Appendix A. Online Risk Assessment Tool - AHRQ National ...
Appendix A. Online Risk Assessment Tool - AHRQ National ...
Appendix A. Online Risk Assessment Tool - AHRQ National ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
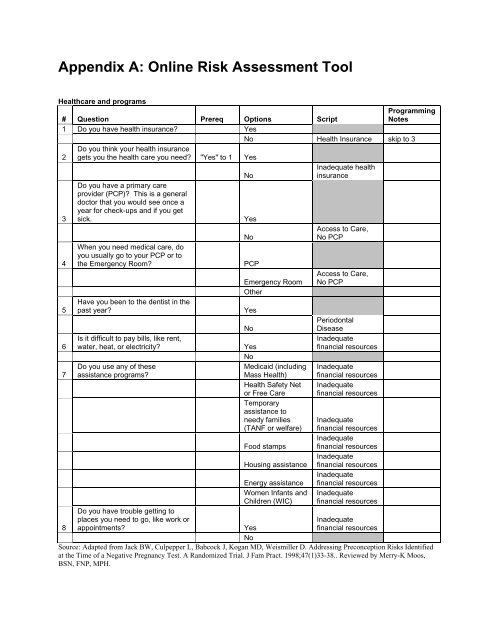
<strong>Appendix</strong> A: <strong>Online</strong> <strong>Risk</strong> <strong>Assessment</strong> <strong>Tool</strong>4 When you need medical care, do you usually go to your PCP or to the Emergency Room?Healthcare and programs# Question Prereq Options ScriptProgrammingNotes1 Do you have health insurance? Yes1 Do you have health insurance? No Health Insurance skip to 32Do you think your health insurancegets you the health care you need? "Yes" to 1 Yes2Do you think your health insurancegets you the health care you need? "Yes" to 1 NoInadequate healthinsurance3Do you have a primary careprovider (PCP)? This is a generaldoctor that you would see once ayear for check-ups and if you getsick.Yes3 Do you have a primary care provider (PCP)? This is a general doctor that you would see once a year for check-ups and if you get sick.NoAccess to Care,No PCPWhen you need medical care, doyou usually go to your PCP or to4 the Emergency Room?PCPAccess to Care,Emergency Room No PCP4 When you need medical care, do you usually go to your PCP or to the Emergency Room?Other556Have you been to the dentist in thepast year?Have you been to the dentist in thepast year?Is it difficult to pay bills, like rent,water, heat, or electricity?6 Is it difficult to pay bills, like rent, water, heat, or electricity?No77777778Do you use any of theseassistance programs?Do you use any of theseassistance programs?Do you use any of theseassistance programs?Do you use any of theseassistance programs?Do you use any of theseassistance programs?Do you use any of theseassistance programs?Do you use any of theseassistance programs?Do you have trouble getting toplaces you need to go, like work orappointments?8 Do you have trouble getting to places you need to go, like work or appointments?NoYesNoYesMedicaid (includingMass Health)Health Safety Netor Free CareTemporaryassistance toneedy families(TANF or welfare)Food stampsHousing assistanceEnergy assistanceWomen Infants andChildren (WIC)YesPeriodontalDiseaseInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesInadequatefinancial resourcesSource: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38.. Reviewed by Merry-K Moos,BSN, FNP, MPH.
health with your partner?3 Are your current partner(s) male, female, or both? "Yes" to 2Relationships# Question Prereq Options Script Programming Notes1Are you dating someone or inany kind of sexual relationship? Yes Continue1 Are you dating someone or in any kind of sexual relationship?No Skip to 4Can you discuss concerns youhave about health with your2 partner? Yes Go to 32 Can you discuss concerns you have aboutNoThe only partner-specificquestions we should askwould be from InfectiousDisease domain. Skip to4 below.Are your current partner(s) male,3 female, or both? "Yes" to 2 Male Ask all partner questions3 Are your current partner(s) male, female, or both? "Yes" to 2FemaleOnly partner questionsfrom Infectious DiseasedomainBoth Ask all partner questionsHave you ever been hit, slapped,4kicked, or physically hurt in anyway?YesPhysical/sexualabuse4 Have you ever been hit, slapped, kicked, or physically hurt in any way?No5Has anyone ever made you dosomething sexual that you didn’twant to do?5 Has anyone ever made you do something sexual that you didn’t want to do?No6Have you ever felt nervous orscared because of the things thatsomeone said to you?6 Have you ever felt nervous or scared because of the things that someone said to you?No7Has anyone ever told you thatyou are a bad person, that youare useless or that you are worthnothing?7 Has anyone ever told you that you are a bad person, that you are useless or that you are worth nothing?No8Are you afraid that someone youknow may hurt you?8 Are you afraid that someone you know may hurt you?No9Are you ever afraid or nervous togo home?9 Are you ever afraid or nervous to go home?NoYesYesYesYesYesPhysical/sexualabuseEmotional(Verbal) abuseEmotional(Verbal) abuseDoes not feelsafeDoes not feelsafe2
2 Do you use birth control on a regular basis? "Yes" to 12a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 2Sexual and reproductive health# Question Prereq Sub-Question Options Script(s)ProgrammingNotes1Have you ever had sex,like vaginal intercourse,oral sex, or anal sex?Yes1 Have you ever had sex, like vaginal intercourse, oral sex, or anal sex?NoRegardless ofanswers to #2and 3, doesnot getQuestions 2,3, 4 inInfectiousDiseasedomain. Inthis section,only askQuestions 3,8, 9 belowDo you use birth control2 on a regular basis? "Yes" to 1 Yes Go to 4aNo No Birth Control Go to 5multiple select(provide all2aIf so, what kind? Checkall the types that you usenow. "Yes" to 2Birth controlpillsBirth Control pillscripts - coulddivide betweeninteractions)2a If so, what kind? Check all the types that you use now. "Yes" to 2Birth controlpatchBirth ControlpatchBirth controlringBirth ControlringBirth controlshotBirth Controlshot (depo)MaleCondom Male CondomsFemaleCondomFemaleCondomsWithdrawal WithdrawalDiaphragm DiaphragmTubes tied Tubal ligationIUD IUDAbstinence AbstinenceImplant ImplantVasectomy VasectomySpermicide SpermicideSpermicidewithCondomSpermicide withCondomMorningafter pillPlan B (morningafter pill)2a If so, what kind? Check all the types that you use now. "Yes" to 22a If so, what kind? Check all the types that you use now. "Yes" to 2Other3Rhythm/naturalfamilyplanningRhythm method(natural familyplanning)General BirthControlRecommendations
