414.1 –NEW: Continuous Positive Airway Pressure-CPAP
414.1 –NEW: Continuous Positive Airway Pressure-CPAP
414.1 –NEW: Continuous Positive Airway Pressure-CPAP

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
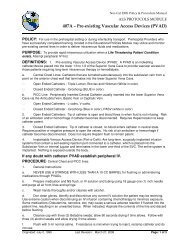
ALS PROTOCOLS MODULE NEW: <strong>Continuous</strong> <strong>Positive</strong> <strong>Airway</strong> <strong>Pressure</strong>-<strong>CPAP</strong> # <strong>414.1</strong>c. Suspected pneumothorax- remove <strong>CPAP</strong>, and evaluate breath sounds, and treat pneuomothoraxif present.3) Hypotension – Systolic < 90, remove <strong>CPAP</strong> and treat hypotension. Administer 250 cc NormalSaline bolus, may repeat once (total 500 cc NS).4) Monitor oxygen supply especially if nebulizers are being run off the same oxygen supply. Caution:<strong>CPAP</strong> devices utilize large amounts of oxygen.Procedure: Make Base Hospital/Receiving Facility contact early to allow respiratory therapy to set upin the Emergency Department and be prepared for the patient to avoid delays in patient transfer. “<strong>CPAP</strong>patient is coming into your facility”1) Place the patient in a seated position with legs dependent (position of comfort)2) Explain the procedure to the patient.3) Instruct the patient to breathe in through their nose slowly and exhale slowly through their mouth.4) Place patient on continuous ECG and oximetry (SpO2)5) Set up <strong>CPAP</strong> circuit and utilize appropriate sized facemask and straps. Utilize the device permanufacturer recommendations.6) Check for air leaks7) Always utilize 100% oxygen for <strong>CPAP</strong>8) Titrate the oxygen flow based upon the patient’s condition and as tolerated9) Start with a liter flow rate of 20 LPM, which will provide approximately 7.5 cm of water pressure10) If the patient condition tolerates it, may advance to a liter flow rate of 25 LPM, approximately 10cm of water pressure11) Monitor and document the patient’s vital signs (BP, HR, RR, and Oxygen saturation (SpO2))every five (5) minutes.12) If the patient’s respiratory status or level of consciousness deteriorates, remove the <strong>CPAP</strong> deviceand reevaluate for advanced airway.13) Continue the <strong>CPAP</strong> until transfer to the hospital ED staff unless the patient is unable to tolerate orclinical condition worsens.14) The narrative must reflect the use of <strong>CPAP</strong>, oxygen flow rate and the resultant PEEP, and theresponse to therapy.Medications:1) If needed, Albuterol will be delivered via in line nebulizer utilizing at least 8 LPM flow(Asthma/COPD etiology).2) May utilize NTG (sublingual tablets only) for chest pain and pulmonary edema patients (spray willbe aerosolized and affect EMS crew). Remember, that <strong>CPAP</strong> effect lost when seal is broken around facemask. If possible, administer nitrates prior to <strong>CPAP</strong>.Failure to Improve: Should a patient not show improvement with <strong>CPAP</strong> (see below list), remove the<strong>CPAP</strong> device and assist ventilations with BVM, use other airway adjuncts, or perform endotrachaelintubation if needed. Remember to always troubleshoot the equipment if patient fails to improve.1) Sustained or increased heart rate2) Sustained or increased respiratory rate3) Sustained elevated BP or hypotension develops4) Sustained low or decreasing oxygen saturation (SpO2)5) Decreased level of consciousness6) Inducement of pneumothoraxOriginated: 03/27/2009 Last Revision: 03/27/09 Page: 2 of 3