Supportive supervision checklist on IMCI - basics
Supportive supervision checklist on IMCI - basics
Supportive supervision checklist on IMCI - basics

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
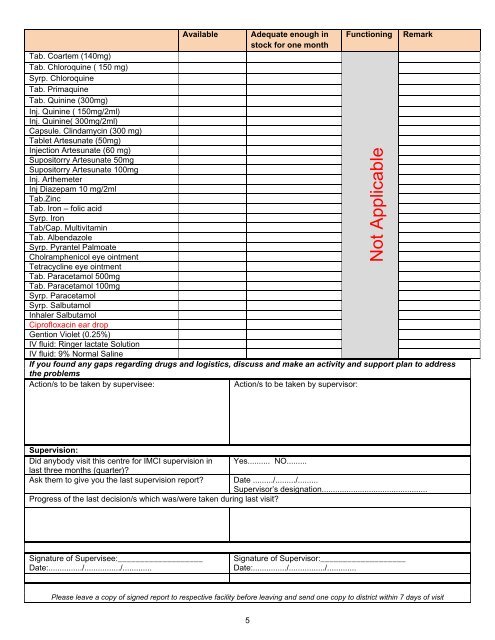
Available Adequate enough in Functi<strong>on</strong>ing Remarkstock for <strong>on</strong>e m<strong>on</strong>thTab. Coartem (140mg)Tab. Chloroquine ( 150 mg)Syrp. ChloroquineTab. PrimaquineTab. Quinine (300mg)Inj. Quinine ( 150mg/2ml)Inj. Quinine( 300mg/2ml)Capsule. Clindamycin (300 mg)Tablet Artesunate (50mg)Injecti<strong>on</strong> Artesunate (60 mg)Supositorry Artesunate 50mgSupositorry Artesunate 100mgInj. ArthemeterInj Diazepam 10 mg/2mlTab.ZincTab. Ir<strong>on</strong> – folic acidSyrp. Ir<strong>on</strong>Tab/Cap. MultivitaminTab. AlbendazoleSyrp. Pyrantel PalmoateCholramphenicol eye ointmentTetracycline eye ointmentTab. Paracetamol 500mgTab. Paracetamol 100mgSyrp. ParacetamolSyrp. SalbutamolInhaler SalbutamolCiprofloxacin ear dropGenti<strong>on</strong> Violet (0.25%)IV fluid: Ringer lactate Soluti<strong>on</strong>IV fluid: 9% Normal SalineIf you found any gaps regarding drugs and logistics, discuss and make an activity and support plan to addressthe problemsActi<strong>on</strong>/s to be taken by supervisee:Acti<strong>on</strong>/s to be taken by supervisor:Not ApplicableSupervisi<strong>on</strong>:Did anybody visit this centre for <strong>IMCI</strong> <str<strong>on</strong>g>supervisi<strong>on</strong></str<strong>on</strong>g> in Yes.......... NO.........last three m<strong>on</strong>ths (quarter)?Ask them to give you the last <str<strong>on</strong>g>supervisi<strong>on</strong></str<strong>on</strong>g> report? Date ........./........./.........Supervisor’s designati<strong>on</strong>...............................................Progress of the last decisi<strong>on</strong>/s which was/were taken during last visit?Signature of Supervisee:___________________Date:.............../................/.............Signature of Supervisor:___________________Date:.............../................/.............Please leave a copy of signed report to respective facility before leaving and send <strong>on</strong>e copy to district within 7 days of visit5