The esthetic zone of smile - Virtual Journal of Orthodontics
The esthetic zone of smile - Virtual Journal of Orthodontics
The esthetic zone of smile - Virtual Journal of Orthodontics

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
function outcomes. <strong>The</strong> firstmeasurable assessment was madeby Andrew by his ‘Six keys tonormal occlusion’ which couldmeasure the final outcome <strong>of</strong> thetreatment and which became afuture foundation for developingpreadjusted appliance system withvarying degrees <strong>of</strong> tip and torquevalues 3 .It must be understood thatthere is no universal “ideal” <strong>smile</strong>.<strong>The</strong> most important <strong>esthetic</strong> goalin orthodontics is to achieve a“balanced” <strong>smile</strong>, which can bestbe described as an appropriatepositioning <strong>of</strong> the teeth andgingival scaffold within thedynamic display <strong>zone</strong> 4 .As mentioned above, this includeslateral, vertical, andanteroposterior aspects, as well asthe cant <strong>of</strong> the maxillary anteriortransverse occlusal plane and thesagittal cant <strong>of</strong> the maxillaryocclusal plane. Smile design andmechanotherapy must be builtaround this <strong>esthetic</strong> plane <strong>of</strong>occlusion, which is <strong>of</strong>ten differentfrom the natural plane <strong>of</strong>occlusion. <strong>The</strong> first considerationin obtaining a consonant <strong>smile</strong> arc,or preserving an already consonant<strong>smile</strong> arc, is bracketpositioning .Smile design alsonecessitates changes in overalltreatment mechanics. In cases withhigh labial ectopic maxillarycanines, for instance, levelling witha continuous archwire will intrudethe maxillary central and lateralincisors and thus flatten the <strong>smile</strong>arc .For such cases segmentedarchtechnique using cantileversprings <strong>of</strong>fers better control <strong>of</strong>levelling and <strong>of</strong> the a<strong>esthetic</strong> plane<strong>of</strong> occlusion. Creating attractive<strong>smile</strong> depends upon factors likewhether the problem is dental orskeletal, any periodontal disease,missing teeth, etc .During thiscourse <strong>of</strong> action an orthodontistmay spend much time in detailingas was spent for major correctionslike skeletal discrepancy, severecrowding, space closure androtations .Frequently the patientsbecome impatient because <strong>of</strong> therequirement <strong>of</strong> the second andthird order changes in buccalsegment 3 . For this role <strong>of</strong> bracketselection and placement plays avery important role 3 . People with anormal dental appearance arejudged more socially attractiveover many personal characteristicsthan those with malocclusions.Those with poor dental <strong>esthetic</strong>shave been linked to lack <strong>of</strong> selfconfidenceand are thought to bedisadvantaged in social,educational, and occupationalsettings 4 . Though, various authorshave written extensively in theliterature regarding the importance<strong>of</strong> various factors to be consideredin aspect to <strong>smile</strong> designing. Thisarticle reviews concepts andprinciples <strong>of</strong> <strong>smile</strong> <strong>esthetic</strong>s inorthodontic treatment that shouldlend <strong>esthetic</strong>s to the entireor<strong>of</strong>acial complex involving unity,form, colour, function and display<strong>of</strong> dentition.Clinical Evaluation<strong>The</strong> most important aspect <strong>of</strong> theclinical assessment is for theclinician to know what to evaluate13
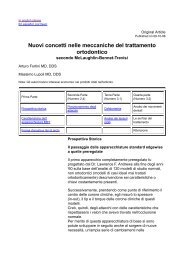
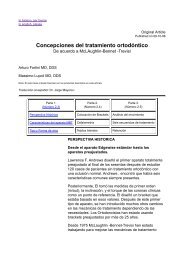
