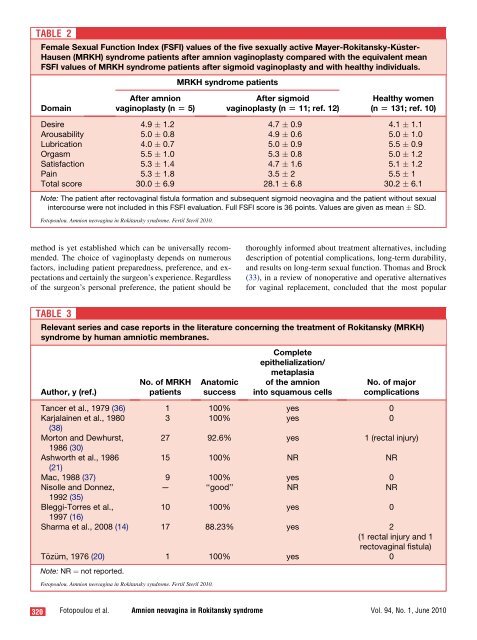
TABLE 2Female Sexual Function Index (FSFI) values <strong>of</strong> the five sexually active Mayer-Rokitansky-K€uster-Hausen (MRKH) syndrome patients after <strong>amnion</strong> <strong>vag<strong>in</strong>oplasty</strong> compared with the equivalent meanFSFI values <strong>of</strong> MRKH syndrome patients after sigmoid <strong>vag<strong>in</strong>oplasty</strong> <strong>and</strong> with healthy <strong>in</strong>dividuals.MRKH syndrome patientsDoma<strong>in</strong>After <strong>amnion</strong><strong>vag<strong>in</strong>oplasty</strong> (n [ 5)After sigmoid<strong>vag<strong>in</strong>oplasty</strong> (n [ 11; ref. 12)Healthy women(n [ 131; ref. 10)Desire 4.9 1.2 4.7 0.9 4.1 1.1Arousability 5.0 0.8 4.9 0.6 5.0 1.0Lubrication 4.0 0.7 5.0 0.9 5.5 0.9Orgasm 5.5 1.0 5.3 0.8 5.0 1.2Satisfaction 5.3 1.4 4.7 1.6 5.1 1.2Pa<strong>in</strong> 5.3 1.8 3.5 2 5.5 1Total score 30.0 6.9 28.1 6.8 30.2 6.1Note: The patient after rectovag<strong>in</strong>al fistula formation <strong>and</strong> subsequent sigmoid neovag<strong>in</strong>a <strong>and</strong> the patient without sexual<strong>in</strong>tercourse were not <strong>in</strong>cluded <strong>in</strong> this FSFI evaluation. Full FSFI score is 36 po<strong>in</strong>ts. Values are given as mean SD.Fotopoulou. Amnion neovag<strong>in</strong>a <strong>in</strong> Rokitansky syndrome. Fertil Steril 2010.method is yet established which can be universally recommended.The choice <strong>of</strong> <strong>vag<strong>in</strong>oplasty</strong> depends on numerousfactors, <strong>in</strong>clud<strong>in</strong>g patient preparedness, preference, <strong>and</strong> expectations<strong>and</strong> certa<strong>in</strong>ly the surgeon’s experience. Regardless<strong>of</strong> the surgeon’s personal preference, the patient should bethoroughly <strong>in</strong>formed about treatment alternatives, <strong>in</strong>clud<strong>in</strong>gdescription <strong>of</strong> potential complications, long-term durability,<strong>and</strong> <strong>results</strong> on long-term sexual function. Thomas <strong>and</strong> Brock(33), <strong>in</strong> a review <strong>of</strong> nonoperative <strong>and</strong> operative alternativesfor vag<strong>in</strong>al replacement, concluded that the most popularTABLE 3Relevant series <strong>and</strong> case reports <strong>in</strong> the literature concern<strong>in</strong>g the treatment <strong>of</strong> Rokitansky (MRKH)syndrome by human amniotic membranes.Author, y (ref.)No. <strong>of</strong> MRKHpatientsAnatomicsuccessCompleteepithelialization/metaplasia<strong>of</strong> the <strong>amnion</strong><strong>in</strong>to squamous cellsNo. <strong>of</strong> majorcomplicationsTancer et al., 1979 (36) 1 100% yes 0Karjala<strong>in</strong>en et al., 1980 3 100% yes 0(38)Morton <strong>and</strong> Dewhurst, 27 92.6% yes 1 (rectal <strong>in</strong>jury)1986 (30)Ashworth et al., 198615 100% NR NR(21)Mac, 1988 (37) 9 100% yes 0Nisolle <strong>and</strong> Donnez,— ‘‘good’’ NR NR1992 (35)Bleggi-Torres et al.,10 100% yes 01997 (16)Sharma et al., 2008 (14) 17 88.23% yes 2(1 rectal <strong>in</strong>jury <strong>and</strong> 1rectovag<strong>in</strong>al fistula)T€oz€um, 1976 (20) 1 100% yes 0Note: NR ¼ not reported.Fotopoulou. Amnion neovag<strong>in</strong>a <strong>in</strong> Rokitansky syndrome. Fertil Steril 2010.320 Fotopoulou et al. Amnion neovag<strong>in</strong>a <strong>in</strong> Rokitansky syndrome Vol. 94, No. 1, June 2010
methods <strong>of</strong> vag<strong>in</strong>al substitution <strong>in</strong>clude passive dilation, <strong>in</strong>laysk<strong>in</strong> grafts, rotational myocutaneous flaps, <strong>and</strong> bowel substitute<strong>vag<strong>in</strong>oplasty</strong>. The American College <strong>of</strong> Obstetricians<strong>and</strong> Gynecologists committee op<strong>in</strong>ion on adolescent healthcare (34) published that the condition can usually be successfullymanaged <strong>in</strong> a conservative way by the use <strong>of</strong> vag<strong>in</strong>al dilatorsas long as the patient is sufficiently motivated. Ifa surgical option is considered, a number <strong>of</strong> approaches areavailable; with the Abbe-McIndoe operation be<strong>in</strong>g the mostcommon.The Abbe-McIndoe technique (29) is <strong>in</strong>deed considered tobe a valid treatment option for <strong>vag<strong>in</strong>oplasty</strong>, but no consensushas been reached on what material should be used for the neovag<strong>in</strong>acanal wall l<strong>in</strong><strong>in</strong>g (27). Various authors have reportedon the use <strong>of</strong> several artificial or biologic materials to coverthe neovag<strong>in</strong>al cavity <strong>and</strong> <strong>in</strong>duce epithelialization. Autologoushuman amniotic membranes (14, 16, 21, 30), homologousamniotic membranes (20), peritoneal layers <strong>of</strong> thepouch <strong>of</strong> Douglas (13), artificial dermis <strong>and</strong> recomb<strong>in</strong>ant basicfibroblast growth factor (7), split-thickness sk<strong>in</strong> graft fromthe buttocks (29), oxidized cellulose (18), acellular hum<strong>and</strong>ermal allograft (26) <strong>and</strong> autologous <strong>in</strong> vitro–cultured vag<strong>in</strong>altissue (27) are some <strong>of</strong> the applied tissues that havebeen named.FIGURE 1Pictures <strong>of</strong> the freeze-dried human amnioticmembranes <strong>and</strong> the vag<strong>in</strong>al mold that is <strong>in</strong>serted for<strong>vag<strong>in</strong>oplasty</strong> <strong>in</strong> Mayer-Rokitansky-K€uster-Hausersyndrome patients. (A) Freeze-dried <strong>amnion</strong> <strong>and</strong>vag<strong>in</strong>al mold. (B) Vag<strong>in</strong>al mold covered with s<strong>of</strong>ratyl.(C) Vag<strong>in</strong>al mold wrapped <strong>in</strong> s<strong>of</strong>ratyl <strong>and</strong> moisturizedamniotic membranes just before <strong>in</strong>sertion <strong>in</strong>to theneovag<strong>in</strong>al cavity.Limited <strong>and</strong> rather older reports are available on the <strong>anatomic</strong><strong>and</strong> functional success <strong>of</strong> <strong>vag<strong>in</strong>oplasty</strong> with human<strong>amnion</strong> (14, 16, 20, 21, 30, 35, 36). The most relevant seriesare presented <strong>in</strong> Table 3. One <strong>of</strong> the first attempts <strong>of</strong> vag<strong>in</strong>alreconstruction from amniotic membranes was <strong>in</strong> 1934 <strong>in</strong> theFrench-language literature, where Br<strong>in</strong>deau used <strong>amnion</strong> toconstruct a neovag<strong>in</strong>a for a patient with mullerian agenesis(39).In the present analysis, we report very good <strong>anatomic</strong> <strong>and</strong>functional <strong>results</strong> <strong>of</strong> <strong>amnion</strong> <strong>vag<strong>in</strong>oplasty</strong> similar to <strong>results</strong>from previous reports. These f<strong>in</strong>d<strong>in</strong>gs confirm those obta<strong>in</strong>edby many previous authors apply<strong>in</strong>g the same method (Table3). In a total <strong>of</strong> 68 reported patients (14, 16, 20, 30, 36,38), all major complications were related to rectal <strong>in</strong>jury (3cases, 4.4%) with otherwise very satisfy<strong>in</strong>g <strong>anatomic</strong> <strong>results</strong>.Of great importance is the fact that follow<strong>in</strong>g diagnos<strong>in</strong>g <strong>of</strong>vag<strong>in</strong>al agenesis <strong>in</strong> adolescent girls, it is important to wait untilthe patient is ready to engage <strong>in</strong> sexual activity before <strong>in</strong>itiat<strong>in</strong>gany k<strong>in</strong>d <strong>of</strong> treatment. For those patients who havea 2–3-cm hymenal fossa, Frank’s method <strong>of</strong> progressive vag<strong>in</strong>aldilation should be always <strong>of</strong>fered (8), but the patientshould be <strong>in</strong>formed that success has proven to be variable<strong>and</strong> unpredictable <strong>and</strong> that the patient needs to be highly motivated<strong>and</strong> will<strong>in</strong>g to cont<strong>in</strong>ue long-term dilations (21, 41).Effective management should, moreover, <strong>in</strong>clude a carefulcomprehensive psychologic preparation <strong>and</strong> support <strong>of</strong> thepatient.We believe that vag<strong>in</strong>al construction from amniotic membranescarries the follow<strong>in</strong>g advantages over other operativereconstructive methods. The human <strong>amnion</strong> appears to haveFotopoulou. Amnion neovag<strong>in</strong>a <strong>in</strong> Rokitansky syndrome. Fertil Steril 2010.Fertility <strong>and</strong> Sterility â 321