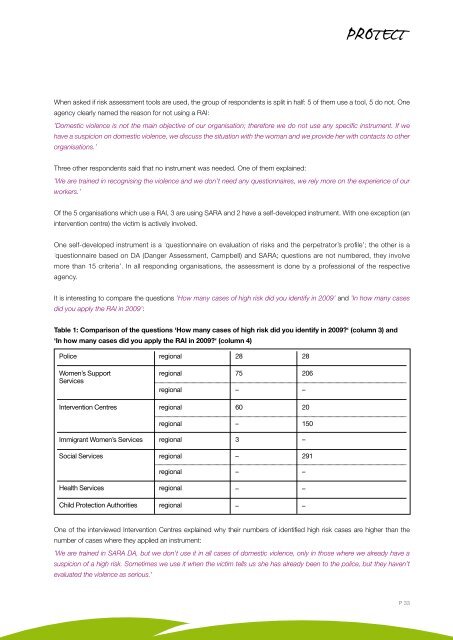
When asked if risk assessment tools are used, the group of respondents is split in half: 5 of them use a tool, 5 do not. Oneagency clearly named the reason for not using a RAI:’Domestic violence is not the main objective of our organisation; therefore we do not use any specific instrument. If wehave a suspicion on domestic violence, we discuss the situation with the woman and we provide her with contacts to otherorganisations.’Three other respondents said that no instrument was needed. One of them explained:’We are trained in recognising the violence and we don’t need any questionnaires, we rely more on the experience of ourworkers.’Of the 5 organisations which use a RAI, 3 are using SARA and 2 have a self-developed instrument. With one exception (anintervention centre) the victim is actively involved.One self-developed instrument is a ’questionnaire on evaluation of risks and the perpetrator’s profile’; the other is a’questionnaire based on DA (Danger Assessment, Campbell) and SARA; questions are not numbered, they involvemore than 15 criteria’. In all responding organisations, the assessment is done by a professional of the respectiveagency.It is interesting to compare the questions ’How many cases of high risk did you identify in 2009’ and ’In how many casesdid you apply the RAI in 2009’:Table 1: Comparison of the questions ‘How many cases of high risk did you identify in 2009?‘ (column 3) and‘In how many cases did you apply the RAI in 2009?‘ (column 4)Police regional 28 28Women’s SupportServicesIntervention Centresregional 75 206regional – –regional 60 20Immigrant Women’s ServicesSocial Servicesregionalregionalregionalregional– 1503 –– 291– –Health Servicesregional––Child Protection Authoritiesregional––One of the interviewed Intervention Centres explained why their numbers of identified high risk cases are higher than thenumber of cases where they applied an instrument:’We are trained in SARA DA, but we don’t use it in all cases of domestic violence, only in those where we already have asuspicion of a high risk. Sometimes we use it when the victim tells us she has already been to the police, but they haven’tevaluated the violence as serious.’P 33
Research ReportsThe blanks in this table signify that most respondents do not count the high risk cases separately, if at all.Looking at the evaluation of the risk assessment tools in use, all participants voiced a positive opinion. But critical commentswere also stated, such as:’The tool (SARA) remains at a surface and doesn’t go deeper. It is good in cases where there is drug or alcohol abuse, butnot in cases of psychological abuse; in those cases we would need a different tool. It consists of 15 questions, some of themask also if the perpetrator received psychiatric treatment at some point. But people with personal disorders often don’t go toa psychiatrist. Also, a victim isn’t able to evaluate the situation well, isn’t able to answer whether she is in danger. We have anegative experience that the police use the tool too strictly, they just fill in the questionnaire with ’yes’ or ’no’, but they do notsee the danger.’Safety planningStandards for protection and safety for high risk victims of intimate partner violence are provided by 8 out of 10 respondents.Among them, 5 have written policies/guidelines. The respondent of the police described the regular standard of protectionand safety of all kinds of victims (not limited to domestic violence). The others stated that these standards are part of thewritten rules of their organisations. A specific difference between victims and high risk victims is not made. The participantsof social services, health services and child protection stated that they do not have written policies/guidelines concerning theprotection of high risk victims.When asked about the measures of protection and safety, seven respondents named safety planning, 5 referred to the multiagencyapproach and 3 indicated other means (multiple answers were possible). One regional social service organisationexplained why they use the multi-agency approach: ’We cooperate with the police; it is a guarantee the victim is not faking/making it up.’There seems to be a misunderstanding concerning the term ’multi-agency approach’. Two respondents used it in the senseof ’multidisciplinary team’: ’We run a multi-agency team at … (but we work for the whole city of ….)’.50% of the participants said that they do not provide regular training for working with high risk victims, specifying:’There is no regular training on high risk violence, but staff participate in domestic violence trainings, there are many seminars,conferences etc. We try to make sure that every employee attends at least one training and provides information to others.’And 9 out of 10 stated that they provide training for newcomers within the organisation. Due to the unspecific question thispart is mostly understood as a general training and not specifically geared to high risk victims. Therefore the answers are notvery valid. Example:’Newcomers are always trained. They participate in an accredited training provided by …, then a basic training in crisis andphone intervention, they are obliged to participate in the trainings. We also organise upgrade trainings for them, we subscribeto professional magazines and buy professional literature.’Two out of 10 organisations review and analyse homicides, attempted homicides and severe cases of violence within theiragency. One does so on a regular basis once a year, the other, whenever a case occurs. The interviewed police unit said thatthis is done on a different (higher) police level.P 34 | PROTECT | Good practice in preventing serious violence, attempted homicides, including crimes in the name of honour, and in protecting high risk victims of gender based violence