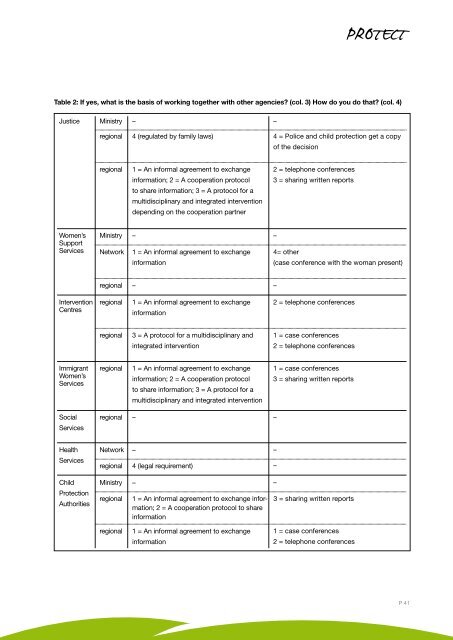
Table 2: If yes, what is the basis of working together with other agencies? (col. 3) How do you do that? (col. 4)JusticeMinistry––regional4 (regulated by family laws)4 = Police and child protection get a copyof the decisionregional1 = An informal agreement to exchangeinformation; 2 = A cooperation protocolto share information; 3 = A protocol for amultidisciplinary and integrated interventiondepending on the cooperation partner2 = telephone conferences3 = sharing written reportsWomen’sSupportServicesMinistryNetwork–1 = An informal agreement to exchangeinformation–4= other(case conference with the woman present)regional––InterventionCentresregional1 = An informal agreement to exchangeinformation2 = telephone conferencesregional3 = A protocol for a multidisciplinary andintegrated intervention1 = case conferences2 = telephone conferencesImmigrantWomen’sServicesregional1 = An informal agreement to exchangeinformation; 2 = A cooperation protocolto share information; 3 = A protocol for amultidisciplinary and integrated intervention1 = case conferences3 = sharing written reportsSocialServicesregional––HealthServicesNetworkregional–4 (legal requirement)––ChildProtectionAuthoritiesMinistryregional–1 = An informal agreement to exchange information;2 = A cooperation protocol to shareinformation–3 = sharing written reportsregional1 = An informal agreement to exchangeinformation1 = case conferences2 = telephone conferencesP 41
Research ReportsThere seem to be some protocols on how to share information and cooperate, but those seem to be regional and not followedin a multi-institutional manner, just bilateral (i.e., between police and one intervention centre). Those protocols do not seem tobe a state-wide strategy to prevent high risk cases, but based on regional/local endeavours of individual agencies.Of the 9 respondents who cooperate with others, 3 stated that they do not need the woman’s consent to share the informationwith others. The respondent of the health service said that they only cooperate with the police, and only if the victim is seriouslyhurt and they assume that a crime has happened. Then they are obliged by law to inform the police – also against the will ofthe victim. All other participants need the women’s consent, either in writing (2) or at least verbal (1) or both (3) depending onthe situation – a verbal agreement may be sufficient for the acute moment, but further on a written consent must be given.Looking at the availability of the data of a high risk case, 9 respondents said that only the case manager has access to thesedata, 2 participants stated that both the case manager and the relevant unit have access.A systematic sharing of information on high risk cases within an organisation was confirmed in 2 NGOs. They review suchcases in their team meetings regularly. One could not give any numbers, the other mentioned 20 cases in 2009.Three participants out of 12 (resp. 15) have written policies/guidelines concerning the cooperation in high risk cases. Therespondent of the regional justice agency again referred to the new enactment describing the cooperation between police,the justice system and victims’ support services. The immigrant women service said that a policy exists, but did not specifydetails. The representative of the health service sector pointed towards ‘written material which gives doctors advice where toturn to if there is a case of domestic violence.‘ With the exception of the above-mentioned enactment, the other answers donot give any clue to high risk cases, unless every domestic violence/forced marriage case is considered a high risk case.All 15 participants denied that the analysis of homicides or attempted homicides is part of their multi-agency work.Summary:Only those who work in direct contact with victims (on the regional level) identify high risk cases. The knowledge about riskassessment instruments seems to be rather limited. Almost half of the respondents who identify high risk victims did notknow any instruments.Mostly, self-developed instruments are in use, but with one exception (child protection authorities) they are not appliedsystematically.According to the mapping results, up to now the ministries have no strategic coordinated plan on protection and safetyfor high risk victims of gender-based intimate partner violence. However, several ministries of Lower Saxony are presentlyworking on a joint effort in form of a protocol on an inter-ministry level.Some protocols to share information and to cooperate on the operational level seem to exist, but those protocols areapparently regional and not multi-institutional (at most bilateral).None of the respondents sees the analysis of homicides and attempted homicides as part of their multi-agency approach,but especially the ministries were rather interested in that aspect.P 42 | PROTECT | Good practice in preventing serious violence, attempted homicides, including crimes in the name of honour, and in protecting high risk victims of gender based violence