image size). <strong>The</strong> resulting numberwas copied and pasted in place <strong>of</strong>the width reading, and the changeswere applied to the JPEG file.Evaluation <strong>of</strong> <strong>smile</strong> design is tobe considered under followingclinical evaluation;1) Dento-facial analysisFig 1 - Video camera set on atripod at 4 feet distance from thesubject in sitting position2) Dental analysisTooth analysisTooth and lip analysisStandardization <strong>of</strong> image<strong>The</strong> frames can be edited in avideo editing s<strong>of</strong>tware (DVD videos<strong>of</strong>t studio) This converts the videointo JPEG. <strong>The</strong>n, each JPEG file <strong>of</strong>the selected subjects can beopened in Adobe Photoshop CS2(Adobe Systems, San Jose,California) and then adjusted byusing the ruler option in the frame.<strong>The</strong> method used to standardizethe image was as described byDesai et al 7 First, the resolutionwas changed to 300 pixels per inchby going to ‘‘image > image size.’’<strong>The</strong>n, the ruler function waschosen and set to millimeter whichcan measure a minimum <strong>of</strong> 0.1mmlength. On the parallel end <strong>of</strong> theruler, a 10-mm area, close to the<strong>smile</strong>, was measured. That numberwas divided into 10 (10/measurement on JPEG file) andmultiplied by the width value foundin image size screen (image >Tooth and gingivalanalysisDENTO-FACIAL ANALYSISMidline DiscrepancyIdeally, the dental midline shouldbe in align with the facial midlinebut usually it does not. As long asthe midline is parallel with the longaxis <strong>of</strong> the face, midlinediscrepancies <strong>of</strong> up to 4 mm willgenerally not be perceived asun<strong>esthetic</strong>. Slight corrections <strong>of</strong>midlines can be accomplished withrestorative dentistry as long as themaxillary centrals are maderelatively symmetric and correctintertooth relationships aremaintained. If the individual teethdo not require restoration andthere is a large midlinediscrepancy, the ideal treatment isorthodontic treatment. One shouldalso check the s<strong>of</strong>t tissueattachment hindering the closure<strong>of</strong> midline diastema 6 (fig2)15
Fig 2- Midline diastema greaterthan 4mm requires orthodontictreatmentDENTAL ANALYSISTooth analysisbeen discussed in the literature tobe between 70% to 80% 8 .Smileswith these values were most <strong>of</strong>tendeemed “<strong>esthetic</strong> to highly<strong>esthetic</strong>.” <strong>The</strong> most <strong>esthetic</strong>allypleasing ratio was 80%. It isextremely important to note thatthe <strong>esthetic</strong> perception <strong>of</strong> widthto-lengthratios is significantlyaffected by the outline form andthe reflective surface <strong>of</strong> the tooth.<strong>The</strong> lateral incisors are between 1mm to a maximum <strong>of</strong> 2.5 mmshorter than the central 8 . For amore petite <strong>smile</strong>, more toward the2 mm to 2.5 mm length isrecommended. <strong>The</strong> canine isslightly shorter than the centralbetween 0.5 to 1 mm 8 .<strong>The</strong> next step is to evaluate therelationship <strong>of</strong> the lips to the teeth,ie, visual tooth display bothstatically and dynamically 7 .Intratooth evaluation<strong>The</strong> average length for maxillarycentral incisors has been measuredat between10 mm to 11 mm.Patients who seek <strong>esthetic</strong>s as aprimary reason for treatment wantto have a full <strong>smile</strong> with “aboveaverage” looking teeth. Acc toEdward Larren 8 the <strong>esthetic</strong> <strong>zone</strong>for the central incisor to bebetween 10.5 mm and 12 mm. Agood length to start the design is11 mm, as it can be modifiedbased on the many other treatmentplanning parameters. <strong>The</strong> widthto- length <strong>esthetic</strong> relationship hasContacts, connectors, andEmbrasure Morphology<strong>The</strong> elements <strong>of</strong> tooth contacts,connectors, and embrasures can be<strong>of</strong> real significance in planning thetreatment <strong>of</strong> the <strong>smile</strong>. Contacts(interdental contact points) aredefined as the exact place that theteeth and touch (what makes flosssnap). <strong>The</strong> connector (also referredto as the interdental contact area)is where the incisors and canines“appear” to touch. <strong>The</strong> contactpoints progress apically as theteeth proceed from the midline tothe posterior. <strong>The</strong> connector heightis greatest between the centralincisors and diminishes from the16
