Montana Medicaid - Fee Schedule Speech Therapy Definitions:
Montana Medicaid - Fee Schedule Speech Therapy Definitions:
Montana Medicaid - Fee Schedule Speech Therapy Definitions:

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Montana</strong> <strong>Medicaid</strong> - <strong>Fee</strong> <strong>Schedule</strong><strong>Speech</strong> <strong>Therapy</strong><strong>Definitions</strong>:July 1, 2005Modifier – When a modifier is present, this indicates system may have different reimbursement or code edits for that procedure code/modifier combination.For example:26 = professional componentTC = technical componentDescription – Procedure code short description. You must refer to the appropriate official CPT-4, HCPCS or CDT-5 coding manual for complete definitionsin order to assure correct coding.Effective – This is the first date of service for which the listed fee is applicable. <strong>Fee</strong>s for drugs, radiopharmaceuticals, blood products, immune globins, vaccines,and toxoids are reviewed and updated quarterly -- effective dates that are greater than three months old indicate that there has been no fee change since that date.Method – Source of fee determination<strong>Fee</strong> Sched: <strong>Medicaid</strong> fee; not determined using RBRVS payment scheduleMedicare: Medicare-prevailing fee.By Report (BR): Equals 43% of billed chargesAnes Value: Number of anesthesia base value units. This is added to the 15 min. time increment units and multiplied by the anesthesia conversion factor of $26.07.RBRVS: Based on Medicare Relative Value Units (RVU’s) x <strong>Montana</strong> <strong>Medicaid</strong> conversion factor x policy adjuster. Conversion factor for fiscal year 2006 is $32.59.*If a valid, current code is not present, that code may be a non-covered service<strong>Fee</strong>sThe facility rate is paid to physicians/practitioners providing services in a hospital, emergency room, or ambulatory surgery center site of service. All other sitesof service receive the office rate. Procedures not normally done in the office are shown with the same facility rate, while those done in both locations havedifferent rates. Bundled services, which are covered but paid as part of a related service, are shown with an RBRVS method and a fee of $0.00.Policy adjustments are applied to certain codes to increase or decrease reimbursement for the service.Global Days – Global surgery indicator. Global surgery periods are pre- and post-operative time frames assigned to surgical procedures.000: Same day as procedure010: Same day and ten days following procedure090: One day prior to and ninety days following procedureMMM: In maternity cases, the global period is per the CPT-4 code descriptionZZZ: Add-on code, global period does not apply. An add-on code must be billed with its associated primary codeSpace: Global concept does not apply to this codePA – Prior AuthorizationIndicatorsY: Prior authorization is required Mult - Multiple surgery guidelines do applySpace - this indicator does not apply to this codeBilat - Bilateral. The procedure can be done bilaterallyAssist - Assistant. An assistant is allowed for this procedureCo-Surg - Co-Surgery. A co-surgeon is allowed for this procedureTeam - A team of surgeons is allowed for this procedureRelated - The procedure code listed is separately billableY - indicator is applicable to this codeSpace - this indicator does not apply to this codePolicy Adjust - M = Maternity, P = Mental Health, D = Profess. DifferentialCPT codes, descriptions and other data only are copyright 1999 American Medical Association for such other date ofpublication of CPT). All Rights Reserved. Applicable FARS/DFARS Apply.Please see first page for a complete descriptionof information contained in the fee schedules.1<strong>Fee</strong>s as of July 2005
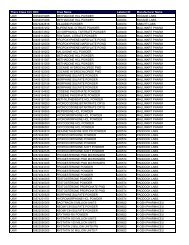
<strong>Montana</strong> <strong>Medicaid</strong> - <strong>Fee</strong> <strong>Schedule</strong><strong>Speech</strong> <strong>Therapy</strong><strong>Fee</strong>s GlobalIndicatorsPolicyProc Mod Description Effective Method Office Facility Days PA Mult Bilat Assist CoSurg Team Adjust92506 SPEECH/HEARING EVALUATION 7/1/2005 RBRVS $84.06 $33.21 D92507 SPEECH/HEARING THERAPY 7/1/2005 RBRVS $40.29 $19.86 D92508 SPEECH/HEARING THERAPY 7/1/2005 RBRVS $19.09 $10.03 D92526 ORAL FUNCTION THERAPY 7/1/2005 RBRVS $53.37 $19.97 D92597 ORAL SPEECH DEVICE EVAL 7/1/2005 RBRVS $63.17 $34.38 D92605 EVAL FOR NONSPEECH DEVICE RX 7/1/2005 RBRVS $0.00 $0.00 D92606 NON-SPEECH DEVICE SERVICE 7/1/2005 RBRVS $0.00 $0.00 D92607 EX FOR SPEECH DEVICE RX 1HR 7/1/2005 RBRVS $72.70 $72.70 D92608 EX FOR SPEECH DEVICE RX ADDL 7/1/2005 RBRVS $13.97 $13.97 D92609 USE OF SPEECH DEVICE SERVICE 7/1/2005 RBRVS $37.89 $37.89 D92610 EVALUATE SWALLOWING FUNCTION 7/1/2005 RBRVS $81.54 $81.54 D92611 MOTION FLUOROSCOPY/SWALLOW 7/1/2005 RBRVS $81.54 $81.54 D96105 ASSESSMENT OF APHASIA 7/1/2005 RBRVS $45.23 $45.23 D97530 THERAPEUTIC ACTIVITIES 7/1/2005 RBRVS $19.78 $19.78 D97532 COGNITIVE SKILLS DEVELOPMENT 7/1/2005 RBRVS $16.75 $16.75 D97533 SENSORY INTEGRATION 7/1/2005 RBRVS $17.67 $17.67 D97535 SELF CARE MNGMENT TRAINING 7/1/2005 RBRVS $20.04 $20.04 D99311 NURSING FAC CARE, SUBSEQ 7/1/2005 RBRVS $25.19 $25.1999312 NURSING FAC CARE, SUBSEQ 7/1/2005 RBRVS $41.74 $41.74Please see first page for a complete descriptionof information contained in the fee schedules.2<strong>Fee</strong>s as of July 2005