Please click here (1.5MB) - Hong Kong Society of Palliative Medicine
Please click here (1.5MB) - Hong Kong Society of Palliative Medicine
Please click here (1.5MB) - Hong Kong Society of Palliative Medicine

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
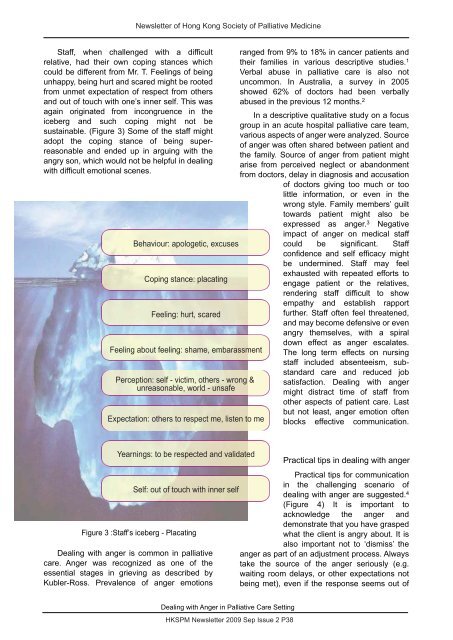
Newsletter <strong>of</strong> <strong>Hong</strong> <strong>Kong</strong> <strong>Society</strong> <strong>of</strong> <strong>Palliative</strong> <strong>Medicine</strong>Staff, when challenged with a difficultrelative, had their own coping stances whichcould be different from Mr. T. Feelings <strong>of</strong> beingunhappy, being hurt and scared might be rootedfrom unmet expectation <strong>of</strong> respect from othersand out <strong>of</strong> touch with one’s inner self. This wasagain originated from incongruence in theiceberg and such coping might not besustainable. (Figure 3) Some <strong>of</strong> the staff mightadopt the coping stance <strong>of</strong> being superreasonableand ended up in arguing with theangry son, which would not be helpful in dealingwith difficult emotional scenes.Behaviour: apologetic, excusesCoping stance: placatingFeeling: hurt, scaredFeeling about feeling: shame, embarassmentPerception: self - victim, others - wrong &unreasonable, world - unsafeExpectation: others to respect me, listen to meranged from 9% to 18% in cancer patients andtheir families in various descriptive studies. 1Verbal abuse in palliative care is also notuncommon. In Australia, a survey in 2005showed 62% <strong>of</strong> doctors had been verballyabused in the previous 12 months. 2In a descriptive qualitative study on a focusgroup in an acute hospital palliative care team,various aspects <strong>of</strong> anger were analyzed. Source<strong>of</strong> anger was <strong>of</strong>ten shared between patient andthe family. Source <strong>of</strong> anger from patient mightarise from perceived neglect or abandonmentfrom doctors, delay in diagnosis and accusation<strong>of</strong> doctors giving too much or toolittle information, or even in thewrong style. Family members’ guilttowards patient might also beexpressed as anger. 3 Negativeimpact <strong>of</strong> anger on medical staffcould be significant. Staffconfidence and self efficacy mightbe undermined. Staff may feelexhausted with repeated efforts toengage patient or the relatives,rendering staff difficult to showempathy and establish rapportfurther. Staff <strong>of</strong>ten feel threatened,and may become defensive or evenangry themselves, with a spiraldown effect as anger escalates.The long term effects on nursingstaff included absenteeism, substandardcare and reduced jobsatisfaction. Dealing with angermight distract time <strong>of</strong> staff fromother aspects <strong>of</strong> patient care. Lastbut not least, anger emotion <strong>of</strong>tenblocks effective communication.Yearnings: to be respected and validatedSelf: out <strong>of</strong> touch with inner selfFigure 3 :Staff’s iceberg - PlacatingDealing with anger is common in palliativecare. Anger was recognized as one <strong>of</strong> theessential stages in grieving as described byKubler-Ross. Prevalence <strong>of</strong> anger emotionsPractical tips in dealing with angerPractical tips for communicationin the challenging scenario <strong>of</strong>dealing with anger are suggested. 4(Figure 4) It is important toacknowledge the anger anddemonstrate that you have graspedwhat the client is angry about. It isalso important not to ‘dismiss’ theanger as part <strong>of</strong> an adjustment process. Alwaystake the source <strong>of</strong> the anger seriously (e.g.waiting room delays, or other expectations notbeing met), even if the response seems out <strong>of</strong>Dealing with Anger in <strong>Palliative</strong> Care SettingHKSPM Newsletter 2009 Sep Issue 2 P38