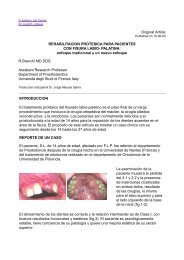
central to the posterior teeth. <strong>The</strong>embrasures (the triangular spaceincisal to the contact) ideally arelarger as the teeth progressposteriorly. <strong>The</strong> shape <strong>of</strong> the spacebetween your teeth called theembrasure <strong>The</strong>se should beconsider before finishing thecontacts as they can be to wide ornarrow 10 .(fig 3 and 4)Fig 3-embrasures can be too wide or narrowgiving unesthethic appearanceFig 4- Contact between anterior teeth iswhere teethactually touch; connector iswhere teeth appear to touch. Embrasures aresmallest between central incisors and growlarger as they progress posteriorly indentitionIntertooth evaluationTooth proportionality and GoldenratioWhen a person <strong>smile</strong>s and theteeth are displayed, there is anintertooth relationship that needsto be maintained for thecomposition to be considered<strong>esthetic</strong>. <strong>The</strong> maxillary centralincisors should be relatively butnot perfectly symmetrical. <strong>The</strong>yshould dominate but notoverwhelm the <strong>smile</strong> 8 .This isobviously very subjective, butresearch has shown that in <strong>smile</strong>sdetermined to be <strong>esthetic</strong>, therewas a clear dominance <strong>of</strong> themaxillary central incisor. Minooetal 9 had suggested that thegolden proportion was not thesame perceived maxillary anteriorteeth widths <strong>of</strong> individuals with an<strong>esthetic</strong> <strong>smile</strong> and concluded thatdue to variety in nature, <strong>esthetic</strong>sin dentistry cannot be justifiedmathematically; individuals shouldnot be standardized in the sameway . Though many authorsrecommend using the goldenproportion to define the opticalwidth <strong>of</strong> the maxillary teeth as theygo posteriorly many studies hasdemonstrated that the actualmeasurements <strong>of</strong> most people’santerior teeth do not in fact followthe golden proportion. It has notbeen determined that if a person’soptical tooth display followed thegolden proportion that this beconsidered more <strong>esthetic</strong> thanother arrangements. Acc to EdwardLarren 8 experience, the relationhip<strong>of</strong> the maxillary lateral to centralincisor comes very close to thegolden proportion in an <strong>esthetic</strong><strong>smile</strong>, and can be used as a guidein shaping teeth 9 . A good guide isto make the optical width <strong>of</strong> thelateral incisor about 65% <strong>of</strong> thecentral incisor (or a little less thantwo thirds).<strong>The</strong> canine does notfollow the golden proportionoptically and is generally about75% to 80% or about three fourthsto four fifths <strong>of</strong> the optical width <strong>of</strong>17
the lateral incisor in <strong>smile</strong>s thatwere considered highly <strong>esthetic</strong>,with an <strong>esthetic</strong>ally acceptable<strong>zone</strong> from 70% to 85% (fig 5 and 6)Fig 5–<strong>The</strong> golden proportionmust be maintained so as to getthe best esthethicsFig 6- Width to length ratio isnot the same and esthethicpercentages is does not followsthe golden proportion 8Tooth and lip analysisIncisor exposure and Smile LinePublished reports have shown thatthe average 30-year-old womandisplays about 3.5 mm <strong>of</strong>maxillary central incisor toothstructure when the lips are at rest<strong>The</strong> prosthodontic literature hasgenerally recommended settingdenture teeth so that 2 mm <strong>of</strong>tooth structure is displayed at rest.In the author’s experience, the 2mm exposed at rest is generallyless than desired by <strong>esthetic</strong>allydriven patients , for most patientswho have improved <strong>esthetic</strong>s astheir primary treatment goal,between 3 mm and 4 mmdisplayed at rest will be <strong>esthetic</strong>allyideal. Another guide for evaluatingthe <strong>esthetic</strong> position <strong>of</strong> themaxillary anterior incisal edgesapplies when the patient <strong>smile</strong>s; inan <strong>esthetic</strong> composition, the tips <strong>of</strong>the maxillary anterior teeth comevery close to touch the lower lip upto a maximum <strong>of</strong> 3 mm away .