candidate handbook - International Nurses Society on Addictions
candidate handbook - International Nurses Society on Addictions
candidate handbook - International Nurses Society on Addictions

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
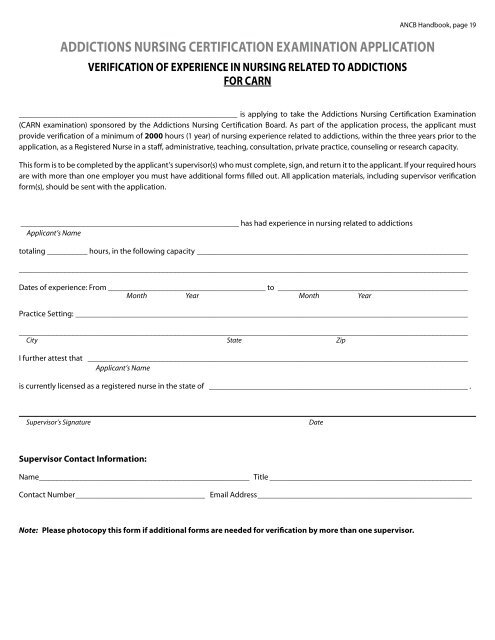
ADDICTIONS NURSING CERTIFICATION EXAMINATION APPLICATIONVERIFICATION OF EXPERIENCE IN NURSING RELATED TO ADDICTIONSFOR CARNANCB Handbook, page 19______________________________________________________ is applying to take the Addicti<strong>on</strong>s Nursing Certificati<strong>on</strong> Examinati<strong>on</strong>(CARN examinati<strong>on</strong>) sp<strong>on</strong>sored by the Addicti<strong>on</strong>s Nursing Certificati<strong>on</strong> Board. As part of the applicati<strong>on</strong> process, the applicant mustprovide verificati<strong>on</strong> of a minimum of 2000 hours (1 year) of nursing experience related to addicti<strong>on</strong>s, within the three years prior to theapplicati<strong>on</strong>, as a Registered Nurse in a staff, administrative, teaching, c<strong>on</strong>sultati<strong>on</strong>, private practice, counseling or research capacity.This form is to be completed by the applicant’s supervisor(s) who must complete, sign, and return it to the applicant. If your required hoursare with more than <strong>on</strong>e employer you must have additi<strong>on</strong>al forms filled out. All applicati<strong>on</strong> materials, including supervisor verificati<strong>on</strong>form(s), should be sent with the applicati<strong>on</strong>.______________________________________________________ has had experience in nursing related to addicti<strong>on</strong>sApplicant’s Nametotaling __________ hours, in the following capacity ___________________________________________________________________________________________________________________________________________________________________________________Dates of experience: From________________________________________ to________________________________________________M<strong>on</strong>th Year M<strong>on</strong>th YearPractice Setting: _________________________________________________________________________________________________________________________________________________________________________________________________________________City State ZipI further attest that _______________________________________________________________________________________________Applicant’s Nameis currently licensed as a registered nurse in the state of _________________________________________________________________ .Supervisor’s SignatureDateSupervisor C<strong>on</strong>tact Informati<strong>on</strong>:Name_____________________________________________________ Title___________________________________________________C<strong>on</strong>tact Number_________________________________ Email Address______________________________________________________Note: Please photocopy this form if additi<strong>on</strong>al forms are needed for verificati<strong>on</strong> by more than <strong>on</strong>e supervisor.