Sexual and reproductive health (continued)# Question Prereq Sub-Question Options Script(s)Do you want to have a3 baby in the next year?Yes3 Do you want to have a baby in the next year?No3 Do you want to have a baby in the next year?Don't44 Have you ever been pregnant?No4a4b4c4d4d.14e4f5Have you ever beenpregnant?How many times haveyou been pregnant?This includes allmiscarriages andabortions. "Yes" to 4How many live birthshave you had? "Yes" to 4How many stillbirthshave you had? "Yes" to 4How many miscarriageshave you had? "Yes" to 4Only ifentered 2or more to1dHow manytimes have youhad amiscarriageafter 14 weeksof pregnancy?4knowYesHow many abortions(elective termination ofpregnancy) have youhad? "Yes" to 4How many cesareansections (c-sections)have you had? "Yes" to 4Have you ever had achild who died after he orshe was born? "Yes" to 4 Yes5 Have you ever had a child who died after he or she was born? "Yes" to 4No6 Have you ever had: "Yes" to 46 Have you ever had: "Yes" to 4 An baby weighing more than 9 pounds (or 4000 grams) at birth?No6 Have you ever had: "Yes" to 4 An baby weighing more than 9 pounds (or 4000 grams) at birth?Don't6 Have you ever had:"Yes"to 46 Have you ever had: "Yes" to 4 An baby weighing 5 1/2 pounds or less (or less than 2500 grams) at birth?No6 Have you ever had: "Yes" to 4 An baby weighing 5 1/2 pounds or less (or less than 2500 grams) at birth?Don'topen-endednumberopen-endednumberopen-endednumber Stillbirth If >0open-endednumberopen-endednumberopen-endednumberopen-endednumberMiscarriage (1or 2) ORMiscarriage (3or more)Two secondtrimestermiscarriagesAbortionCesareanSectionInfant or ChildDeathAn babyweighing morethan 9 pounds(or 4000 grams)at birth? Yes HBW infantknow HBW infantAn babyweighing 5 1/2pounds or less(or less than2500 grams) atbirth? Yes LBW infantknow LBW infantProgrammingNotesintro shouldnot stresspregnancy/babyContinue to1a-1fSkip to nextdomainGiveappropriatescript based onnumberenteredGive script ifenter 2 ormore
Sexual and reproductive health (continued)# Question Prereq Sub-Question Options Script(s)A premature orpreterm baby(born at least 3Prior premature6 Have you ever had: "Yes" to 4 weeks early)? Yesbirth6 Have you ever had: "Yes" to 4 A premature or preterm baby (born at least 3 weeks early)?No6 Have you ever had: "Yes" to 4 A premature or preterm baby (born at least 3 weeks early)?Don't6 Have you ever had:"Yes"to 46 Have you ever had: "Yes" to 4 A baby with a birth defect?No6 Have you ever had: "Yes" to 4 A baby with a birth defect?Don't6 Have you ever had:"Yes"to 46 Have you ever had: "Yes" to 4 A baby that had to stay in an intensive care nursery (NICU)?No6 Have you ever had:"Yes"to 4Prior prematureknow birthA baby with abirth defect? Yes Birth defectknow Birth defectA baby that hadto stay in anintensive carenursery (NICU)? Yes NICUVaginalbleeding late inpregnancy?6 Have you ever had: "Yes" to 4 Vaginal bleeding late in pregnancy?No6 Have you ever had:"Yes"to 4A problem withyour uterus(womb)?6 Have you ever had: "Yes" to 4 A problem with your uterus (womb)?No6 Have you ever had: "Yes" to 4 A problem with your uterus (womb)?Don't7YesYesknowHave you ever gottenpregnant less than 3months after the end ofanother pregnancy? "Yes" to 4 Yes7 Have you ever gotten pregnant less than 3 months after the end of another pregnancy? "Yes" to 4No7 Have you ever gotten pregnant less than 3 months after the end of another pregnancy? "Yes" to 4Don't8When you were bornvery early or very small?8 When you were born very early or very small?No8 When you were born very early or very small?Don’t9When your mother wasborn, was she born veryearly or very small?9 When your mother was born, was she born very early or very small?NoknowYesknowYesVaginalbleedingUterineanomaliesUterineanomaliesShort timebetweenpregnanciesShort timebetweenpregnanciesBorn low birthweight orpretermBorn low birthweight orpretermMother born lowbirth weight orpretermProgrammingNotesMother born lowbirth weight orDon't know preterm9 When your mother was born, was she born very early or very small?Source: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1):33-38. References: Norton M. Newevidence on birth spacing: Promising findings for improving newborn, infant, child, and maternal health. International Journal ofGynecology and Obstetrics (2005) 89, S1—S6. Zhu BP. Effect of interpregnancy interval on birth outcomes: Findings from threerecent US studies. International Journal of Gynecology and Obstetrics. 2005. 89:S25—S33. Zhu BP, Rolfs RT, Nangle BE,Horan, JM. Effect of the interval between pregnancies on perinatal outcomes. NEJM. 2005; 340(8):589-594. Reviewed by DeanV. Coonrod, MD; Karla Damus, RN, MSPH, PhD.5
Chronic medical and meds# Question Prereq Options Script(s) Programming Notes1Do you have any chronic healthconditions, like diabetes, asthmaor HIV? Yes Tb high riskPlug in "because youhave been diagnosedwith a chronic healthcondition"1 Do you have any chronic health conditions, like diabetes, asthma or HIV?No2Have you been told by a doctorthat you have any of these healthissues? Check all that apply: Diabetes DiabetesPre-Diabetes2 Have you been told by a doctor that you have any of these health issues? Check all that apply:Pre-Diabetes2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:Lupus2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:GestationalDiabetes(diabetes duringpregnancy)ThyroidDisease(Overactive)ThyroidDisease(Underactive)Phenylketonuria(PKU)Hypertension(high bloodpressure)RheumatoidArthritisGestationalDiabetes(diabetesduringpregnancy)ThyroidDiseaseoveractiveThyroidDiseaseunderactivePKUHypertensionRheumatoidArthritisSLEKidneyChronic RenalProblems DiseaseCardiovascularDisease (heartdisease) Cardiovascular2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:2 Have you been told by a doctor that you have any of these health issues? Check all that apply:Blood Clots ThrombophiliaAsthma AsthmaSeizures(Epilepsy) SeizuresNone of theabove3 Do you have a disability? YesWomen withDiabilities3 Do you have a disability?No4 Have you ever had cancer? Yes Cancer4 Have you ever had cancer?No5Do you take any medicinesprescribed by a doctor? Yes Prescriptions Continue to 3Skip to 45 Do you take any medicines prescribed by a doctor?No6
