Healthcare System in Saudi Arabia - Journal of Alternative ...
Healthcare System in Saudi Arabia - Journal of Alternative ...
Healthcare System in Saudi Arabia - Journal of Alternative ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Journal</strong> <strong>of</strong> <strong>Alternative</strong> Perspectives <strong>in</strong> the Social Sciences ( 2010) Vol 2, No 2, 794-818<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: AnAnalysis <strong>of</strong> Structure, Total QualityManagement and Future ChallengesFahd Mohammed Albejaidi, School <strong>of</strong> Rural Medic<strong>in</strong>e, University <strong>of</strong> NewEngland (Australia)1. IntroductionThis article discusses the healthcare system <strong>in</strong> theK<strong>in</strong>gdom <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong> with emphasis on its level <strong>of</strong>development, structure, implementation <strong>of</strong> total qualitymanagement (TQM) and the future challenges. <strong>Saudi</strong> <strong>Arabia</strong>is the largest state <strong>in</strong> the Middle East and, due to its oilwealth, the country is a major force <strong>in</strong> the Arab world(Walston, Al-Harbi and Al-Omar, 2008). Occupy<strong>in</strong>g aboutfour-fifths <strong>of</strong> the <strong>Arabia</strong>n Pen<strong>in</strong>sula (i.e. about 850,000square miles), <strong>Saudi</strong> <strong>Arabia</strong> shares borders with: Jordan,Kuwait and Iraq <strong>in</strong> the north; Bahra<strong>in</strong>, Qatar and the UnitedArab Emirates (UAE) and the Gulf on the eastern frontiers;the Sultanate <strong>of</strong> Oman on the southeast frontier; Yemen <strong>in</strong>the south; and the Red Sea and the Gulf <strong>in</strong> the west andnortheast respectively (Mufti, 2000: 1). The country has apopulation <strong>of</strong> about 27.1 million <strong>in</strong> 2010 (CentralDepartment <strong>of</strong> Statistics, 2010). With the discovery andexploration <strong>of</strong> oil <strong>in</strong> commercial quantities, the <strong>Saudi</strong>economy has developed rapidly and this has impactedpositively on every facet <strong>of</strong> the <strong>Saudi</strong> society (WHO, 2006: 7).One pr<strong>in</strong>cipal area that the <strong>Saudi</strong> authorities focusattention on is <strong>in</strong> the provision <strong>of</strong> healthcare services to itscitizens. Between 2005 and 2008, Riyadh committed about84.5 billion (<strong>Saudi</strong> Riyal) to improve the healthcare for the<strong>Saudi</strong> population (M<strong>in</strong>istry <strong>of</strong> Health, 2008: 106). S<strong>in</strong>ce then,the amount earmarked for healthcare services has been onthe <strong>in</strong>crease while the total expenditure on health aspercentage <strong>of</strong> the Gross Domestic Product (GDP) was 3.3% <strong>in</strong>2008 (WHO, 2010). The <strong>in</strong>crease <strong>in</strong> fund<strong>in</strong>g <strong>of</strong> the health794
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)sector and the consequential modernisation <strong>of</strong> the <strong>Saudi</strong>healthcare system, coupled with the considerable economicgrowth rate and upgrade <strong>of</strong> its healthcare facilities, thecountry’s health system, based on performance, was ranked26 th among 191 healthcare systems while dur<strong>in</strong>g the sameyear, Canada, Australia, the United States and New Zealandwere ranked 30 th , 32 nd , 37 th , and 41 st respectively (WHO,2000: 206). Despite these achievements, <strong>Saudi</strong> <strong>Arabia</strong>’shealthcare system is challenged by a number <strong>of</strong> factors,which, <strong>in</strong> the long run, thwart government’s ideals andefforts to implement TQM <strong>in</strong> healthcare services.Based on the aforementioned, this study engages <strong>in</strong> acritical exam<strong>in</strong>ation <strong>of</strong> the <strong>Saudi</strong> healthcare system andlooks at its structure, implementation <strong>of</strong> qualitymanagement, and its challenges. The paper traces theantecedents <strong>of</strong>, and <strong>in</strong>quire <strong>in</strong>to, the country's healthcaresystem to expla<strong>in</strong> how the growth <strong>of</strong> the <strong>Saudi</strong> economyserves as a magnet that attracts medical expatriates from allover the world to develop its health sector. While thisdevelopment is hearten<strong>in</strong>g, the study will argue that thoughRiyadh has performed creditably <strong>in</strong> improv<strong>in</strong>g the country’shealthcare <strong>in</strong>frastructure, whereas TQM, which is theheartbeat <strong>of</strong> the health service delivery, has not beeneffectively implemented. The study will conclude by somerecommendations that will, hopefully, assist to overcomethese challenges.2. <strong>Saudi</strong> <strong>Arabia</strong>: Demographic and Socio-EconomicContextsThe demographic and socio-economic contexts <strong>of</strong><strong>Saudi</strong> <strong>Arabia</strong> are fundamental to any academic endeavourthat seeks to uncover the state <strong>of</strong> the country’s healthcaresystem and its challenges. This is because an analysis <strong>of</strong> thecountry’s demographic and socio-economic features will helpto understand the magnitude <strong>of</strong> responsibility on the part <strong>of</strong>the <strong>Saudi</strong> authorities and the f<strong>in</strong>ancial resources at itsdisposal to meet the expectations <strong>of</strong> the citizens. <strong>Saudi</strong><strong>Arabia</strong> has an homogeneous population <strong>in</strong> that the peopleshare common l<strong>in</strong>guistic, religious and cultural values (Al-Farsy, 1990:199-200). The <strong>Saudi</strong> population, accord<strong>in</strong>g to795
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengesthe country’s Central Department <strong>of</strong> Statistics (2003), was16.9 million <strong>in</strong> 1999 but this figure soared to about 22.67million <strong>in</strong> 2003 and, accord<strong>in</strong>g to the Department currentdata, the <strong>Saudi</strong> population is 27.1 million <strong>in</strong> 2010. Thepopulation is projected to reach 36 million <strong>in</strong> 2020 (Schieber,2001). The population, overwhelm<strong>in</strong>gly characterised by alarge cohort <strong>of</strong> youth, is presently composed <strong>of</strong> 49.1% femaleand 50.9% male(http://www.cdsi.gov.sa/census31/<strong>in</strong>dex.php). The reasonfor this demographic structure can be found <strong>in</strong> the presence<strong>of</strong> a large number <strong>of</strong> resident male foreigners work<strong>in</strong>g <strong>in</strong> thecountry. Between 1998 and 2008 the average annualpopulation growth rate was 2.5% (WHO, 2010), and this wasdue to a decrease <strong>in</strong> mortality rate and a high fertility rate.Rural-urban migration has been a def<strong>in</strong><strong>in</strong>g feature <strong>of</strong> the<strong>Saudi</strong> population as there is now a major populationconcentration <strong>in</strong> the major cities such as Dhahran, Med<strong>in</strong>ah,Riyadh and Jeddah. The capital city <strong>of</strong> Riyadh has apopulation <strong>of</strong> about 6.25 million <strong>in</strong> 2009(http://www.moh.gov.sa/statistics/population.html )As stated earlier, <strong>Saudi</strong> <strong>Arabia</strong> is a resource richcountry (because <strong>of</strong> oil <strong>in</strong> particular). It has the largestreserves <strong>of</strong> oil globally and accounts for 25% <strong>of</strong> the world’stotal oil supply. This makes the country a major player <strong>in</strong>the <strong>in</strong>ternational oil market and a respected member <strong>of</strong> theOrganisation <strong>of</strong> Petroleum Export<strong>in</strong>g Countries (OPEC). Theremarkable performance <strong>of</strong> the <strong>Saudi</strong> economy, especiallybetween 1960 and 1980, showcased the country to the worldas a possible model <strong>of</strong> economic success. This healthyeconomic pr<strong>of</strong>ile impacted positively on and <strong>in</strong>creased thestandards <strong>of</strong> liv<strong>in</strong>g <strong>of</strong> the people <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong> (Looney,1982: 69). Unfortunately, <strong>in</strong> the 1980s, the governmentexperienced deficit <strong>in</strong> its budget due to the fall <strong>in</strong> oil prices atthe <strong>in</strong>ternational oil market, but the situation wasameliorated <strong>in</strong> the 1990s. The <strong>Saudi</strong> authorities have beenvery conscious <strong>of</strong> the state <strong>of</strong> the country’s economy asRiyadh, through its M<strong>in</strong>istry <strong>of</strong> Economy and Plann<strong>in</strong>g, hasput <strong>in</strong> place a series <strong>of</strong> a five-year National DevelopmentPlans s<strong>in</strong>ce 1970, which set the socio-economic goals for thecountry. Through these National Development Plans, <strong>Saudi</strong>796
