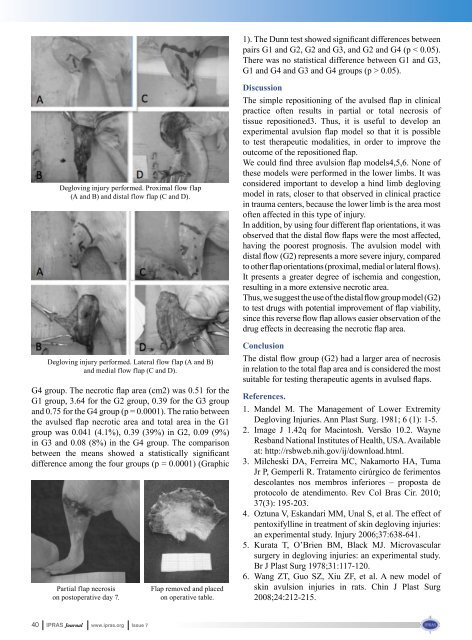
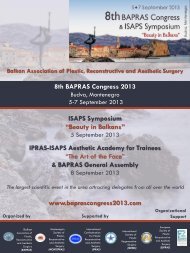
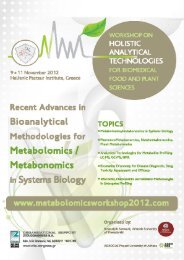
1). The Dunn test showed significant differences betweenpairs G1 and G2, G2 and G3, and G2 and G4 (p < 0.05).There was no statistical difference between G1 and G3,G1 and G4 and G3 and G4 groups (p > 0.05).Degloving injury performed. Proximal flow flap(A and B) and distal flow flap (C and D).Degloving injury performed. Lateral flow flap (A and B)and medial flow flap (C and D).G4 group. The necrotic flap area (cm2) was 0.51 for theG1 group, 3.64 for the G2 group, 0.39 for the G3 groupand 0.75 for the G4 group (p = 0.0001). The ratio betweenthe avulsed flap necrotic area and total area in the G1group was 0.041 (4.1%), 0.39 (39%) in G2, 0.09 (9%)in G3 and 0.08 (8%) in the G4 group. The comparisonbetween the means showed a statistically significantdifference among the four groups (p = 0.0001) (GraphicPartial flap necrosison postoperative day 7.Flap removed and placedon operative table.DiscussionThe simple repositioning of the avulsed flap in clinicalpractice often results in partial or total necrosis oftissue repositioned3. Thus, it is useful to develop anexperimental avulsion flap model so that it is possibleto test therapeutic modalities, in order to improve theoutcome of the repositioned flap.We could find three avulsion flap models4,5,6. None ofthese models were performed in the lower limbs. It wasconsidered important to develop a hind limb deglovingmodel in rats, closer to that observed in clinical practicein trauma centers, because the lower limb is the area mostoften affected in this type of injury.In addition, by using four different flap orientations, it wasobserved that the distal flow flaps were the most affected,having the poorest prognosis. The avulsion model withdistal flow (G2) represents a more severe injury, comparedto other flap orientations (proximal, medial or lateral flows).It presents a greater degree of ischemia and congestion,resulting in a more extensive necrotic area.Thus, we suggest the use of the distal flowgroupmodel(G2)to test drugs with potential improvement of flap viability,since this reverse flow flap allows easier observation of thedrug effects in decreasing the necrotic flap area.ConclusionThe distal flow group (G2) had a larger area of necrosisin relation to the total flap area and is considered the mostsuitable for testing therapeutic agents in avulsed flaps.References.1. Mandel M. The Management of Lower ExtremityDegloving Injuries. Ann Plast Surg. 1981; 6 (1): 1-5.2. Image J 1.42q for Macintosh. Versão 10.2. WayneResband National Institutes of Health, USA. Availableat: http://rsbweb.nih.gov/ij/download.html.3. Milcheski DA, Ferreira MC, Nakamorto HA, TumaJr P, Gemperli R. Tratamento cirúrgico de ferimentosdescolantes nos membros inferiores – proposta deprotocolo de atendimento. Rev Col Bras Cir. 2010;37(3): 195-203.4. Oztuna V, Eskandari MM, Unal S, et al. The effect ofpentoxifylline in treatment of skin degloving injuries:an experimental study. Injury 2006;37:638-641.5. Kurata T, O’Brien BM, Black MJ. Microvascularsurgery in degloving injuries: an experimental study.Br J Plast Surg 1978;31:117-120.6. Wang ZT, Guo SZ, Xiu ZF, et al. A new model ofskin avulsion injuries in rats. Chin J Plast Surg2008;24:212-215.40 <strong>IPRAS</strong> Journal www.ipras.org Issue 7
Syndactyly Correction by “Duoderm-plasty”:An Original Model for Mastering Plastic SurgeryG.V. Yaghjyan, D.O. AbrahamyanPlastic Reconstructive Surgery and Microsurgery Centre, University Hospital № 1.58 Abovyan street, Yerevan, 375025, Republic of Armeniae-mail: plastam@yahoo.comSummaryА novel technique is presented for mastering skills inPlastic Surgery, using only improvised means, particularlythe self-adhesive Duoderm ® CGF ® , which is very similarto the human skin. An example of its application forsyndactyly correction by trilobed flap is shown. Theso-called Duoderm-plasty is an easy and cost-effectivemethod, which allows mastering and perfection ofdifferent Plastic Surgery ‘tricks’, planning a scheduledsurgery and can also serve as a measure for such skills ofthe medical students and residents.KeywordsResidency training; Surgery planning; Z-plasty;SyndactylyIntroductionTraining in the specialty of Plastic Surgery deals with theresection, repair, replacement and reconstruction of defectsof form and function of the integument and its underlyinganatomic structures. It is a long-lasting and laboriousprocess, requiring not merely an excellent, advancedknowledge of medical science, but also a well-developedspatial reasoning and ‘sleight of hand’. The latter can beimproved using different contemporary technologies andequipment offered by many companies.Prior to the 1950’s, the operating room (OR) representedthe only place to visualize surgery outside the classroom.The introduction of film allowed residents to build andintegrate verbal and pictorial representations of disease.Movies became particularly useful in surgical learning tohelp describe anatomic relationships and procedures. Inthe 1980’s computers became an additional tool, with thepotential to model the complexity of real tissues and togain insight into surgical outcomes through simulation. 