<strong>The</strong><strong>esthetic</strong> treatment would be toreposition the incisal edges <strong>of</strong> themaxillary anterior teeth withinthese two dentolabial <strong>esthetic</strong><strong>zone</strong>s. <strong>The</strong> modality <strong>of</strong> treatmentwould be determined inconjunction with the evaluation <strong>of</strong>all the other <strong>smile</strong> design andtreatment goal parameters. Ifpatients display less than 4 mm <strong>of</strong>the maxillary central at rest andthe teeth need to be lengthened,the length will generally beachieved by adding to the incisaledge. In an <strong>esthetic</strong> <strong>smile</strong>, theedges <strong>of</strong> the maxillary anteriorteeth follow a convex or gull-wingcourse matching the curvature <strong>of</strong>the lower lip and are generallyradially parallel to the horizon.From a frontal view, the maxillaryarch from central to molar appearsto curve upward, but not always. Ifit does, this apparent curve may be18
a result <strong>of</strong> a slight posterior cant tothe maxilla or the frequentappearance <strong>of</strong> the Curve <strong>of</strong> Spee inthe intact dentition. Slight tomoderate deviations to this patterncan be effectively treated with<strong>esthetic</strong> recontouring orconservative restorative dentistry.In situations where there is idealtooth form and color but there arediscrepancies to the <strong>smile</strong> line orvisual tooth display, restorativedentistry is not indicated, as thiswould cause unnecessarymutilation <strong>of</strong> otherwise healthytooth structure. In these clinicalsituations, and when there ismoderate to severe distortion <strong>of</strong>the <strong>smile</strong> line, orthodontics wouldbe the more appropriatetreatment 10 .(fig 7)Fig 7- Incisors exposure and<strong>smile</strong> line Transverse narrowing <strong>of</strong> themaxilla, especially in the premolarregion. Expansion <strong>of</strong> the maxillaryarch is required in order to fill thecorners <strong>of</strong> the <strong>smile</strong>. Palatal angulation <strong>of</strong> themaxillary posterior dentition.Increased palatal root torque and/or expansion <strong>of</strong> the posteriormaxillary dentition, primarily thepremolar region, are required. Incosmetic dentistry, an increase inthe thickness <strong>of</strong> the buccal aspect<strong>of</strong> ceramic restorations on thepremolar teeth may help to fill outthe <strong>smile</strong>. Retro-positioned maxilla.Maxillary advancement is thetreatment <strong>of</strong> choiceA broad <strong>smile</strong> with a minimalbuccal corridor is deemed most<strong>esthetic</strong> by lay people;however, abroad <strong>smile</strong> without a buccalcorridor could also be perceived asfake.If the space appears excessivewhen the patient is smiling, a smallamount <strong>of</strong> the contours <strong>of</strong> themaxillary posterior restorations—assuming restorations need to beplaced for restorative reasons. Ifconservative additive or subtractive(ie, <strong>esthetic</strong> contouring) techniqueswill not work <strong>esthetic</strong>ally, thenorthodontics should beconsidered 14 .(fg 8)Dark Buccal CorridorIn an <strong>esthetic</strong> <strong>smile</strong> there is whathas been termed negative space,which is a small space between themaxillary posterior teeth and theinside <strong>of</strong> the cheek 13 . <strong>The</strong> presence<strong>of</strong> dark buccal corridors may bedue to:Fig 8– Right and left buccalcorridors must be considered19