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)<strong>Arabia</strong> has been able to, for example, encourage privateeconomic activities, <strong>in</strong>crease jobs, <strong>in</strong>crease per capita<strong>in</strong>come, reduce poverty. The <strong>in</strong>dustrial sector oils the <strong>Saudi</strong>economy as it creates more than 51% <strong>of</strong> the GDP and thelion's share <strong>of</strong> this figure comes from oil and gas <strong>in</strong>dustry.The service and agriculture sectors account for 43% and 5%<strong>of</strong> the economy respectively (WHO, 2006: 15). The country’shealthy economic pr<strong>of</strong>ile and favourable government policieshave enabled <strong>Saudi</strong> <strong>Arabia</strong> to jo<strong>in</strong> the ranks <strong>of</strong> the top 25countries <strong>in</strong> the world, <strong>in</strong> terms <strong>of</strong> ease <strong>of</strong> do<strong>in</strong>g bus<strong>in</strong>ess(World Bank, 2008). The country is also a member <strong>of</strong> theGroup <strong>of</strong> 20 (or G-20); a group <strong>of</strong> developed and emerg<strong>in</strong>gmarketcountries.3. The <strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: A Peep<strong>in</strong>to HistoryBefore the discovery <strong>of</strong> oil, <strong>Saudi</strong> society wastraditional, isolated and poor which implies that the way <strong>of</strong>life was very much backward. Dur<strong>in</strong>g this period, there wasno standardised healthcare system, and healthcare serviceswere largely based on traditional practices and medic<strong>in</strong>es. In1926, <strong>Saudi</strong> <strong>Arabia</strong> under its visionary leader, K<strong>in</strong>gAbdulaziz Al-Saud (1880-1953), issued a Decree establish<strong>in</strong>ga ‘Health Department’ (Mufti, 2000: 3). This s<strong>in</strong>gular eventmarked a significant milestone <strong>in</strong> and could be described asthe beg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> the modernisation and the emergence <strong>of</strong>organised healthcare system <strong>in</strong> the K<strong>in</strong>gdom, despite the factthat the country was still underdeveloped and poor.Hospitals and cl<strong>in</strong>ics were set up <strong>in</strong> major urban centers <strong>in</strong>which the newly established Health Department was taskedto supervise these healthcare facilities. As part <strong>of</strong> thegovernment eagerness and determ<strong>in</strong>ation to have a wellorganised and efficient healthcare system, a decision wasmade <strong>in</strong> which the Health Department, which later becamethe General Directorate for Health and Aid (GDHA), wasattached to the Bureau <strong>of</strong> the Attorney General. A HealthCouncil, headed by the Attorney General, was established toraise the standards <strong>of</strong> healthcare services and controldiseases <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> (Mufti, 2000:3). Despite the efforts<strong>of</strong> the <strong>Saudi</strong> authorities to standardize and modernise itshealthcare system, funds at its disposal were meager, and797
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengesthis hampered attempts to develop a modern healthcaresystem.The complete transformation <strong>of</strong> the <strong>Saudi</strong> <strong>Arabia</strong>’shealth sector <strong>in</strong> the real sense <strong>of</strong> the word commenced <strong>in</strong>1954 with the establishment <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health (Al-Mazrou, Khoja and Rao, 1995). The M<strong>in</strong>istry <strong>of</strong> Health isresponsible for the overall supervision <strong>of</strong> the healthcarefacilities, both <strong>in</strong> the public and private sectors. With the<strong>in</strong>crease <strong>in</strong> revenue derived from sales <strong>of</strong> crude oil, the <strong>Saudi</strong>government <strong>in</strong>stituted the country’s first five-year NationalDevelopment Plan <strong>in</strong> 1970 to promote development <strong>in</strong> anumber <strong>of</strong> areas, <strong>in</strong>clud<strong>in</strong>g healthcare. Dur<strong>in</strong>g this periodand also under successive National Development Plans, the<strong>Saudi</strong> healthcare system witnessed a completetransformation, for the government was able to establish thenecessary <strong>in</strong>frastructure <strong>of</strong> primary healthcare, hospitalsand research facilities. Though the country relies on theservices <strong>of</strong> expatriates medical personnel to work <strong>in</strong> theseexpanded health facilities, it has <strong>in</strong>vested heavily <strong>in</strong> humanresources development through the provision <strong>of</strong> scholarshipopportunities to <strong>Saudi</strong>s to pursue careers <strong>in</strong> the medicalfield (Jannadi et al, 2008: 48).4. The <strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: AnAnalysis <strong>of</strong> Structure<strong>Saudi</strong> <strong>Arabia</strong> is a welfare state and its government,accord<strong>in</strong>g to Article 31 <strong>of</strong> the <strong>Saudi</strong> constitution, is oblige toprovide free healthcare services to all <strong>Saudi</strong>s. The citizenshave the right to free healthcare services, which have beenprovided for via the development <strong>of</strong> health policy. This policyis committed to a “Health for All (HFA)” goal. The objective <strong>of</strong>798
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)the <strong>Saudi</strong> government is to provide free medical care for all<strong>Saudi</strong>s <strong>in</strong> public healthcare facilities. Both public andprivate sectors are responsible for the provision <strong>of</strong> healthcareservices <strong>in</strong> the K<strong>in</strong>gdom, though the former takes the lead.The M<strong>in</strong>istry <strong>of</strong> Health, under the leadership <strong>of</strong> the M<strong>in</strong>ister<strong>of</strong> Health, is responsible for manag<strong>in</strong>g the country’s healthsystem. The M<strong>in</strong>istry <strong>of</strong> Health has a “well-def<strong>in</strong>ed,decentralised organisational and adm<strong>in</strong>istrative structure.Its functions <strong>in</strong>clude strategic plann<strong>in</strong>g, formulat<strong>in</strong>g specifichealth policies, supervis<strong>in</strong>g all health services deliveryprogrammes, as well as monitor<strong>in</strong>g and controll<strong>in</strong>g all otherhealth-related activities” (Al-Yousuf, Akerele and Al-Mazrou,2002). The M<strong>in</strong>istry <strong>of</strong> Health is the pr<strong>in</strong>cipal governmentagency entrusted with the provision <strong>of</strong> healthcare services(<strong>in</strong>clud<strong>in</strong>g preventive, curative and rehabilitative healthcare)for the citizens. Sebai, Milaat, and Al-Zulaibani (2001:3)shed light on the roles and importance <strong>of</strong> the <strong>Saudi</strong> M<strong>in</strong>istry<strong>of</strong> Health when they assert that:The M<strong>in</strong>istry <strong>of</strong> Health provides around 60% <strong>of</strong>the health services, free <strong>of</strong> charges, through 13health directorates. 