PSP End of Life Care Algorithm - GPSC
PSP End of Life Care Algorithm - GPSC
PSP End of Life Care Algorithm - GPSC

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
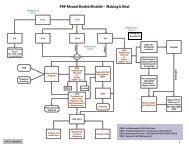
<strong>End</strong> <strong>of</strong> <strong>Life</strong><strong>PSP</strong> ModuleTransition 3Dependency and Symptom IncreaseKey indicator(s) into the Transition: Concern about ability to support client at home given increasing careneedsMaterial provided in package for transition: Notification <strong>of</strong> Expected Death FormMOAEnsure regular contact with family (designated decision maker)Confirm if the client/family is receiving H&CC palliative care services and bring to physicianattention if notIdentify the primary H&CC Nurse, health unit, and pharmacy detailsCoordination <strong>of</strong> care discussions: Schedule palliative care conference meetingIf GP does home visits, may schedule a home visit alone or preferably in conjunction with Home<strong>Care</strong> Nurse to discuss plans for care as illness progressesGPAssess, manage pain and symptoms; provide prognosis, ongoing review/planning. Ensure MOAsput calls through from H&CC Nursing.Coordination <strong>of</strong> care discussion:Either joint visit (0103) or phone call (14016) with H&CC Nursing re options for care as illnessprogresses (PALLIATIVE CARE PLANNING CONFERERNCE).Have self/client/family sign no CPR order form (Counselling Fee 0120 may also be done at HomeVisit 0103Review with client/family how to contact GP after hours and review with the family if death shouldoccur at home (Office Visit 0100 or Home Visit 0103)GP may complete Notification <strong>of</strong> Expected Death if appropriate. (Involves a discussion with H&CC,as such Community Conferencing Fee 14016 applies)Consider others that can extend your medical team to form a full healthcare team. Thesemembers can include social workers and family.Specialist/ConsultantSpecialists: Assess level <strong>of</strong> input needed, demitting point, re-evaluate interventionOther Health <strong>Care</strong> Pr<strong>of</strong>essionals*<strong>Care</strong> Coordinator/Case Coordinator or Home <strong>Care</strong> NurseH&CC - Nursing: Participate in palliative care planning conference with GP, review goals <strong>of</strong> care andupdate the shared care plan (e.g. as to role <strong>of</strong> further investigations)H&CC - Nursing: With GP, help client/family identify and select options for care, depending on thecommunity (may be in conjunction with the Specialist Hospice Palliative <strong>Care</strong> TeamH&CC - Nursing: Prepare client/family for home death and provide intensive home care/supportand specifically home deathH&CC - Nursing: Assess need for further equipment as illness progresses & function reduced--e.g.hospital bed; also need for increased respite/support from home support74_EOL_<strong>PSP</strong>_Transition_3_V2.0 1 <strong>of</strong> 2