6 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 56 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 5Chronic medical and meds (continued)# Question Prereq Options Script(s) Programming Notes6Do you take any prescriptions forthe following health issues?Check all that apply: "Yes" to 5 Diabetes PrescriptionsPlug condition intoscript6 Do you take any prescriptions for the following health issues? Check all that apply: "Yes" to 5Seizures(Epilepsy) PrescriptionsPlug condition intoscriptHypertension(high bloodpressure) PrescriptionsPlug condition intoscriptThyroidDisease PrescriptionsPlug condition intoscriptLupus PrescriptionsPlug condition intoscriptRheumatoidArthritisPrescriptionsPlug condition intoscriptAsthma PrescriptionsPlug condition intoscriptKidneyProblems PrescriptionsPlug condition intoscriptCardiovascularDisease (heartdisease) PrescriptionsPlug condition intoscriptBlood Clots PrescriptionsPlug condition intoscriptChronic Pain PrescriptionsPlug condition intoscriptFor anotherhealth issue PrescriptionsPlug condition intoscriptDo you take any "over the7 counter" medications? Yes OTC's7 Do you take any "over the counter" medications?NoHave you ever taken herbs (likechamomile or ginseng), herbalteas, home remedies, or weightloss products for your health?HerbalSupplementsand weightloss products8YesNo8 Have you ever taken herbs (like chamomile or ginseng), herbal teas, home remedies, or weight loss products for your health?Source: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38. Reviewed by Anne L. Dunlop,MD, MPH; Benjamin D. Solomon, MD; Cynthia S. Shellhaas, MD, MPH; Joseph N.Bottalico, DO; Melissa A. McDiarmid, MD,MPH; Mona R. Prasad, DO, MPH; Paula M. Gardiner, MD, MPH; Catherine Ruhl, CNM, MS.7
Family and genetic historyAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health1 Have you or your partner ever had any of the following conditions? Check all that apply:PromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health1 Have you or your partner ever had any of the following conditions? Check all that apply:PromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health1 Have you or your partner ever had any of the following conditions? Check all that apply:PromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health1 Have you or your partner ever had any of the following conditions? Check all that apply:PromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health1 Have you or your partner ever had any of the following conditions? Check all that apply:PromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health1 Have you or your partner ever had any of the following conditions? Check all that apply:Promotion# Question Prereq Options Script(s)Add "or yourpartner" if chose"Male" or "Both"Have you or your partner ever had to Question 3 inany of the following conditions? HealthChromosomal1 Check all that apply:Promotion disorders Personal History1 Have you or your partner ever had any of the following conditions? Check all that apply:Add "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionDeafness Personal HistoryFacial Clefts(Cleft Palate) Personal HistorySickle Celldisease or trait Personal HistoryThalassemia Personal HistoryDevelopmentalDelay/MentalRetardation Personal HistoryBlood Clots Personal HistoryCancer Personal HistoryClotting1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:1 Have you or your partner ever had any of the following conditions? Check all that apply:2Has anyone in your family or yourpartner’s family ever had(including parents, grandparents,siblings, aunts, uncles, cousins)and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:Add "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health HeartPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in Health OtherPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or yourpartner's family"if chose "Male"or "Both" toQuestion 3 inHealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in Health DeafnessPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionThalassemiaAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in Health BloodPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in Health CancerPromotiondisordersNeural TubeDefects (SpinaBifida)Personal HistoryPersonal HistoryDisease Personal HistoryVision loss,inherited fromfamily member Personal HistoryFamily history ofother congenitalmalformations orbirth defectsPersonal HistoryPersonal HistoryDon't knowabout genetichistoryDon’t knowNone of theaboveChromosomaldisorders Family HistoryFamily HistoryFacial Clefts(Cleft Palate) Family HistorySickle CellDisease or trait Family HistoryFamily HistoryDevelopmentalDelay/MentalRetardation Family HistoryClots Family HistoryFamily HistoryProgrammingNotes8
Family and genetic history (continued)# Question Prereq Options Script(s)Add "or yourpartner's family"Has anyone in your family or your if chose "Male"partner’s family ever hador "Both" to(including parents, grandparents, Question 3 insiblings, aunts, uncles, cousins) HealthClotting2 and of the following?:Promotion disorders Family HistoryNeural TubeDefects (ex:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:Add "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionSpina Bifida) Family History2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:2 Has anyone in your family or your partner’s family ever had (including parents, grandparents, siblings, aunts, uncles, cousins) and of the following?:3Add "or your partner's family" if chose "Male" or "Both" to Question 3 in Health HeartPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in Health CysticPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionAdd "or your partner's family" if chose "Male" or "Both" to Question 3 in HealthPromotionDisease Family HistoryVision loss,inherited fromfamily member Family HistorySudden InfantDeath Syndrome(SIDS)Family HistoryEarly infantdeathFamily HistoryMuscularDystrophy Family HistoryFibrosis Family HistoryFamily history ofother congenitalmalformations orbirth defects Family HistoryDon’t knowNone of theaboveDon't knowabout genetichistoryWhat is your blood ancestors’ethnic/racial/geographicbackground? Please check all thatapply: White Ethnicity-Based3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3European3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 33 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3French-Canadian3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3Cajun3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3African3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3Mediterranean3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3Asian3 What is your blood ancestors’ ethnic/racial/geographic background? Please check all that apply: 3Ethnicity-BasedAshkenaziJewishEthnicity-BasedEthnicity-BasedEthnicity-BasedEthnicity-BasedEthnicity-BasedEthnicity-BasedNone of theaboveProgrammingNotesAdapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identified at theTime of a Negative Pregnancy Test. A Randomized Trial. J. Fam Pract. 1998;47(1)33-38. Reviewed by Benjamin D. Solomon,MD; W. Gregory Feero, MD, PhD; Karla Damus, RN, MSPH, PhD.9