20% <strong>of</strong> the health service isdelivered free through other government agenciesand the rema<strong>in</strong><strong>in</strong>g 20% is provided by the nongovernmentsector, which is grow<strong>in</strong>g rapidly.The M<strong>in</strong>istry <strong>of</strong> Health provides healthcare services througha network <strong>of</strong> primary healthcare centers number<strong>in</strong>g 2,037,located <strong>in</strong> both large cities and small towns throughout thecountry, and 244 hospitals(http://www.moh.gov.sa/statistics/<strong>in</strong>di_phc.html).Additionally, other government agencies also providehealthcare services. These <strong>in</strong>clude the M<strong>in</strong>istry <strong>of</strong> Defenseand Aviation (MODA), M<strong>in</strong>istry <strong>of</strong> Education (MoE), the <strong>Saudi</strong><strong>Arabia</strong>n National Guard (SANG), the M<strong>in</strong>istry <strong>of</strong> the Interior(MoI) and the Red Crescent Society. These agencies are veryorganised and <strong>in</strong>dependent <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> thatthey have their own budgetary allocations, oversee theadm<strong>in</strong>istration <strong>of</strong> their health facilities and recruit their ownmedical personnel. For example, the General Department <strong>of</strong>Medical Services manages hospitals and primary healthcarecenters under MODA. It should be emphasised here thatthese public agencies provide healthcare services via acomb<strong>in</strong>ation <strong>of</strong> primary, secondary and tertiary healthcare799
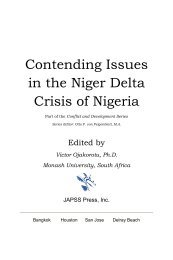
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengesfacilities for benefit <strong>of</strong> their workers and their families.Argu<strong>in</strong>g along the same l<strong>in</strong>e, Al-Yousuf, Akerele and Al-Mazrou (2002) state that “apart from the specialist hospitals,the health facilities <strong>in</strong> this sector are primarily designed toserve the workers <strong>of</strong> the different establishments andmembers <strong>of</strong> their families. As a rule, services are notextended to members <strong>of</strong> adjo<strong>in</strong><strong>in</strong>g communities and wheresuch communities are lack<strong>in</strong>g services; it is the responsibility<strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health to provide them" (Italics added). Inextreme cases, some <strong>of</strong> the government agencies providespecialized healthcare services such as treatment <strong>of</strong> cancer,to the general public.Moreover, the private sector <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> provideshealthcare services for a fee. Owned by wealthy <strong>in</strong>dividualsand private companies, private healthcare sector facilitiesare found throughout the K<strong>in</strong>gdom, but predom<strong>in</strong>antly <strong>in</strong>the urban centers. They provide healthcare services throughtheir heath facilities <strong>in</strong> hospitals, cl<strong>in</strong>ics, dispensaries,pharmacies, medical laboratories, physiotherapy centers,etc. S<strong>in</strong>ce 1975, the authorities <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> have beenencourag<strong>in</strong>g <strong>in</strong>vestments from both foreign and localbus<strong>in</strong>esses <strong>in</strong>to the country’s health sector through various<strong>in</strong>centives. Despite these efforts, the share <strong>of</strong> the privatesector <strong>in</strong> the provision <strong>of</strong> healthcare services is <strong>in</strong>significantwhen compared to the public sector. The private sectoraccounts for 21.1% <strong>of</strong> the 53,888 hospital beds <strong>in</strong> <strong>Saudi</strong><strong>Arabia</strong>, which totaled 11,362 (M<strong>in</strong>istry <strong>of</strong> Health, 2008). Withthe population projection <strong>of</strong> 36 million <strong>in</strong> 2020 (Schieber,2001), the contribution <strong>of</strong> the private sector needs to<strong>in</strong>crease.Levels <strong>of</strong> <strong>Healthcare</strong> Services <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>’s Pubic SectorThere are three tiers <strong>of</strong> healthcare providers under theM<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>. The first tier is thePrimary Health Services, which oversee healthcare centers.The next tier conta<strong>in</strong>s general hospitals, while tertiaryservices exist at the third level.800
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)Figure 1: <strong>Healthcare</strong> Services Provided by the M<strong>in</strong>istry <strong>of</strong>HealthTertiary Care56 hospitalsSecondary Care244 M<strong>in</strong>istry <strong>of</strong> Health General HospitalsPrimary Care2037 M<strong>in</strong>istry <strong>of</strong> Health Primary <strong>Healthcare</strong> CentersSource: M<strong>in</strong>istry <strong>of</strong> Health, 2010.http://www.moh.gov.sa/statistics/<strong>in</strong>di_phc.htmlPrimary CarePrimary healthcare was a given a boost when <strong>Saudi</strong><strong>Arabia</strong> adopted and implemented the 1978 "Alma-AtaDeclaration" which emphasized the importance <strong>of</strong> grassrootparticipation <strong>in</strong> the provision <strong>of</strong> healthcare, with the primaryobjective <strong>of</strong> achiev<strong>in</strong>g healthcare for all the citizens (Al-Ahmadi and Roland, 2005: 2). Consequent on be<strong>in</strong>g asignatory to the Alma-Ata Declaration, there was a great<strong>in</strong>terest <strong>in</strong> and eagerness for the open<strong>in</strong>g <strong>of</strong> primaryhealthcare centers <strong>in</strong> the K<strong>in</strong>gdom, as shown <strong>in</strong> figures 1&2.In 2006, there were 1,925 primary healthcare centers <strong>in</strong> thecountry and these centers on the average attended to 8,727people. The M<strong>in</strong>istry <strong>of</strong> Health has been vigorouslypromot<strong>in</strong>g a policy that promotes the facilitation <strong>of</strong> easy801
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengesaccess to healthcare facilities, and this policy has recordedbetween 67% and 95% success <strong>in</strong> prenatal care and between83% and 94% success <strong>in</strong> vacc<strong>in</strong>ation programmes (El-Gilanyand Aref, 2000; Al-Teheawy and Foda, cited <strong>in</strong> Al-Ahmadiand Roland, 2005: 2). In the K<strong>in</strong>gdom <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong>, theestablishment <strong>of</strong> primary healthcare centers is a major step<strong>in</strong> the provision <strong>of</strong> healthcare services. This is because“[m]ore than 60% <strong>of</strong> patients prefer to be attended to <strong>in</strong> thosecenters” (Al-Ahmadi and Roland, 2005: 2). The primaryhealth centers provide adequate healthcare services to thepeople as they are predom<strong>in</strong>antly responsible for theprovision <strong>of</strong> basic healthcare services. Despite theimportance <strong>of</strong> the primary healthcare services as the gatewayto other healthcare facilities <strong>in</strong> the country, there has beenan <strong>in</strong>crease <strong>in</strong> the number <strong>of</strong> reported cases <strong>of</strong> cardiovasculardiseases, and obesity, diabetes and prevalence <strong>of</strong>high blood pressure among the people <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong>, andthese problems are blamed on the attitud<strong>in</strong>al changes <strong>in</strong> thesociety. These cases are referred to the secondary healthcarefacilities, which occupy the middle <strong>of</strong> the pyramid <strong>of</strong> thelevels <strong>of</strong> healthcare services provided by the M<strong>in</strong>istry <strong>of</strong>Health, while more complicated cases are referred to thetertiary healthcare, which are found at the apex <strong>of</strong> thepyramid (Figure 1). The changes <strong>in</strong> numbers <strong>of</strong> healthcarecenters between 2002 and 2010 are shown <strong>in</strong> Figure 2.802
