of the European Organization of Research and Treatment of Cancer(EORTC). Blood, 2007. 110: 479–484.Olsen E, et al., ISCL/EORTC. Revisions to the staging and classification of mycosisfungoides and Sezary syndrome: a proposal of the International Society for <strong>Cutaneous</strong><strong>Lymphoma</strong>s (ISCL) and the cutaneous <strong>lymphoma</strong> task force of the EuropeanOrganization of Research and Treatment of Cancer (EORTC). Blood, 2007. 110: 1713–1722.Trautinger F, et al. EORTC consensus recommendations for the treatment of mycosistungoides/Sézary syndrome. European Journal of Cancer, 2006. 42: 1014–1030.<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v317/18
Willemze R, et al. WHO-EORTC classification for cutaneous <strong>lymphoma</strong>s. Blood, 2005.15; 105: 3768–3785.Haghighi B, et al. Pagetoid reticulosis (Woringer-Kolopp disease): animmunophenotypic, molecular, and clinicopathologic study. Modern Pathology, 2000.13: 502–510.Diamandidou E, et al. Transformation of mycosis fungoides/Sézary syndrome: clinicalcharacteristics and prognosis. Blood, 1998: 92: 1150–1159.How we can help youWe provide:● a freephone helpline providing information and emotional support 0808 808 5555(9am–6pm Mondays–Thursdays; 9am–5pm Fridays) or information@<strong>lymphoma</strong>s.org.uk● information sheets and booklets about <strong>lymphoma</strong> (free of charge)● a website with forums – www.<strong>lymphoma</strong>s.org.uk● the opportunity to be put in touch with others affected by <strong>lymphoma</strong> through ourbuddy scheme● a nationwide network of <strong>lymphoma</strong> support groups.How you can help usWe continually strive to improve our information resources for people affected by <strong>lymphoma</strong>and we would be interested in any feedback you might have on this article. Please visitwww.<strong>lymphoma</strong>s.org.uk/feedback or email publications@<strong>lymphoma</strong>s.org.uk if you haveany comments. Alternatively please phone our helpline on 0808 808 5555.We make every effort to ensure that the information we provide is accurate but itshould not be relied upon to reflect the current state of medical research, which isconstantly changing. If you are concerned about your health, you should consultyour doctor.The <strong>Lymphoma</strong> <strong>Association</strong> cannot accept liability for any loss or damage resultingfrom any inaccuracy in this information or third party information such asinformation on websites which we link to. Please seeour website (www.<strong>lymphoma</strong>s.org.uk) for moreinformation about how we produce our information.© <strong>Lymphoma</strong> <strong>Association</strong>PO Box 386, Aylesbury, Bucks, HP20 2GARegistered charity no. 1068395Updated: April 2013Next planned review: 2015<strong>Cutaneous</strong> T-<strong>cell</strong> <strong>lymphoma</strong>LYM0157/CTCL/2013v318/18