1 Have you been diagnosed with any of the following conditions? Check all that apply:1 Have you been diagnosed with any of the following conditions? Check all that apply:1 Have you been diagnosed with any of the following conditions? Check all that apply:of the following conditions? Check all that apply:2 Do you take medications for any of the following conditions? Check all that apply:2 Do you take medications for any of the following conditions? Check all that apply:2 Do you take medications for any of the following conditions? Check all that apply:2 Do you take medications for any of the following conditions? Check all that apply:Psychiatric# Question PrereqSub-Question Options Points Script(s)Have you been diagnosedwith any of the followingconditions? Check all that1 apply: Depression Depression1 Have you been diagnosed with any of the following conditions? Check all that apply:Anxiety AnxietyBipolarBipolarDisorderDisorderSchizophrenia SchizophreniaNone of theaboveDo you take medications forany of the followingconditions? Check all that2 apply: Depression Prescriptions2 Do you take medications for anyAnxiety PrescriptionsBipolarDisorderPrescriptionsSchizophrenia PrescriptionsOther mentalhealthconditionPrescriptionsNone of theaboveHas anyone in your family oryour partner’s family beendiagnosed with any of theFamily Historyfollowing conditions? Checkof psychiatric3 all that apply:Depressioncondition3 Has anyone in your family or your partner’s family been diagnosed with any of the following conditions? Check all that apply:Anxiety3 Has anyone in your family or your partner’s family been diagnosed with any of the following conditions? Check all that apply:3 Has anyone in your family or your partner’s family been diagnosed with any of the following conditions? Check all that apply:Schizophrenia3 Has anyone in your family or your partner’s family been diagnosed with any of the following conditions? Check all that apply:4In the last 2 weeks, how oftenhave you been bothered byany of the followingproblems?Several4 In the last 2 weeks , how often have you been bothered by any of the following problems? Little interest or pleasure in doing things4 In the last 2 weeks , how often have you been bothered by any of the following problems? Little interest or pleasure in doing things4 In the last 2 weeks , how often have you been bothered by any of the following problems? Little interest or pleasure in doing thingsBipolarDisorderNone of theaboveLittle interestor pleasure indoing things Not at all 0days 1More thanhalf the days 2Nearly everyday 3Family Historyof psychiatricconditionFamily Historyof psychiatricconditionFamily Historyof psychiatricconditionDepression=positive fromscreeningtool, but notdiagnosedProgrammingNotesPositive Score>5 when 4-4iare combined10
Psychiatric (continued)# Question Prereq4aIn the last 2 weeks, how oftenhave you been bothered byany of the followingproblems?4a Feeling down, depressed, or hopeless.Several4a4a5Sub-Question Options Points Script(s)Feeling down,depressed, orhopeless. Not at all 0days 1More thanFeeling down, depressed, or hopeless.half the days 2Nearly everyday 3Feeling down, depressed, or hopeless.In the last month, how oftenhave you felt that you wereunable to control theimportant things in your life? Never 0Almost5 In the last month , how often have you felt that you were unable to control the important things in your life?Sometimes5 In the last month , how often have you felt that you were unable to control the important things in your life?Fairly5 In the last month , how often have you felt that you were unable to control the important things in your life?Very5 In the last month , how often have you felt that you were unable to control the important things in your life?6never 12often 3often 4In the last month, how oftenhave you felt confident aboutyour ability to handle yourpersonal problems? Never 4Almost6 In the last month , how often have you felt confident about your ability to handle your personal problems?Sometimes6 In the last month , how often have you felt confident about your ability to handle your personal problems?Fairly6 In the last month , how often have you felt confident about your ability to handle your personal problems?Very6 In the last month , how often have you felt confident about your ability to handle your personal problems?7never 32often 1often 0In the last month, how oftenhave you felt that things weregoing your way? Never 4Almost7 In the last month , how often have you felt that things were going your way?Sometimes7 In the last month , how often have you felt that things were going your way?Fairly7 In the last month , how often have you felt that things were going your way?Very7 In the last month , how often have you felt that things were going your way?8never 32often 1often 0In the last month, how oftenhave you felt difficulties werepiling up so high that youcould not overcome them? Never 0ProgrammingNotesIf patient answers"more than halfthe days or nearlyevery day toeither of the firsttwo, continue torest of screening.Or STOP ifanswers "not atall" or "severaldays" to BOTH.For 5-8, a scoreof 8 or morewould lead to thestress scriptAlmost never 18 In the last month , how often have you felt difficulties were piling up so high that you could not overcome them?Sometimes 28 In the last month , how often have you felt difficulties were piling up so high that you could not overcome them?Fairly often 38 In the last month , how often have you felt difficulties were piling up so high that you could not overcome them?Very often 48 In the last month , how often have you felt difficulties were piling up so high that you could not overcome them?Sources: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38. PHQ-9 Depression Scale:Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001Sep;16(9):606-13. Perceived Stress Scale: Cohen S. Retrieved from: http://www.psy.cmu.edu/~scohen/. Reviewed by ArielaFriedler, MD; Peter S. Bernstein, MD, MPH11