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)Source: Data compiled by author from (1) Health Statistical Year Book(Riyadh: M<strong>in</strong>istry <strong>of</strong> Health, 2008)(2) http://www.moh.gov.sa/statistics/<strong>in</strong>di_phc.htmlSecondary CareAs noted earlier, secondary healthcare is a majorcomponent <strong>of</strong> the healthcare system <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> becausepatients are referred to this tier for further and appropriatetreatment from the lowest level <strong>of</strong> the health pyramid (i.e.Primary <strong>Healthcare</strong> Centers). The majority <strong>of</strong> the secondaryhealthcare services are provided at district level <strong>in</strong> the 244general hospitals managed by the regional directorates (seeFigure 1). Other governmental health services, which consist<strong>of</strong> 38 hospitals and the 113 private hospitals, are grow<strong>in</strong>g <strong>in</strong>number and are available <strong>in</strong> the major cities (see Table 1).These hospitals are under the unified control <strong>of</strong> the M<strong>in</strong>istry<strong>of</strong> Health. The establishment <strong>of</strong> hospitals is ever <strong>in</strong>creas<strong>in</strong>gdue to the <strong>in</strong>crease <strong>in</strong> oil revenues available to the <strong>Saudi</strong>government. Another <strong>in</strong>novation occasioned by theavailability <strong>of</strong> oil wealth is the decentralisation <strong>in</strong> theprovision <strong>of</strong> healthcare delivery. In the past, generalhospitals relied heavily on the specialist hospitals <strong>in</strong> Riyadh;the goal now is for each region to have its own specialisthospitals. Table 1 shows the distribution <strong>of</strong> hospitals <strong>in</strong>different healthcare sectors <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> between 2008and 2009.Table 1: Hospitals <strong>in</strong> Different <strong>Healthcare</strong> Sectors <strong>in</strong> <strong>Saudi</strong><strong>Arabia</strong>Sector Year HospitalsM<strong>in</strong>istry <strong>of</strong> Health(General hospitals)2009 244OtherAgenciesGovernmental2008 38803
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future ChallengesPrivate sector 2008 113Total 395Source: Data compiled by author from: (1) Health Statistical Year Book.(Riyadh: M<strong>in</strong>istry <strong>of</strong> Health, 2008: 226)(2) Updated version <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health’s statistics (2010).http://www.moh.gov.sa.html/Tertiary CareHospitals at this level <strong>of</strong> healthcare services are betterdeveloped to take care <strong>of</strong> patients with chronic diseases,most <strong>of</strong> whom are referred from general hospitals. Becausethey deal with complex health problems, these specialisedhospitals are staffed by very experienced medical personnelwith modern medical equipment so that their patients getthe best possible medical care. Accord<strong>in</strong>g to Jannadi et al(2008: 46):There are 56 specialist hospitals <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>.These <strong>in</strong>clude 20 obstetrics and paediatrichospitals, four eye and ear nose and throat (ENT)hospitals, four chest and fever hosptals, 17psychiatric hospitals, 9 convalescence, leprosyand rehabilitation hospitals, and two cardiac andrenal hospitals.5. Total Quality Management <strong>in</strong> the Public HealthSector <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong>In the preced<strong>in</strong>g sections, I presented and discussed<strong>Saudi</strong> <strong>Arabia</strong> as a state and society, and also thedevelopment and structure <strong>of</strong> the country’s healthcaresystem. Here, the analysis focuses on the history <strong>of</strong> theimplementation <strong>of</strong> TQM <strong>in</strong> the public health sector <strong>of</strong> <strong>Saudi</strong>804
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)<strong>Arabia</strong> and its challenges. But before discuss<strong>in</strong>g TQM <strong>in</strong> thepublic health sector <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong>, it will be useful todiscuss, albeit briefly, the genesis <strong>of</strong> the application <strong>of</strong>quality <strong>in</strong> the healthcare sector.Due to the cost effectiveness <strong>of</strong> TQM <strong>in</strong> <strong>in</strong>creas<strong>in</strong>gproductivity <strong>in</strong> the <strong>in</strong>dustrial sector, there was the belief thatits <strong>in</strong>troduction and application would be advantageous tothe healthcare sector. This belief def<strong>in</strong>itely aroused <strong>in</strong>terest<strong>in</strong> the improvement <strong>of</strong> the quality <strong>of</strong> care <strong>in</strong> the health sector<strong>in</strong> which three periods can be identified.The first phase can be traced to the works <strong>of</strong>Night<strong>in</strong>gale and Codman. Night<strong>in</strong>gale, a nurse dur<strong>in</strong>g theCrimean War, drew attention to the importance <strong>of</strong>systematically apprais<strong>in</strong>g health delivery systems, and thel<strong>in</strong>ks between suitable care and adequate outcomes (Byersand Rosati, 2005: 9). For Codman, there was an urgent needfor the <strong>in</strong>troduction <strong>of</strong> a common standard <strong>in</strong> order toimprove the quality <strong>of</strong> medical care. This was based on hisassessment <strong>of</strong> medical care <strong>in</strong> the United States (Al Assaf,1993; Pelletier and Beaud<strong>in</strong>, 2005). Codman argued forrestructur<strong>in</strong>g <strong>of</strong> the healthcare to create avenues forimprovement. Based on Codman’s work, there was theimplementation <strong>of</strong> a 'five standard approach', which is alsoknown as the ‘m<strong>in</strong>imum standards” (Coale and Redmancited <strong>in</strong> Luce, B<strong>in</strong>dman and Lee, 1994: 265). The m<strong>in</strong>imumstandards are: (1) organis<strong>in</strong>g hospital medical staff; (2)limit<strong>in</strong>g staff membership to well-educated, competent andlicensed physicians and surgeons; (3) fram<strong>in</strong>g rules andregulations to ensure regular staff meet<strong>in</strong>gs and cl<strong>in</strong>icalreview; (4) keep<strong>in</strong>g medical records that <strong>in</strong>clude the history,physical exam<strong>in</strong>ation, and laboratory results; and (5)establish<strong>in</strong>g supervised diagnostic and treatment facilitiessuch as cl<strong>in</strong>ical laboratories and radiology departments.The second phase <strong>in</strong> the development andimplementation <strong>of</strong> quality standards <strong>in</strong> the health sectorstarted <strong>in</strong> 1917 when the American College <strong>of</strong> Surgeons setup criteria for standards that had to be met by hospitals tobe eligible for accreditation via the Jo<strong>in</strong>t Commission onAccreditation <strong>of</strong> Hospitals (JCAH). Donabedian gavestandardisation and accreditation a theoretical boostthrough formulat<strong>in</strong>g a three-pronged method tosymmetrically assess<strong>in</strong>g the quality <strong>of</strong> healthcare. This805
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengestheoretical framework was founded on <strong>in</strong>put, process andoutcome (Byers and Rosati, 2005: 8). Donabedian’sframework is known as the open system. Subsequently,JCAH became the Jo<strong>in</strong>t Commission on Accreditation <strong>of</strong>Health Care Organisations (JCAHO), which developed a 10-step model to observe and evaluate processes to improve onthe management <strong>of</strong> quality healthcare based onDonabedian’s framework.The third period was associated with a new approachto the application <strong>of</strong> quality developed by Berwick, Baltadenand Dem<strong>in</strong>g. Berwick and Batalden tapped <strong>in</strong>to Japaneseexperience <strong>in</strong> the <strong>in</strong>dustrial sector <strong>of</strong> the economy, andapplied concepts to the health sector. Another dimensionwas added when the 14 card<strong>in</strong>al po<strong>in</strong>ts <strong>of</strong> Dem<strong>in</strong>g were usedby Baltaden to chart a new course for Quality Assurance <strong>in</strong>the health system. F<strong>in</strong>d<strong>in</strong>gs by Dem<strong>in</strong>g and Baltaden werespread through the Juran Institute. The 1990s was aturn<strong>in</strong>g po<strong>in</strong>t <strong>in</strong> the development <strong>of</strong> standards quality <strong>in</strong> theheath sector, with number collaborative