<strong>The</strong> vertical exposure <strong>of</strong> themaxillary incisors in relation to theupper lip at rest should be 2−4mm, and on smiling the entirecrown <strong>of</strong> the maxillary incisorsshould be exposed, with up to 1−2mm <strong>of</strong> associated gingiva. Aspontaneous <strong>smile</strong>, which isinvoluntary and expresses joyousemotion, tends to raise the upperlip slightly more than a posed<strong>smile</strong>, which is voluntary .DENTO-GINGIVAL ANALYSIS<strong>The</strong> lips frame the teeth andgingiva. <strong>The</strong> gingiva frames theteeth. <strong>The</strong> ratio <strong>of</strong> tooth structureto the amount <strong>of</strong> gingival andlabial tissue should be harmonizedto prevent an over-dominance <strong>of</strong>any one element. <strong>The</strong> verticalaspects <strong>of</strong> <strong>smile</strong> anatomy are thedegree <strong>of</strong> maxillary anterior toothdisplay (Morley ratio), upper lipdrape, and gingival display. In ayouthful <strong>smile</strong>, 75-100% <strong>of</strong> themaxillary central incisors should bepositioned below an imaginary linedrawn between the commissures.(fig 9)Fig 9 – a; acceptable morley ratiob; excessive display <strong>of</strong> incisorsOther factors to consider indesigning <strong>esthetic</strong> gingivalrelationships are: gingival line (therelationships <strong>of</strong> free gingivalmargins <strong>of</strong> the maxillary teeth),gingival scalloping and contour,papillary tip positioning, andgingival colorGingival Line and its Zenith<strong>The</strong> key <strong>esthetic</strong> issue is that thegingival line for the anterior teethshould be relatively horizontal tothe horizon and relativelysymmetric on both sides <strong>of</strong> themidline. It may radiate up slightlyas it goes posterior. It is not criticalthat the lateral incisor gingival linefall incisal to the central as this isnot obvious when a person issmiling. Positioning the lateral tothe central incisor within 0.5 mmgingivally and 1 mm incisally isgenerally perceived as <strong>esthetic</strong> aslong as horizontal symmetry ismaintained. <strong>The</strong> contour <strong>of</strong> thegingival (ie, gingival scallop) to thetip <strong>of</strong> the papilla should bebetween 4 mm or 5mm and thetips <strong>of</strong> the papillae should have the20
same radiating symmetry as theincisal edges and the free gingivalmargins. In an <strong>esthetic</strong> <strong>smile</strong>, thevolume <strong>of</strong> the gingiva from theapical aspect <strong>of</strong> the free gingivalmargin to the tip <strong>of</strong> the papilla isabout 40% to 50% <strong>of</strong> the length<strong>of</strong> the maxillary anterior tooth andfully fills the gingival embrasure .Insituations where this conditiondoes not exist, periodontal andorthodontic procedures are thetreatments <strong>of</strong> choice to create thecorrect gingival architecture.<strong>Orthodontics</strong> not only positions theteeth but also can repositiongingiva and bone. Gingival colorshould appear pink and healthy orconsistent with the healthy color <strong>of</strong>individual race variations 15,16 .(fig10)According to the accreditationcriteria for the American Academy<strong>of</strong> Cosmetic Dentistry, “<strong>The</strong>gingival shape <strong>of</strong> the mandibularincisors and the maxillary lateralsshould exhibit a symmetricalhalfoval or half-circular shape. <strong>The</strong>maxillary centrals and caninesshould exhibit a gingival shapethat is more elliptical. Thus, thegingival zenith (the most apicalpoint <strong>of</strong> the gingival tissue) islocated distal to the longitudinalaxis <strong>of</strong> the maxillary centrals andcanines (Fig 11). <strong>The</strong> gingivalzenith <strong>of</strong> the maxillary laterals andmandibular incisors shouldcoincide with their longitudinalaxis 16 .Fig 10 -Ideal gingival scallop 8Two concepts <strong>of</strong> cosmetic dentistrythat are important to the final<strong>esthetic</strong> outcome <strong>of</strong> orthodonticpatients are gingival shape andgingival contour. In cosmeticdentistry, care is taken in theassessment <strong>of</strong> the gingivalarchitecture for the anterior teethto have certain characteristics.Gingival shape refers to curvature<strong>of</strong> the gingival margin <strong>of</strong> the tooth,determined by the cementoenameljunction and the osseous crest.Fig 11- Gingival shape refers tocurvature <strong>of</strong> gingival margin <strong>of</strong>tooth. Gingival zenith (mostapical point <strong>of</strong> gingival tissue) isdistal to longitudinal axis <strong>of</strong>maxillary central incisors andcanines. Gingival zenith <strong>of</strong>maxillary lateral incisors shouldcoincide with their longitudinalaxis.Conclusion21