The next questions are about immunizations, like HPV, tetanus, the flu and more. Do you know about any of the1immunizations you have gotten in the past?1a Have you received any of the following vaccines: "Yes" to 1 Measles, Mumps and Rubella (MMR) vaccine (in childhood)1a Have you received any of the following vaccines: "Yes" to 1 Measles, Mumps and Rubella (MMR) vaccine (in childhood)Tdap - tetanus, diptheria and pertusis - vaccine (once when you were 11-12 years and/or another1b Have you received any of the following vaccines: "Yes" to 1after you turned 18)Tdap - tetanus, diptheria and pertusis - vaccine (once when you were 11-12 years and/or another1b Have you received any of the following vaccines: "Yes" to 1after you turned 18)1c Have you received any of the following vaccines: "Yes" to 1 Tetanus booster shot (within the past 10 years)1c Have you received any of the following vaccines: "Yes" to 1 Tetanus booster shot (within the past 10 years)1d Have you received any of the following vaccines: "Yes" to 1 HPV vaccine - 3 doses (ever)1d Have you received any of the following vaccines: "Yes" to 1 HPV vaccine - 3 doses (ever)1e Have you received any of the following vaccines: "Yes" to 1 Varicella vaccine (2 doses), or ever had the chicken pox1e Have you received any of the following vaccines: "Yes" to 1 Varicella vaccine (2 doses), or ever had the chicken pox1f Have you received any of the following vaccines: "Yes" to 1 Influenza (flu) vaccine (this year)1f Have you received any of the following vaccines: "Yes" to 1 Influenza (flu) vaccine (this year)Immunizations# Question Prereq Sub-Question Options Script(s) Programming NotesThe next questions areabout immunizations, likeHPV, tetanus, the flu andmore. Do you knowabout any of theimmunizations you have1 gotten in the past? Yes Continue to 1a-1gGeneralImmunizationsNo1aHave you received any of the following vaccines:"Yes" to 1Measles, Mumps andRubella (MMR)vaccine (in childhood) YesNo MMRDon'tknow MMRTdap - tetanus,diptheria and pertusis- vaccine (once whenyou were 11-12 yearsand/or another after1bHave you received any of the following vaccines: "Yes" to 1you turned 18) YesNo TdapDon'tknow Tdap1cHave you received any of the following vaccines: "Yes" to 1Tetanus booster shot(within the past 10years)YesNo TdDon'tknow TdHPV vaccine - 31dHave you received any of the following vaccines: "Yes" to 1doses (ever)YesNo HPVDon'tknow HPVVaricella vaccine (2doses), or ever had1eHave you received any of the following vaccines: "Yes" to 1the chicken pox YesNo VaricellaDon'tknow Varicella1fHave you received any of the following vaccines: "Yes" to 1Influenza (flu) vaccine(this year)YesIf flu season (October -April?)No InfluenzaDon'tknow InfluenzaHepatitis B vaccine1gHave you received any of the following vaccines: "Yes" to 1(ever)Yes1gHave1gHaveyou received any of the following vaccines: "Yes" to 1 Hepatitis B vaccine (ever)Noyou received any of the following vaccines: "Yes" to 1 Hepatitis B vaccine (ever)Don'tknowHep B atriskHep B atriskif no / don’t know assessfor risk of contractinghepatitis B ( question 2)if no / don’t know assessfor risk of contractinghepatitis B ( question 2)12
Immunizations (continued)# Question Prereq Sub-Question Options Script(s) Programming NotesPlease answer "Yes,""No," or "Don't know" to"No" or"Don't know"to Hep BvaccinequestionHave you ever livedwith someone whoHep B at risk script - haveVPA hold paper with list ofrisks (if more than one is2 the following questions: above has Hepatitis B? Yesselected)2 Please answer "Yes," "No," or "Don't know" to the following questions: "No" or "Don't know" to Hep B vaccine question above Have you ever lived with someone who has Hepatitis B?No2 Please answer "Yes," "No," or "Don't know" to the following questions: "No" or "Don't know" to Hep B vaccine question above Have you ever lived with someone who has Hepatitis B?2aIf "Male" or"Both" toQuestion 3 inHealthPromotion2a If "Male" or "Both" to Question 3 in Health Promotion Does your partner have Hepatitis B?No2a If "Male" or "Both" to Question 3 in Health Promotion Does your partner have Hepatitis B?2b"Yes" to 1 ofHealthPromotionDoes your partnerhave Hepatitis B?Have you had sexwith more than oneperson during thepast 6 months?2b "Yes" to 1 of Health Promotion Have you had sex with more than one person during the past 6 months?No2b "Yes" to 1 of Health Promotion Have you had sex with more than one person during the past 6 months?2c2c Are you being treated with hemodialysis?No2c2eAre you being treatedwith hemodialysis?Are you being treated with hemodialysis?Have you everworked or do you livein an institution for thedevelopmentallydisabled?2e Have you ever worked or do you live in an institution for the developmentally disabled?NoHave you traveled toHaiti, DominicanRepublic, Africa,Southeast Asia, theMiddle East (exceptIsrael), South PacificIslands, West PacificIslands, or theAmazon River Basinin the last year?13Don'tknowYesDon'tknowYesDon'tknowYesDon'tknowYesat risk forSTIat risk forSTIat risk forSTIat risk forSTIHep B atriskHep B atriskHep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)Hep B at risk script - haveVPA hold paper with list ofrisks (if more than one isselected)2gYesHave you traveled to Haiti, Dominican Republic, Africa, Southeast Asia, the Middle East (except No2gIsrael), South Pacific Islands, West Pacific Islands, or the Amazon River Basin in the last year?Source: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38. Reviewed by Dean V. Coonrod,MD, MPH; Richard Long, MD; Shanna N. Cox, MSPH.
