Menactra Vaccine Consent form - Grey Bruce Health Unit
Menactra Vaccine Consent form - Grey Bruce Health Unit
Menactra Vaccine Consent form - Grey Bruce Health Unit
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
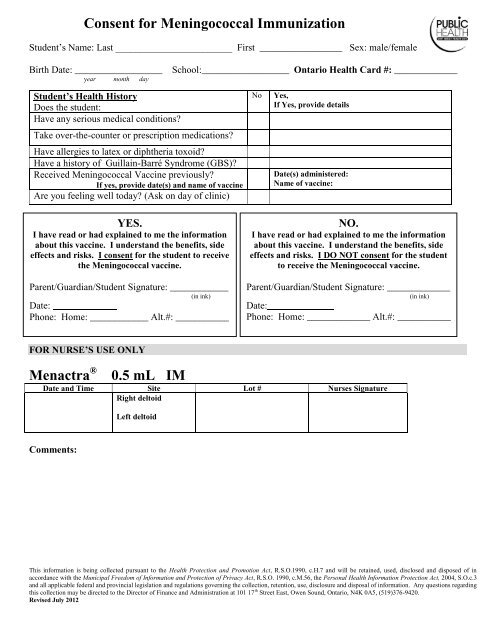
<strong>Consent</strong> for Meningococcal ImmunizationStudent’s Name: Last ________________________ First _________________ Sex: male/femaleBirth Date: __________________year month daySchool:__________________ Ontario <strong>Health</strong> Card #: _____________Student’s <strong>Health</strong> HistoryDoes the student:Have any serious medical conditions?Take over-the-counter or prescription medications?Have allergies to latex or diphtheria toxoid?Have a history of Guillain-Barré Syndrome (GBS)?Received Meningococcal <strong>Vaccine</strong> previously?If yes, provide date(s) and name of vaccineAre you feeling well today? (Ask on day of clinic)NoYes,If Yes, provide detailsDate(s) administered:Name of vaccine:YES.I have read or had explained to me the in<strong>form</strong>ationabout this vaccine. I understand the benefits, sideeffects and risks. I consent for the student to receivethe Meningococcal vaccine.Parent/Guardian/Student Signature: ____________(in ink)Date:Phone: Home: ____________ Alt.#: ___________NO.I have read or had explained to me the in<strong>form</strong>ationabout this vaccine. I understand the benefits, sideeffects and risks. I DO NOT consent for the studentto receive the Meningococcal vaccine.Parent/Guardian/Student Signature: _____________(in ink)Date:Phone: Home: _____________ Alt.#: ___________FOR NURSE’S USE ONLY<strong>Menactra</strong> ®0.5 mL IMDate and Time Site Lot # Nurses SignatureRight deltoidLeft deltoidComments:This in<strong>form</strong>ation is being collected pursuant to the <strong>Health</strong> Protection and Promotion Act, R.S.O.1990, c.H.7 and will be retained, used, disclosed and disposed of inaccordance with the Municipal Freedom of In<strong>form</strong>ation and Protection of Privacy Act, R.S.O. 1990, c.M.56, the Personal <strong>Health</strong> In<strong>form</strong>ation Protection Act, 2004, S.O.c.3and all applicable federal and provincial legislation and regulations governing the collection, retention, use, disclosure and disposal of in<strong>form</strong>ation. Any questions regardingthis collection may be directed to the Director of Finance and Administration at 101 17 th Street East, Owen Sound, Ontario, N4K 0A5, (519)376-9420.Revised July 2012