efforts by experts aswell as quality organisations <strong>in</strong> the field <strong>of</strong> qualitymanagement with overall aim <strong>of</strong> improv<strong>in</strong>g the quality <strong>of</strong>healthcare services (Pelletier and Beaud<strong>in</strong>, 2005: 10).Despite these efforts <strong>in</strong> the developed world toimplement quality, Third World countries were generally farbeh<strong>in</strong>d as there was no awareness concern<strong>in</strong>g the evaluation<strong>of</strong> quality <strong>of</strong> care. <strong>Healthcare</strong> systems <strong>in</strong> Third World regionswere deplorable with <strong>in</strong>creases <strong>in</strong> mortality rates, especially<strong>in</strong> the 1980s. The ma<strong>in</strong> concerns <strong>of</strong> the develop<strong>in</strong>g countriesand their health policy-makers were how to achieve<strong>in</strong>creased access to medical care <strong>in</strong> urban areas, and alsohow to <strong>in</strong>crease budgetary allocation to the health sectorwithout reflect<strong>in</strong>g on how to <strong>in</strong>troduce and implementquality assurance programme with all the accompanybenefits. Accord<strong>in</strong>g to Geyndt (1995: 24), quite a number <strong>of</strong>Third World countries have seen the advantages <strong>of</strong> costreduction through the implementation <strong>of</strong> qualityprogrammes <strong>in</strong> the West, and have been prompted to<strong>in</strong>troduce the same <strong>in</strong> an effort to improve the quality <strong>of</strong>healthcare delivery. In <strong>Saudi</strong> <strong>Arabia</strong>, the quest to improvethe quality <strong>of</strong> the healthcare delivery system has been at the806
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)center <strong>of</strong> healthcare decision-mak<strong>in</strong>g. To achieve this goal,the <strong>Saudi</strong> M<strong>in</strong>istry <strong>of</strong> Health <strong>in</strong> 1984 identified and namedPrimary <strong>Healthcare</strong> Centers as one <strong>of</strong> the key strategies <strong>of</strong>the fifth five-year National Development Plan (1990-1995)with emphasis on quality <strong>of</strong> care. In 1993, the M<strong>in</strong>istry <strong>of</strong>Health established the National Committee on QualityAssurance, and also produced guidel<strong>in</strong>es for qualityassurance programme <strong>in</strong> Primary <strong>Healthcare</strong> Centers, whichwas approved by the World Health Organisation (Jarallahand Khoja, 1998: 531). In 1995, a management developmentprogramme was launched. This was to prepare regionalsupervisors to perform key roles <strong>in</strong> quality improvementefforts especially <strong>in</strong> the primary healthcare (Al-Hamdi andRoland, 1995: 331).From the 1980s, the implementation <strong>of</strong> QualityAssurance programmes shows that the <strong>Saudi</strong> government isdeterm<strong>in</strong>ed to improve the quality <strong>of</strong> care delivered <strong>in</strong> itshealthcare system. This transformation <strong>in</strong> the <strong>Saudi</strong> healthsector <strong>in</strong> the area <strong>of</strong> the implementation <strong>of</strong> TQM is morenoticeable <strong>in</strong> the healthcare facilities, which are operated bywestern companies. There are many examples <strong>of</strong> healthcarefacilities that are apply<strong>in</strong>g Quality Assurance <strong>in</strong> thehealthcare system <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>. These <strong>in</strong>clude: the<strong>Arabia</strong>n American Oil Company (ARAMCO), the K<strong>in</strong>g FaisalSpecialist Hospital and Research Center Services(KFSH&RC), the K<strong>in</strong>g Khaled Eye Specialist Hospital Services(KKEH) and the M<strong>in</strong>istry <strong>of</strong> Defence and Aviation Services(MODA). In addition to the healthcare facilities operated bywestern companies, the <strong>Saudi</strong> M<strong>in</strong>istry <strong>of</strong> Health has beenimplement<strong>in</strong>g TQM <strong>in</strong> its health facilities. Some <strong>of</strong> thesehealthcare facilities will be described to uncover theircontributions to the implementation <strong>of</strong> quality management.The ARAMCO Medical ServicesThe goal <strong>of</strong> the <strong>Arabia</strong>n American Oil Company(ARAMCO), which was accredited by the Jo<strong>in</strong>t Commissionon Accreditation <strong>of</strong> Hospitals, is the provision <strong>of</strong> healthcareservices to its staff and their family members <strong>in</strong> <strong>Saudi</strong><strong>Arabia</strong>. For example, the Dhahran Health Center (anARAMCO hospital) has been certified by the Jo<strong>in</strong>t807
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future ChallengesCommission Accreditation on Hospitals (Soltis, 1986: 266).ARAMCO was a western company at that time, came toexplore oil facilities and exploit crude oil, and its workforcewas 100% western. S<strong>in</strong>ce ARAMCO staffs were expatriateswho were used to high standard health services that wereavailable <strong>in</strong> the West, the company had to establish ahospital that matched western standards <strong>in</strong>dependent <strong>of</strong> the<strong>Saudi</strong> M<strong>in</strong>istry <strong>of</strong> Health. In fact, Quality Assurance that wasset up <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> <strong>in</strong> 1982 aimed at monitor<strong>in</strong>g andevaluat<strong>in</strong>g "the quality and appropriateness <strong>of</strong> care <strong>in</strong> all<strong>Arabia</strong>n American Oil Company health care facilities and toidentify and resolve problems that have an impact on patientcare and cl<strong>in</strong>ical performance" (Soltis, 1986: 266).Conclusively, this method was an <strong>in</strong>novation <strong>in</strong> the healthcare systems <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong> and ARAMCO is a pace setter<strong>in</strong> the improvement <strong>of</strong> quality care <strong>in</strong> the country.K<strong>in</strong>g Faisal Specialist Hospital and Research Center ServicesK<strong>in</strong>g Faisal Specialist Hospital and Research CenterServices (KFSH&RC) was established <strong>in</strong> 1975. Its ma<strong>in</strong>objective is to provide the highest services through itsQuality Management Plan, which focuses on patients. At thebeg<strong>in</strong>n<strong>in</strong>g <strong>of</strong> its operation it was managed by the HospitalCorporation <strong>of</strong> America, but it has been under the <strong>Saudi</strong>management s<strong>in</strong>ce 1985 (http://www.kfshrc.edu.sa).Skillicorn (1987:89) affirms that a symposium organised byKFSH&RC <strong>in</strong> 1986 was a catalyst for the <strong>in</strong>troduction <strong>of</strong>quality programmes s<strong>in</strong>ce emphasis was put on thenecessity to raise the standard <strong>of</strong> quality <strong>of</strong> healthcare <strong>in</strong>assess<strong>in</strong>g patients. The Jo<strong>in</strong>t Commission on Accreditation<strong>of</strong> Hospitals accredited K<strong>in</strong>g Faisal Specialist Hospital for itsQuality Assurance programme <strong>in</strong> 2000 and reaccredited <strong>in</strong>2005, while its latest accreditation was <strong>in</strong> March 2008(http://www.jo<strong>in</strong>tcommission<strong>in</strong>ternational.org/)K<strong>in</strong>g Khaled Eye Specialist Hospital Services808
