PENNCare PPO Benefit Summary - uphs
PENNCare PPO Benefit Summary - uphs
PENNCare PPO Benefit Summary - uphs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
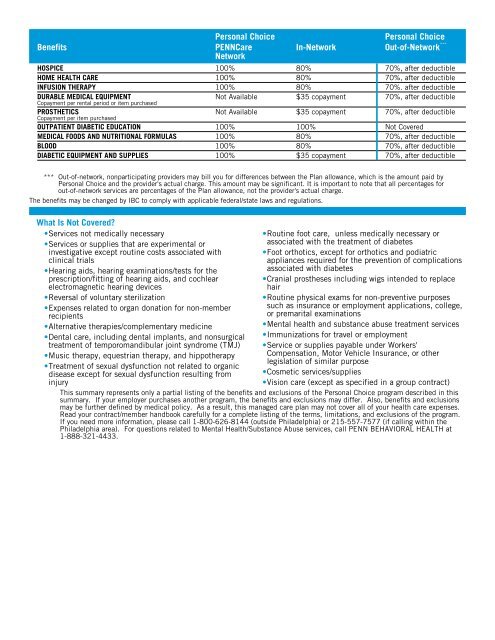
<strong>Benefit</strong>sPersonal Choice<strong>PENNCare</strong>NetworkPersonal ChoiceIn-Network Out-of-Network ***HOSPICE 100% 80% 70%, after deductibleHOME HEALTH CARE 100% 80% 70%, after deductibleINFUSION THERAPY 100% 80% 70%. after deductibleDURABLE MEDICAL EQUIPMENTNot Available $35 copayment 70%, after deductibleCopayment per rental period or item purchasedPROSTHETICSNot Available $35 copayment 70%, after deductibleCopayment per item purchasedOUTPATIENT DIABETIC EDUCATION 100% 100% Not CoveredMEDICAL FOODS AND NUTRITIONAL FORMULAS 100% 80% 70%, after deductibleBLOOD 100% 80% 70%, after deductibleDIABETIC EQUIPMENT AND SUPPLIES 100% $35 copayment 70%, after deductible*** Out-of-network, nonparticipating providers may bill you for differences between the Plan allowance, which is the amount paid byPersonal Choice and the provider's actual charge. This amount may be significant. It is important to note that all percentages forout-of-network services are percentages of the Plan allowance, not the provider's actual charge.The benefits may be changed by IBC to comply with applicable federal/state laws and regulations.What Is Not Covered?•Services not medically necessary•Services or supplies that are experimental orinvestigative except routine costs associated withclinical trials•Hearing aids, hearing examinations/tests for theprescription/fitting of hearing aids, and cochlearelectromagnetic hearing devices•Reversal of voluntary sterilization•Expenses related to organ donation for non-memberrecipients•Alternative therapies/complementary medicine•Dental care, including dental implants, and nonsurgicaltreatment of temporomandibular joint syndrome (TMJ)•Music therapy, equestrian therapy, and hippotherapy•Treatment of sexual dysfunction not related to organicdisease except for sexual dysfunction resulting frominjury•Routine foot care, unless medically necessary orassociated with the treatment of diabetes•Foot orthotics, except for orthotics and podiatricappliances required for the prevention of complicationsassociated with diabetes•Cranial prostheses including wigs intended to replacehair•Routine physical exams for non-preventive purposessuch as insurance or employment applications, college,or premarital examinations•Mental health and substance abuse treatment services•Immunizations for travel or employment•Service or supplies payable under Workers'Compensation, Motor Vehicle Insurance, or otherlegislation of similar purpose•Cosmetic services/supplies•Vision care (except as specified in a group contract)This summary represents only a partial listing of the benefits and exclusions of the Personal Choice program described in thissummary. If your employer purchases another program, the benefits and exclusions may differ. Also, benefits and exclusionsmay be further defined by medical policy. As a result, this managed care plan may not cover all of your health care expenses.Read your contract/member handbook carefully for a complete listing of the terms, limitations, and exclusions of the program.If you need more information, please call 1-800-626-8144 (outside Philadelphia) or 215-557-7577 (if calling within thePhiladelphia area). For questions related to Mental Health/Substance Abuse services, call PENN BEHAVIORAL HEALTH at1-888-321-4433.