Infectious disease# Question Prereq Sub-Question Options Script(s)1 Check all that apply1 Check all that apply1a1a Are you a healthcare worker?No1bHave you received bloodproducts or organs before1992? Yes Hep C (at risk)Have you received bloodproducts or organs before1992? NoAre you a healthcareworker?YesHep C (at risk),Tb high riskAre you a public safetyworker, like a policeofficer or firefighter? Yes Hep B at riskAre you a public safety worker, like a police officer or firefighter?NoDo you work in acorrectional institution,like a jail? Or have youever stayed overnight in ajail?1b Do you work in a correctional institution, like a jail? Or have you ever stayed overnight in a jail?No1c1c1dDo you work in a daycare,nursery school, orkindergarten? Or are youoften in contact withchildren under 6 yearsold?Do you work in a daycare, nursery school, or kindergarten? Or are you often in contact with children under 6 yearsold?Were you born in acountry other than theUnited States?1d Were you born in a country other than the United States?No1e"Yes" to1c1e "Yes" to 1c Were you born in Latin America, Carribean, Africa, Asia, Eastern Europe, or Russia?No1f1f1gYesYesNoYesTb high risk, atrisk for STI,HepC (at risk)CytomegalovirusImmigrant orRefugeeWere you born in LatinAmerica, Carribean,Africa, Asia, EasternEurope, or Russia? Yes Tb high riskHave you traveled toCentral America, SouthAmerica, Africa, Asia,Eastern Europe, theSouth Pacific or theCaribbean in the lastyear? Yes MalariaHave you traveled to Central America, South America, Africa, Asia, Eastern Europe, the South Pacific or the NoCaribbean in the last year?1g Have you been in contact with someone who has tuberculosis (Tb)?No1gHave you been in contactwith someone who hastuberculosis (Tb)? Yes Tb high riskHave you been in contact with someone who has tuberculosis (Tb)?Don'tknowTb high riskProgrammingNotesAlso, if yes toquestion and girlhas not hadhepatitis B vaccinethen use Hep B atriskAlso, if yes toquestion and girlhas not hadhepatitis B vaccinethen use Hep B atriskPlug in "becauseyou have been incontact withsomeone who hastuberculosis"14
Infectious disease (continued)# Question Prereq Sub-Question Options Script(s)Do you have a tattoo orbody piercing that yougot in your home or1hsomeone else's home? Yes Hep C (at risk)1h Do you have a tattoo or body piercing that you got in your home or someone else's home?No2Has a doctor or nurseever told you that youhave any of the following?Select all that apply.2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.Syphilis2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.Gonorrhea2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.HIV2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.2 Has a doctor or nurse ever told you that you have any of the following? Select all that apply.33When you went to seeyour doctor or nurse inthe past, he or she mayhave tested you for asexually transmittedinfection, or STI. Haveyou ever been tested foran STI? This wouldinclude Chlamydia,Syphillis, HIV and others."Yes" toQuestion1 HealthPromotionWhen you went to see your doctor or nurse in the past, he or she may have tested you for a sexually transmittedNoinfection, or STI. Have you ever been tested for an STI? This would include Chlamydia, Syphillis, HIV and others. "Yes" to Question 1 Health PromotionChlamydia ChlamydiaSyphilisHIVGenitalHerpesHepatitisCTuberculosis(TB)None ofthe aboveYesGonorrhea, Atrisk for STIHSVHepC (hasinfection)TB (hasinfection)Not tested foran STI and issexually activeProgrammingNotesPlug in "becauseyou have a tattoo orpiercing that wasdone at home"Also, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptAlso, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptAlso, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptAlso, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptAlso, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptAlso, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptAlso, if yes to anyand girl has not hadhepatitis B vaccinethen use "Hep B atrisk" scriptContinue 3a-3dbelowonly use if notreceiving "at risk forSTI" script. Skip3a-3d15
Infectious disease (continued)"Yes" to 3# Question Prereq Sub-Question Options Script(s)Please check “Yes,” “No”Have you been testedor “Don’t know” to eachfor Chlamydia in the3a test. "Yes" to 3 past year?YesNot tested foran STI and is3a3a3b3b3b3c3c3c4445Please choose either"Yes," "No" or "Don'tknow" for the next set ofquestions."Yes" to 3"Yes" to 3"Yes" to 3"Yes" to 3"Yes" to 3"Yes" to 3"Yes" to 3"Yes" toQuestion1 HealthPromotion5 Please choose either "Yes," "No" or "Don't know" for the next set of questions. "Yes" to Question 1 Health Promotion5 Please choose either "Yes," "No" or "Don't know" for the next set of questions. "Yes" to Question 1 Health Promotion5aHave you been tested for Chlamydia in the past year?Have you been tested for Chlamydia in the past year?Have you been testedfor syphilis ?Have you been tested for syphilis ?Have you been tested for syphilis ?Have you been testedfor HIV ?Have you been tested for HIV ?Have you been tested for HIV ?Have you had your ppdtest in the past 2 years?This is the skin testwhere they insert abubble of fluid under theskin of your forearm.Have you had your ppd test in the past 2 years? This is the skin test where they insert a bubble of fluid underthe skin of your forearm.Have you had your ppd test in the past 2 years? This is the skin test where they insert a bubble of fluid underthe skin of your forearm.NoDon'tknowYesNoDon'tknowYesNoDon'tknowYesNoDon'tknowsexually activeNot tested foran STI and issexually activeNot tested foran STI and issexually activeNot tested foran STI and issexually activeNot tested foran STI and issexually activeNot tested foran STI and issexually activeNot tested foran STI and issexually activeNot tested foran STI and issexually activeHave you ever hadunprotected sex? (Thismeans vaginalintercourse without acondom, oral sexwithout a condom, oranal sex without acondom.) Yes At risk for STIHave you ever had unprotected sex? (This means vaginal intercourse without a condom, oral sex without acondom, or anal sex without a condom.)Have you ever had unprotected sex? (This means vaginal intercourse without a condom, oral sex without acondom, or anal sex without a condom.)5a Have you ever been paid for sex, or had sex for drugs?NoNoDon'tknowAt risk for STIHave you ever beenpaid for sex, or had sexfor drugs? Yes At risk for STIProgrammingNotesonly use if notreceiving "at risk forSTI" scriptonly use if notreceiving "at risk forSTI" scriptonly use if notreceiving "at risk forSTI" scriptonly use if notreceiving "at risk forSTI" scriptadd "in the pastyear" if they answeryes to any of theSTIs in question 3only use if notreceiving "at risk forSTI" scriptonly use if notreceiving "at risk forSTI" scriptonly use if notreceiving "at risk forSTI" scriptonly use if notreceiving "at risk forSTI" scriptPlug in "have hadunprotected sex."Plug in "may havehad unprotectedsex."Plug in "have beenpaid for sex or hadsex for drugs."16