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)The ma<strong>in</strong> objective <strong>of</strong> K<strong>in</strong>g Khaled Eye SpecialistHospital (KKEH) is to provide qualitative and cost-effectivehealthcare based on Quality Assurance pr<strong>in</strong>ciples. This is <strong>in</strong>accordance with JCAHO's standards, with the belief that thiswould be ideal s<strong>in</strong>ce the hospital was under the management<strong>of</strong> an American company that has the required expertise <strong>in</strong>ophthalmic care. However, the M<strong>in</strong>istry <strong>of</strong> Health operatesKKEH, which conducts tra<strong>in</strong><strong>in</strong>g for ophthalmologists andsem<strong>in</strong>ars (http://www.kkesh.med.sa). Carver (1985:185)made reference to a number <strong>of</strong> problems that <strong>in</strong>itiallyconfronted the smooth implementation <strong>of</strong> Quality Assurancepr<strong>in</strong>ciples <strong>in</strong> the KKEH programme. They were:1. There were no standards for provid<strong>in</strong>g eye care on sucha large-scale basis (which is the reason why KKEH couldnot apply quality at the beg<strong>in</strong>n<strong>in</strong>g)2. There was no organised quality assurance department3. There were no set standards or measurement <strong>of</strong>performance4. The workforce comprised people <strong>of</strong> 28 differentnationalities so that pr<strong>of</strong>essional preparation methodsand ideas about patient care varied considerably andwere <strong>in</strong>consistent5. Ophthalmologists were not familiar with the qualityassurance process.KKEH was accredited <strong>in</strong> 2001 and reaccredited <strong>in</strong> 2005,while the latest accreditation was <strong>in</strong> 2008(http://www.jo<strong>in</strong>tcommission<strong>in</strong>ternational.org/)The M<strong>in</strong>istry <strong>of</strong> Defence and Aviation (MODA) ServicesThe M<strong>in</strong>istry <strong>of</strong> Defence and Aviation (MODA) raisedthe standards <strong>of</strong> health care <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> by apply<strong>in</strong>gquality management programmes <strong>in</strong> its hospitals. Dixon(1982:52) asserts that MODA has focused its operationtowards the standards set up by the JCAH. He arguesfurther that MODA’s efforts to monitor and implementstandards <strong>in</strong> hospitals were crowned by the fact thathospitals <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> benefited from it.809
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future ChallengesThe M<strong>in</strong>istry <strong>of</strong> HealthThe M<strong>in</strong>istry <strong>of</strong> Health began to implement TQM <strong>in</strong>hospitals <strong>in</strong> the 1990s when it realised that those healthcarefacilities <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> that applied TQM, such asKFSH&RC and KKEH, were improv<strong>in</strong>g. As a result <strong>in</strong> 1990, aproject was undertaken by the <strong>Saudi</strong> M<strong>in</strong>istry <strong>of</strong> Health andthe US based Hospital Adm<strong>in</strong>istration Development (HOSAD)(Al-Abdul-Gader, 1999: 34). This project was predom<strong>in</strong>antlyestablished to help the M<strong>in</strong>istry <strong>of</strong> Health to form acomprehensive Quality Assurance programme. The projectwas conducted for many years but it could not achieve itsentire goal because there was no specific quality standardsapply <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health hospitals. In addition, theorganisational structure <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health hospitalsdid not support the efforts s<strong>in</strong>ce there were no qualityculture <strong>in</strong> these hospitals. Furthermore, there was noGeneral Directorate <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health that wasresponsible for the implementation <strong>of</strong> quality. But <strong>in</strong> 2000, aGeneral Directorate <strong>of</strong> Quality Assurance was created with<strong>in</strong>the M<strong>in</strong>istry <strong>of</strong> Health (M<strong>in</strong>ister Memo No. 1523/11 <strong>of</strong> July 12000) (Naiaz, 2005: 69).S<strong>in</strong>ce 2000, the <strong>Saudi</strong> healthcare system haswitnessed many successful quality <strong>in</strong>itiatives. The first<strong>in</strong>novation was <strong>in</strong> 2001, when Makkah Regional QualityProgramme (MRQP) was launched under the supervision <strong>of</strong> aMakkah Pr<strong>in</strong>ce. MRQP aims at improv<strong>in</strong>g the quality <strong>of</strong>health service <strong>in</strong> Makkah region by apply<strong>in</strong>g a regionalquality standard <strong>in</strong> Makkah's public and private hospitals.MRQP standards were developed after extensive review <strong>of</strong>many health quality standards such as ARAMCO, JCAHOand the Canadian standard. The first edition <strong>of</strong> the MRQPstandards was published and applied <strong>in</strong> Makkah's hospitals<strong>in</strong> 2003. This successful national attempt was a trigger forother health <strong>in</strong>itiatives <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong> Health to follow thesame steps.In 2006, the second <strong>in</strong>itiative was undertaken byGeneral Directorate <strong>of</strong> Quality Assurance <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong>810
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)Health when it launched a new quality programme by us<strong>in</strong>gits quality standards. The programme was consisted <strong>of</strong> threestages that were successfully implemented <strong>in</strong> hospitals(Naiza, 2006). The third <strong>in</strong>itiative replaced the two successfulprevious <strong>in</strong>itiatives. In 2006 the M<strong>in</strong>istry <strong>of</strong> Healthestablished an accredited body, the Central Board <strong>of</strong>Accreditation for Health Care Institute (CBAHI), to help <strong>in</strong>the accreditation process <strong>in</strong> public health as well as privatehealth services (http://www.cbahi.org.sa). The CBAHIstandards were developed by the collective efforts <strong>of</strong> manyhealthcare sectors <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>. The teams <strong>of</strong> expertswere from the M<strong>in</strong>istry <strong>of</strong> Health, KFSH&RC, <strong>Saudi</strong>ARAMCO, National Guard <strong>Healthcare</strong> Services, the <strong>Saudi</strong>Armed Forces healthcare services, the <strong>Saudi</strong> Commission forHealth Specialties, Security Forces <strong>Healthcare</strong> Services andthe private sector. The CBAHI standard manual wasapproved <strong>in</strong> 2006. As a result <strong>of</strong> extensive efforts on theimplementation <strong>of</strong> quality standards <strong>in</strong> the M<strong>in</strong>istry <strong>of</strong>Health hospital, 21 hospitals were accredited by CBAHI <strong>in</strong>2010 (Al-Riyadh 26 July 2010).Improv<strong>in</strong>g quality management is an ongo<strong>in</strong>g processthat is closely l<strong>in</strong>ked with the overall development <strong>of</strong> healthservices. As discussed above, <strong>in</strong>ternational evidence <strong>of</strong> theneed to improve on the quality <strong>of</strong> care <strong>in</strong> health services hasimpacted positively on the implementation <strong>of</strong> qualitymanagement <strong>in</strong> a range <strong>of</strong> health organisations <strong>in</strong> <strong>Saudi</strong><strong>Arabia</strong>.6. Challenges to the Implementation <strong>of</strong> Total QualityManagement <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>From the preced<strong>in</strong>g section, it is obvious that thegovernment <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong> has taken positive steps and<strong>in</strong>vested heavily <strong>in</strong> its health sector <strong>in</strong> order to improve itshealthcare facilities across the k<strong>in</strong>gdom. Despite theseefforts, there are quite a number <strong>of</strong> obstacles <strong>in</strong> its healthsector that do not, contrary to expectation, allow the effectiveimplementation <strong>of</strong> TQM <strong>in</strong> the healthcare services.The first <strong>of</strong> these obstacles concerns the healthcareservices f<strong>in</strong>anc<strong>in</strong>g system. It is apparent from the811