Today, various protocols <strong>of</strong> <strong>smile</strong>design are available. However,most clinicians wish to use thesimplest protocol with the mostpredictable results. It is to benoted that <strong>smile</strong> design shouldalways be a multifactorial decisionmakingprocess that allows theclinician to treat patients with anindividualised and interdisciplinaryapproach. <strong>The</strong> Esthethic <strong>zone</strong> <strong>of</strong><strong>smile</strong> presented in this articleclearly indicates the mostimportant components <strong>of</strong> <strong>smile</strong>design, their clinical significanceduring the <strong>smile</strong> design procedure.I believe that the maintain theesthethic <strong>zone</strong> through theseparameters is a simple andpractical that can help the clinicianto easily comprehend the‘complex’ <strong>smile</strong> design procedures<strong>of</strong> orthodontics.References1- Tjan AHL, Miller GD. Some <strong>esthetic</strong> factorsin a <strong>smile</strong>. J. Prosthet. Dent. 1984; 51:24-8.2- Grove Philip. Webster’s Internationaldictionary <strong>of</strong> the English language, Ed. 14,Springfield, Mass, 1961, G and C. MerriamCompany Publishers, II,21513- Anoop sondi; the implications <strong>of</strong> Bracketselection and Bracket Placement onFinishing details ;Seminars in<strong>Orthodontics</strong> ;2001;9;155-1644- Marc b. Ackerman; james l. Ackerman, ;<strong>smile</strong> analysis and design in the digitalera; journal <strong>of</strong> clinical orthodontics ;2002;volume xxxvi ; 4;231-2365- Moorrees CFA, Kean MR. Natural headposition: a basic consideration in theinterpretation <strong>of</strong> cephalometricradiographs. Am J Phys Anthropol; 1958;16: 213−2346- Farhad B Naini;Daljit S gill; FacialA<strong>esthetic</strong>s: Clinical Aessement ; DentUpdate 2008; 35: 159-1707- Shyam Desai, Madhur Upadhyay, andRavindra Nanda. Dynamic <strong>smile</strong> analysis:Changes with age. Am. J. Orthod.Dent<strong>of</strong>ac. Orthop. 2009;136:310.e1-310.e108- Edward A. McLaren,Smile Analysis andEsthetic Design:“In the Zone”; Insidedentistry; 2009;july/aug; 44-489- Minoomahsh i d evaluation <strong>of</strong> ‘‘goldenproportion’’ in individuals with an <strong>esthetic</strong><strong>smile</strong>; J esthet restor dent 16:185–193,200410-Varun Pratap Singh; Principles <strong>of</strong> SmileAnalysis in <strong>Orthodontics</strong>- A ClinicalOverview; Health Renaissance, January-April 2011; Vol 9 (No.1);35-4011-J. Bennett, R. P. McLaughlin: “OrthodonticManagement <strong>of</strong> the Dentition with thePreadjusted Appliance,” ISBN 1 899066Isis Medical Media 1997.12-Strang , R.H.W. A textbook <strong>of</strong>orthodontia . Philadelphia; Lea andFebiger , 199313-Moore T, Buccal corridors and <strong>smile</strong><strong>esthetic</strong>s. Am J <strong>Orthodontics</strong>Dent<strong>of</strong>acialOrthopedics.2005;127(2):208-213.14-Hulsey CM. An <strong>esthetic</strong> evaluation <strong>of</strong>tooth-lip relationships present in <strong>smile</strong>.Am J Orthod 1970;57:132-44.15-Kurth JR, Kokich VG. Open gingivalembrasures after orthodontic treatment inadults: Prevalence and etiology. Am JOrthod Dent<strong>of</strong>acial Orthop 2001;120:116-2316-David M. Sarver; Principles <strong>of</strong> cosmeticdentistry in orthodontics: Part 1. Shapeand proportionality <strong>of</strong> anterior teeth; Am JOrthod Dent<strong>of</strong>acial Orthop2004;126:749-522