1It is known that learners retain 10 to 15% of what is read,10-20% of what they hear, and 20-30% of what they see,but when audiovisual materials are integrated, knowledgeretention increases to 40-50%. 2Therefore, simple inanimate models have been developedfor practice of basic surgical skills. Synthetic skinsuturing models and computer simulations of surgery areemerging as a prime education tool at several surgicalskills centres in the West. 5,6Despite all these advances, the system of surgical skillsteaching in Armenia, as well as in many other developingcountries still remains on the 1980’s level because theabovementioned training systems are too expensive.Maintenance of well-equipped dissecting rooms andbiomedical laboratories is impossible in the presenteconomic status. Residents can hone their skills onlyat the OR, which is not so simple, because each expertsurgeons seek to achieve the best results and he/she willrarely agree to ‘rely’ on a novice’s skills. On the otherhand, patients or patients’ relatives always want to beoperated by the best, famous expert surgeons. Anotherproblem is that trainees often ‘wait’ for a specific case fora long time: there are many residents and trainees, morethan the specific cases.All this forced the authors to propose a model, whichwould facilitate and improve the skill acquisition process,at least to some extent, in one of the basic sections ofPlastic Surgery – integument (cutaneous) surgery.Model descriptionThe proposed model is based on the use of self-adhesivehydrocolloid dressings (Duoderm ® CGF ® ) as human-skinsubstitutes.That is why we called this method ‘Duodermplasty’.The unique elastic properties of Duoderm ® CGF ®Issue 7 www.ipras.org <strong>IPRAS</strong> Journal 41
- Page 1: ISSN: 2241-1275
- Page 4 and 5: A I M S A N D S C O P E• To promo
- Page 7 and 8: within the range of statistically e
- Page 9 and 10: G E N E R A L S E C R E T A R Y ’
- Page 11 and 12: Issue 7 www.ipras.org IPRAS Journal
- Page 13 and 14: After Madrid came Beijing, China, f
- Page 15 and 16: From the left: Mr Alexey Kovalsky,
- Page 17 and 18: Mr. Zacharias Kaplanidis (IPRAS Exe
- Page 19 and 20: P I O N E E R SAn interview with Dr
- Page 21 and 22: of excellence is that of evidence-b
- Page 23 and 24: R I S I N G S T A RAn interview wit
- Page 25 and 26: Issue 7 www.ipras.org IPRAS Journal
- Page 27 and 28: Women from the mountains in Afghani
- Page 30 and 31: They must be confident. Security is
- Page 32 and 33: IPRAS (Asia-Pacific Section) organi
- Page 34 and 35: EntertainmentThe organizers were pa
- Page 36 and 37: Plastic Surgery Mission in Togo,Cla
- Page 38 and 39: S U R V E Y SHonoured with the awar
- Page 42 and 43: Duoderm ® CGF ® and Hand modelare
- Page 44 and 45: where the trilobed flap 6 is used.
- Page 46 and 47: 46 IPRAS Journal www.ipras.org Issu
- Page 48: Plastic Surgery Hyperguide:An Inter
- Page 53 and 54: coming back to the scene has everyt
- Page 58 and 59: 23rd Annual EURAPS Meeting,Munich,
- Page 60 and 61: Surgeons conducted meetings in the
- Page 62 and 63: Panamanian Association of Plastic,
- Page 64 and 65: It was, however, not until shortly
- Page 66 and 67: in 1941, gaining a Masters Degree i
- Page 68 and 69: lack of funding and facilities for
- Page 70 and 71: Despite these hurdles, reconstructi
- Page 72 and 73: Patna, Lucknow, Bombay, Pune, Delhi
- Page 74 and 75: TPCDHistory and present situationof
- Page 76 and 77: andom choice of cases, watched by t
- Page 78 and 79: stimulated his interested in maxill
- Page 80 and 81: BAPRAS and the Developing WorldBrit
- Page 82 and 83: 82 IPRAS Journal www.ipras.org Issu
- Page 84 and 85: World Health OrganizationDear colle
- Page 86 and 87: 86 IPRAS Journal www.ipras.org Issu
- Page 88 and 89: 88 IPRAS Journal www.ipras.org Issu
- Page 102 and 103:
102 IPRAS Journal www.ipras.org Iss
- Page 104:
104 IPRAS Journal www.ipras.org Iss
- Page 109 and 110:
For the FIRST time…The 1st IPRASI
- Page 114 and 115:
NATIONAL & CO-OPTED SOCIETIES’ FU
- Page 116 and 117:
I P R A S W E B S I T EJOIN YOUR CO
- Page 118 and 119:
I P R A S P A S T G E N E R A L S E
- Page 120:
7th Issue December 2011IPRAS Journa