Infectious disease (continued)# Question Prereq Sub-Question Options Script(s) Programming NotesHave any of your sexualpartners beenPlug in "have had asexual partner that5bdiagnosed with a STI? Yes At risk for STI had an STI."5b Have any of your sexual partners been diagnosed with a STI?No5b5c5c Have any of your sexual partners had syphilis or herpes?No5c5d5d5d5e5e5e5f"Male" or"Both" toQuestion3 inHealthPromotionHave any of your sexual partners been diagnosed with a STI?Don'tknow At risk for STIHave any of your sexualpartners had syphilis orherpes? Yes At risk for STIHave any of your sexual partners had syphilis or herpes?Don'tknowAt risk for STIHave any of your malesexual partners had sexwith men? Yes At risk for STI"Male" or "Both" to Question 3 in HealthNoPromotion Have any of your male sexual partners had sex with men?"Male" or "Both" to Question 3 in HealthPromotion"Male" or"Both" toQuestion3 inHealthPromotionHave any of your male sexual partners had sex with men?Don'tknowAt risk for STIHave any of your sexualpartners had HepatitisC? Yes Hep C (at risk)"Male" or "Both" to Question 3 in HealthNoPromotion Have any of your sexual partners had Hepatitis C?"Male" or "Both" to Question 3 in HealthPromotion Have any of your sexual partners had Hepatitis C?5f Have you ever used illicit drugs (street drugs)? This includes marijuana.NoDon'tknowHep C (at risk)Have you ever usedillicit drugs (streetdrugs)? This includesmarijuana. Yes At risk for STISkip to 4iPlug in "may havehad a sexual partnerthat had an STI."Plug in "had a sexualpartner who hadsyphilis or herpes."Plug in "had a sexualpartner who hadsyphilis or herpes."Plug in "have hadmale sexual partnerwho has had sex withmen." Also, if yes toquestion and girl hasnot had hepatitis Bvaccine then use HepB at risk. (PartnerQuestion)Plug in "may havehad male sexualpartner who has hadsex with men."Also, ifyes to question andgirl has not hadhepatitis B vaccinethen use Hep B atrisk. (PartnerQuestion)Plug in "may havehad a sexual partnerwho had hepatitis c."Plug in "have had asexual partner whohad hepatitis c."Plug in "have usedstreet drugs." Also, ifyes to question andgirl has not hadhepatitis B vaccinethen use Hep B atrisk.Source: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38. Reviewed by Dean V. Coonrod,MD, MPH; Mona R. Prasad, DO, MPH; Shanna N. Cox, MSPH.17
Parental exposures# Question Prereq Options Script(s)12During the last 12months, what was theLARGEST number ofalcoholic drinks that youdrank in a single day? open-ended number AlcoholWhich of the followingbest describes yourtobacco use?2 Which of the following best describes your tobacco use?2 Which of the following best describes your tobacco use?2 Which of the following best describes your tobacco use?345How many cigarettes doyou smoke on a normalday?How many times in thepast year have you usedan illegal drug or used aprescription medicationfor non-medical reasons?Have you ever usedintravenous (IV) drugs?5 Have you ever used intravenous (IV) drugs? 1 or more to question 4NoIf chose oneof first threeoptions for 41 or more toquestion 4I smoke, or usetobacco, regularlynowI smoke, or usetobacco, regularlynow, but I've cutdownI smoke, or usetobacco, every oncein awhileI don't smoke or usetobacco at allopen-ended numberopen-ended numberYes6 Do you use cocaine? Yes6 Do you use cocaine?NoTobaccoTobaccoTobaccoIllicitDrugsAt riskfor STI,HepCHep C(at risk)ProgrammingNotes4 or moreleads to scriptAnswer of 1 ormore leads toscriptPlug in"because youuse IV drugs"to both scripts.Plug in"because youuse cocaine."Text for InfoButtonOne drink isequal to: a 12ounce can ofbeer, OR a 5ounce glass ofwine, OR ashot ofliquor/hardalcohol.Tobaccoincludescigarettes,chew, snuff,cigars, etc.Sources: Alcohol Question: Dawson, DA, Pulay, AJ, Grant, BF. A comparison of two single-item screeners for hazardousdrinking and alcohol use disorder. Alcohol Clin Exp Res. Vol 34, No 2, 2010; pp 364-374. DAST-10: Skinner, HA. The DrugAbuse Screening Test. Addictive Behaviors. 1982;7,363-371. Reviewed by R. Louise Floyd, DSN, RN.18
Nutrition and activity# Question Prereq1How many servings doyou eat per day of:1 How many servings do you eat per day of:Vegetables2Sub-Question Options Script(s) Programming NotesFruitsopen-endednumber valueHealthy Eatingopen-endednumber value Healthy EatingDo you eat fish morethan twice a week? Yes Mercury2 Do you eat fish more than twice a week?No3Do you eat any of thefollowing? Check allthat apply:3 Do you eat any of the following? Check all that apply:3 Do you eat any of the following? Check all that apply:3 Do you eat any of the following? Check all that apply:3 Do you eat any of the following? Check all that apply:4at risk if fruits and veggies addup to less than 5. Plug in "donot eat enough fruits andvegetables" to Healthy Eatingscript.at risk if fruits and veggies addup to less than 5. Plug in "donot eat enough fruits andvegetables" to Healthy EatingscriptRaw or veryundercookedmeats or fish Toxoplasmosis If selected, provide scriptUnpasteurizeddairy products orcheese Listerosis If selected, provide scriptSoft cheeses likefeta, bluecheese, brie,goat cheese orqueso fresco Listerosis If selected, provide scriptHot dogs or delimeat Listerosis If selected, provide scriptWalnuts, olive oilor fatty fish(salmon,mackerel, laketrout, sardines,albacore tuna)Omega-3 FattyAcidsDo you tend to snackon junk food (chips,soda, candy, desserts)most days? Yes Healthy Eating4 Do you tend to snack on junk food (chips, soda, candy, desserts) most days?No5Do you think youmight have an eatingdisorder, like anorexiaor bulimia? Yes Eating Disorder5 Do you think you might have an eating disorder, like anorexia or bulimia?No6Select the way(s) youget folic acid:6 Select the way(s) you get folic acid:Folic6 Select the way(s) you get folic acid:None6 Select the way(s) you get folic acid:Don'tMultivitamin with400 mcg folicacidacid pillknowMultivitaminwith folic acid(doesn’t takeone)Multivitaminwith folic acid(doesn’t takeone)Provide script if NOT selectedPlug in "eat a lot of junk food"to Healthy Eating script19