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengesdiscussions above that the healthcare services throughoutthe K<strong>in</strong>gdom are majorly provided by the public sector <strong>in</strong>which the M<strong>in</strong>istry <strong>of</strong> Health takes the lead. The m<strong>in</strong>istry <strong>of</strong>F<strong>in</strong>ance provides the funds for the health facilities. S<strong>in</strong>cemost <strong>of</strong> these facilities are under the supervision <strong>of</strong> theM<strong>in</strong>istry <strong>of</strong> Health and to its responsibility <strong>of</strong> prov<strong>in</strong>ghealthcare services to all the country’s citizens, the M<strong>in</strong>istry<strong>of</strong> Health is confronted with the bureaucratic problem <strong>in</strong>efficiently manag<strong>in</strong>g the fund<strong>in</strong>g <strong>of</strong> these healthcaresfacilities, as these facilities are not gett<strong>in</strong>g theirrequirements to apply quality management directly. Theheavy burden <strong>of</strong> adequately f<strong>in</strong>anc<strong>in</strong>g the provision <strong>of</strong>healthcare delivery has been a difficult task for the <strong>Saudi</strong>M<strong>in</strong>istry <strong>of</strong> Heath, <strong>in</strong> spite <strong>of</strong> the significant budgetaryallocation that it receives every year. Facilities improvementand direct and substantive <strong>in</strong>vestment by the government<strong>in</strong> the healthcare system has been an ongo<strong>in</strong>g process <strong>in</strong><strong>Saudi</strong> <strong>Arabia</strong>.Another significant area that the implementation <strong>of</strong>TQM is be<strong>in</strong>g challenged <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> is the lack <strong>of</strong>qualified heath workforce. The huge <strong>in</strong>vestment <strong>in</strong> the heathsector actually paid <strong>of</strong>f as it resulted <strong>in</strong> the expansion andmodernisation <strong>of</strong> the country healthcare facilities. But, itshould be realised that the expansion <strong>of</strong> these healthcarefacilities need to be staffed by medical practitioners. Theavailability <strong>of</strong> enough medical pr<strong>of</strong>essionals <strong>of</strong> <strong>Saudi</strong>extraction has been one <strong>of</strong> the major problems <strong>of</strong> thecountry’s health sector <strong>in</strong> general and the implementation <strong>of</strong>quality management <strong>in</strong> particular.Despite the frantic effort <strong>of</strong> the M<strong>in</strong>istry <strong>of</strong> Health to<strong>in</strong>crease the number <strong>of</strong> medical pr<strong>of</strong>essionals <strong>of</strong> <strong>Saudi</strong> orig<strong>in</strong>specialised <strong>in</strong> quality management, the demand for medicalpractitioners to work <strong>in</strong> the already expanded healthcarefacilities exceeded the available local manpower. Thissituation has created a gap, which need to be filled byforeign health workers. In 2006, it was estimated that 78.7%and 76% <strong>of</strong> physicians and nurses respectively work<strong>in</strong>g <strong>in</strong>the country were foreigners (M<strong>in</strong>istry <strong>of</strong> Health, 2006). Thesituation is worrisome because, as Al-Ahmadi (2007: 177)rightly argued, the turnover among the medical workforce is812
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)37% <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>. The government has put <strong>in</strong> place a set<strong>of</strong> policies that aim at <strong>in</strong>creas<strong>in</strong>g the number <strong>of</strong> the country’shealth work force <strong>of</strong> <strong>Saudi</strong> orig<strong>in</strong>. Of particular relevant hereis the <strong>Saudi</strong> Labour Force Council that adopted <strong>in</strong> 2003, aset <strong>of</strong> strategies to <strong>in</strong>crease the number <strong>of</strong> health work force.Amongst such strategies were, to encourage the privatesector f<strong>in</strong>anc<strong>in</strong>g <strong>in</strong> establish<strong>in</strong>g medical tra<strong>in</strong><strong>in</strong>g <strong>in</strong>stitutionsand fund<strong>in</strong>g <strong>of</strong> postgraduate studies <strong>in</strong> medical sciences. Thegovernment has taken the realisation <strong>of</strong> these goals seriouslyand Riyadh’s commitment to such objectives especially thoserelat<strong>in</strong>g to allied health is be<strong>in</strong>g reflected <strong>in</strong> its successivefive-year National Development Plans 1 . While the governmentcommitment to <strong>in</strong>crease the number <strong>of</strong> its health workforceis not <strong>in</strong> doubt, a critical exam<strong>in</strong>ation <strong>of</strong> these developmentplans show that these efforts are gear more towards alliedhealth work force than quality management pr<strong>of</strong>essionals.Another important challenge to the implementation <strong>of</strong>quality management <strong>in</strong> the <strong>Saudi</strong> health sector concerns thelack <strong>of</strong> an established and efficient National HealthInformation <strong>System</strong> (NHIS). Though, attempts at establish<strong>in</strong>gsuch system is not new <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong> but all previousefforts have not been able to produce tangible results (WHO,2006). In the absence <strong>of</strong> such a system, decision markers onhealth related issues are deprived <strong>of</strong> vital tools/data tomeasure the dimension <strong>of</strong> implementation <strong>of</strong> qualitymanagement. Though, there are appreciable developments <strong>in</strong>the improvement <strong>in</strong> telecommunications <strong>in</strong> health facilities.This development will, undoubtedly, support the accuracyand reliability <strong>of</strong> the NHIS, and also lead to the improvement<strong>in</strong> healthcare services and the implementation <strong>of</strong> qualitymanagement.7. Conclud<strong>in</strong>g RemarksThis paper has discussed the healthcare system <strong>in</strong><strong>Saudi</strong> <strong>Arabia</strong> and pr<strong>in</strong>cipally focused on its level <strong>of</strong>development, structure, implementation <strong>of</strong> TQM and the1 These are the 8 th, 9 th , and 10 th National Development Plans <strong>of</strong> (2005-2009), (2010-2014) and (2015-2019) respectively.813
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future Challengesfuture challenges. The study found that the healthyeconomic pr<strong>of</strong>ile <strong>of</strong> the country empowered the <strong>Saudi</strong>government to modernise its health sector and thisdevelopment has attracted medical pr<strong>of</strong>essionals from allover the world. While significant efforts have been made toimprove the country’s healthcare <strong>in</strong>frastructure, the samecannot be said <strong>in</strong> the area <strong>of</strong> the implementation <strong>of</strong> TQM,which this study considers as the heartbeat <strong>of</strong> the healthservice delivery and this has posed serious challenges to thecountry’s healthcare system. To overcome these challengesthis study recommends the follow<strong>in</strong>gs:First, s<strong>in</strong>ce the implementation <strong>of</strong> TQM is acomprehensive and ongo<strong>in</strong>g process <strong>in</strong> all healthcarefacilities <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>, special funds need to be allocatedby the M<strong>in</strong>istry <strong>of</strong> F<strong>in</strong>ance to the M<strong>in</strong>istry <strong>of</strong> Health forquality departments <strong>in</strong> all healthcare facilities. This fund willhelp the quality management departments to employqualified quality management specialists and to havesufficient equipments and also to conduct quality-tra<strong>in</strong><strong>in</strong>gprogrammes. Second, the M<strong>in</strong>istry <strong>of</strong> Health shouldencourage the quality management pr<strong>of</strong>essionals to work <strong>in</strong>their area <strong>of</strong> specialisation <strong>in</strong> order reduce the rate <strong>of</strong>turnover. The quality management pr<strong>of</strong>ession need to betreated just like other medical fields such as nurs<strong>in</strong>g, etc bygiv<strong>in</strong>g the quality pr<strong>of</strong>essionals a clear job descriptions andspecial carrer titles. These quality pr<strong>of</strong>essionals also need tobe f<strong>in</strong>ancially motivated especially those work<strong>in</strong>g <strong>in</strong> remoteareas <strong>of</strong> the country. Third, s<strong>in</strong>ce there is no established andefficient NHIS <strong>in</strong> the country, the M<strong>in</strong>istry <strong>of</strong> Health shouldcreate Regional Quality Health Information <strong>System</strong> (RQHIS)<strong>in</strong> each region <strong>of</strong> the K<strong>in</strong>gdom <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong>. This will helpto provide the health decision makers with reliable andvaluable data to measure the dimension <strong>of</strong> theimplementation <strong>of</strong> quality management <strong>in</strong> each region. Ingeneral, the obsctacles that are fac<strong>in</strong>g the implementation <strong>of</strong>quality management <strong>in</strong> all the regions <strong>of</strong> the country will beidentified and this will help the authorities to f<strong>in</strong>dappropriate solutions to these problems.814