7 Do you take any of the following vitamins or minerals? Check all that apply:7 Do you take any of the following vitamins or minerals? Check all that apply:Nutrition and activity (continued)# Question PrereqSub-Question Options Script(s) Programming Notes7Do you take any of thefollowing vitamins orminerals? Check allthat apply: Calcium CalciumProvide script if they DO NOTselect7 Do you take any of the following vitamins or minerals? Check all that apply:Vitamin D Vitamin DProvide script if they DO NOTselectIron IronProvide script if they DO NOTselectVitamin A Vitamin A Provide script if they DO select7 Do you take any of the following vitamins or minerals? Check all that apply:8None of theaboveCalcium,Vitamin D andIronDo you drinkcaffeinated drinks likecoffee, tea, soda, orenergy drinks? Yes Caffeine8 Do you drink caffeinated drinks like coffee, tea, soda, or energy drinks?No9What is your heightand weight?9 What is your height and weight?9 What is your height and weight?9 What is your height and weight?9 What is your height and weight?2 open-endedvaluesSee BMI chartCalculate BMI [weight/(height ininches x height in inches)] x703= BMI Underweight=
Environmental exposures# Question Prereq Options Script(s)Do you have well water at1 your home?Yes1 Do you have well water at your home?No1 Do you have well water at your home?Don't1a1a Has it been tested? If "Yes" to 1No1a Has it been tested? If "Yes" to 1Don't2knowIf "Yes"Has it been tested? to 1 YesWater Hazard, WellWaterWater Hazard, WellknowWaterHave you been exposed tolead? Yes Lead2 Have you been exposed to lead?No2 Have you been exposed to lead?Don't3know LeadDo you live near a toxicwaste site or ‘superfundsite’? Yes Soil Hazards3 Do you live near a toxic waste site or ‘superfund site’?No4Do you frequently drinkwater from plastic bottles?4 Do you frequently drink water from plastic bottles?No5Do you frequently eatfoods that come from metalcans that have a whiteplastic lining, like cannedsoup or vegetables?5 Do you frequently eat foods that come from metal cans that have a white plastic lining, like canned soup or vegetables?No5 Do you frequently eat foods that come from metal cans that have a white plastic lining, like canned soup or vegetables?Don't6YesYesWater Hazard, PlasticBottlesEnvironmentalHazard, Plastic LiningEnvironmentalknowHazard, Plastic LiningDo you ever clean a cat'slitter box? Yes Toxoplasmosis6 Do you ever clean a cat's litter box?No7Does your job or yourpartner’s job fall into any ofthe following categories?Check all that apply: Lab and clinical healthcare work Workplace ExposuresWorkplace ExposuresWorkplace Exposuresmaking or metal tempering Workplace ExposuresJobs that use: pesticides,herbicides, rodenticides, solvents(oil-based paints), heavy metals(lead), paint stripping agents, leadbasedpaints or non-latex-basedpaints that are solvent based andcontain metals for pigments Workplace Exposuresof the aboveknow7 Does your job or your partner’s job fall into any of the following categories? Check all that apply:Printing7 Does your job or your partner’s job fall into any of the following categories? Check all that apply:Dry-cleaning7 Does your job or your partner’s job fall into any of the following categories? Check all that apply:Jewelry7 Does your job or your partner’s job fall into any of the following categories? Check all that apply:7 Does your job or your partner’s job fall into any of the following categories? Check all that apply:None7 Does your job or your partner’s job fall into any of the following categories? Check all that apply:Don'tProgrammingNotesGo to Question1aSkip to Question2Skip to Question221
8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:Environmental exposures (continued)# Question Prereq Options Script(s)ProgrammingNotes8In your home(s), have youor your partner beenexposed to any of thefollowing? Check all thatapply: Solvents (oil based paints) Household Exposures8 In your home(s), have you or your partner been exposed to any of the following? Check all that apply:Heavy metals (lead) Household ExposuresPaint stripping chemicals (withmethylene chloride)Household ExposuresJewelry making or metal tempering Household ExposuresPesticides Household ExposuresHerbicides Household ExposuresRodenticides Household ExposuresRemoval of old paint or wall paperfrom walls containing lead-basedpaint.Household ExposuresNon-latex-based paints that aresolvent based and contain metalsfor pigments and antifoulant agents Household ExposuresNone of the aboveDon't knowSource: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38. Reviewed by Melissa A.McDiarmid, MD, MPH; Paula M. Gardiner, MD, MPH.Men# QuestionHas your partner been to the1 doctor in the past year?Sub-Question Options Script(s)YesProgrammingNotesPartner has not been to doctor inNolast year1 Has your partner been to the doctor in the past year?Partner has not been to doctor inDon't Know last year1 Has your partner been to the doctor in the past year?Has your partner beencounseled on his reproductivelife plan (plan about birth controland when he wants to have2 children in the future)?YesPartner has not been counseledNoon reproductive life plan2 Has your partner been counseled on his reproductive life plan (plan about birth control and when he wants to have children in the future)?Partner has not been counseledDon't Know on reproductive life plan2 Has your partner been counseled on his reproductive life plan (plan about birth control and when he wants to have children in the future)?Does your partner have aprimary care doctor (PCP),which is a doctor he would see3 for check-ups or if he was sick?YesNo Partner does not have a doctor3 Does your partner have a primary care doctor (PCP), which is a doctor he would see for check-ups or if he was sick?Don't Know Partner does not have a doctor3 Does your partner have a primary care doctor (PCP), which is a doctor he would see for check-ups or if he was sick?Source: Adapted from Jack BW, Culpepper L, Babcock J, Kogan MD, Weismiller D. Addressing Preconception <strong>Risk</strong>s Identifiedat the Time of a Negative Pregnancy Test. A Randomized Trial. J Fam Pract. 1998;47(1)33-38. Reviewed by Keith A. Frey, MD,MBA.22