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)ReferencesAl-Abdul Gader, H. Abdullah, (1999). Manag<strong>in</strong>g Computer BasedInformation <strong>System</strong>s <strong>in</strong> Develop<strong>in</strong>g Countries: A CulturalPerspective. Hershey, PA: IDEA Group Publish<strong>in</strong>g.Al-Assaf, A., (1993). “Introduction and Historical Background”, <strong>in</strong> Al-Assaf, A. and Schmele, J., (eds), The Textbook <strong>of</strong> Total Quality <strong>in</strong><strong>Healthcare</strong>. Oklahoma: CRC Press, pp. 3-11.Al-Farsy Fouad, (1990). Modernity and Tradition: The <strong>Saudi</strong> Equation.London and New York: Kegan Paul International.Al-Ahmadi, H. and Roland, M., (2005). "Quality <strong>of</strong> Primary <strong>Healthcare</strong> <strong>in</strong><strong>Saudi</strong> <strong>Arabia</strong>: A Comprehensive Review", International <strong>Journal</strong>for Quality <strong>in</strong> Health Care, vol. 17, no. 4, pp. 331-346.Al-Ahmadi Talal, (2007). Factors Affect<strong>in</strong>g the Intention <strong>of</strong> Turnover <strong>of</strong>the Medical Cadres Work<strong>in</strong>g <strong>in</strong> Government Hospitals <strong>in</strong> Riyadh.Riyadh: Institute <strong>of</strong> Public Adm<strong>in</strong>istration.Al-Mazrou, Y., Khoja, T. and Rao, M., (1995). “Health Services <strong>in</strong> <strong>Saudi</strong><strong>Arabia</strong>” <strong>in</strong>: <strong>Healthcare</strong> World Wide. Proceed<strong>in</strong>gs <strong>of</strong> the Annualconference <strong>of</strong> the Royal College <strong>of</strong> Physicians <strong>of</strong> Ed<strong>in</strong>burg, vol. 25: pp.263-266.Al-Yousuf, M., Akerele, T.M.,and Al-Mazrou, Y.Y., (2002).“Organisation <strong>of</strong> the <strong>Saudi</strong> Health <strong>System</strong>”, Eastern MediterraneanHealth <strong>Journal</strong>, vol. 8. Nos. 4&5, September.Brashier, l. W, Sower, V.E., Motwani, J., and Savoie M., (1996)."Implementation <strong>of</strong> TQM/CQI <strong>in</strong> the <strong>Healthcare</strong> Industry",Benchmark<strong>in</strong>g for Quality Management & Technology, vol. 3, no.2, pp. 31-50.Carver, A., (1985). Quality Assurance <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>. Puerto Rico:International Hospital Congress.815
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future ChallengesCentral Department <strong>of</strong> Statistics, (2010). Census Book for <strong>Saudi</strong> <strong>Arabia</strong>.Riyadh: M<strong>in</strong>istry <strong>of</strong> Economy and Plann<strong>in</strong>g.Dixon, N., (1982). "Quality Assurance <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>n Hospitals." <strong>Saudi</strong>Medical <strong>Journal</strong>, vol. 5, no. 1, pp.47-53.Geyndt, W. D., (1995). Manag<strong>in</strong>g the Quality <strong>of</strong> Health <strong>in</strong> Develop<strong>in</strong>gCountries. Wash<strong>in</strong>gton D. C: The World Bank.Jannadi, B., et al., (2008). "Current Structures and Future Challenges forthe <strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>." Asia Pacific <strong>Journal</strong> <strong>of</strong>Health Management, vol. 3, no. 1, pp. 43-50.Jarallah, J. and Khoja, T., (1998). "Perception <strong>of</strong> Supervisors <strong>of</strong> TheirRole <strong>in</strong> Primary <strong>Healthcare</strong> Programmes <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>", EasternMediterranean Health <strong>Journal</strong>, vol. 4, no. 3.Khoja, T. and Saleem, A., (2001). Primary <strong>Healthcare</strong>: History,Achievements and Future. Riyadh: M<strong>in</strong>istry <strong>of</strong> Health Press.Looney, R., (1982). <strong>Saudi</strong> <strong>Arabia</strong>'s Development Potential. Toronto:Lex<strong>in</strong>gton Books.Luce, J. M., B<strong>in</strong>dman, B., and Lee, R., (1994). "A Brief History <strong>of</strong><strong>Healthcare</strong> Quality Assessment and Improvement <strong>in</strong> the UnitedStates." The Western <strong>Journal</strong> <strong>of</strong> Medic<strong>in</strong>e, vol. 160, no. 3.M<strong>in</strong>istry <strong>of</strong> Economy and Plann<strong>in</strong>g, (2003). Human Development Report:<strong>Saudi</strong> <strong>Arabia</strong>. Riyadh: M<strong>in</strong>istry <strong>of</strong> Economy and Plann<strong>in</strong>g Press.M<strong>in</strong>istry <strong>of</strong> Health, (2006). Health Statistical Year Book. Riyadh: M<strong>in</strong>istry<strong>of</strong> Health Press.M<strong>in</strong>istry <strong>of</strong> Health, (2008). Health Statistical Year Book. Riyadh: M<strong>in</strong>istry<strong>of</strong> Health Press.Mufti, Mohammed Hassan, S., (2000). <strong>Healthcare</strong> Development Strategies<strong>in</strong> the K<strong>in</strong>gdom <strong>of</strong> <strong>Saudi</strong> <strong>Arabia</strong>. New York: Spr<strong>in</strong>ger.Naiaz, A. H, (2005). Quality <strong>of</strong> Health Care: Theory and Practice.816
Fahd Mohammed Albejaidi, University <strong>of</strong> New England (Australia)Riyadh: M<strong>in</strong>istry <strong>of</strong> Health Press.Naiaz, A. H, (2006). "The implementation <strong>of</strong> Quality Programme <strong>in</strong>General Directorates <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>", Quality <strong>Journal</strong>, vol. 1, p. 11.Pelletier, Luc R. and Beaud<strong>in</strong>, Christy L., (2005). Q Solutions: EssentialResources for the <strong>Healthcare</strong> Quality Pr<strong>of</strong>essional. Glenview, IL:National Association for <strong>Healthcare</strong> QualitySafran, N., (1988). <strong>Saudi</strong> <strong>Arabia</strong>: The Ceaseless Quest for Security. NewYork: Cornell University Press.Schieber, G., (2001). “Vision 2020 Health Sector Report”, <strong>in</strong> M<strong>in</strong>istry <strong>of</strong>Economy and Plann<strong>in</strong>g’s Future Vision for the <strong>Saudi</strong> Economy. Riyadh:M<strong>in</strong>istry <strong>of</strong> Economy and Plann<strong>in</strong>g Press.Sebai, Z., Milaat, W., and Al- Zulaiabani, A., (2001). "Health CareServices <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: Past, Present and Future" <strong>Saudi</strong> Society <strong>of</strong>Family and Community Medic<strong>in</strong>e, vol. 8, no. 3, pp. 93-101.Skillicorn, S., (1987). "Quality Assurance: Mirage or Mirror?" Annals <strong>of</strong><strong>Saudi</strong> Medic<strong>in</strong>e, vol. 7, no. 2, pp. 89-92.Soltis, M., (1986). "Summary <strong>of</strong> a Quality Assurance Program <strong>in</strong> <strong>Saudi</strong><strong>Arabia</strong>." QRB, vol. 12, no. 7, p. 266.Walston Stephen, Al-Harbi Yousef and Al-Omar Badran, (2008). "TheChang<strong>in</strong>g Face <strong>of</strong> <strong>Healthcare</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>", Ann <strong>Saudi</strong> Med., no. 28,pp. 243-250.Watk<strong>in</strong>s, K., (2005). “Human Development Report 2005”, <strong>in</strong> UnitedNations, International Cooperation at a Crossroads: Aid, Trade andSecurity <strong>in</strong> an Unequal World. New York: United Nations.World Health Organisation (WHO), (2000). Health <strong>System</strong>s: Improv<strong>in</strong>gHealth. Geneva: World Health Organisation.World Health Organisation (WHO), (2004). The Work <strong>of</strong> WHO <strong>in</strong> theEastern Mediterranean Region: Annual Report <strong>of</strong> the Regional Director 1January—31 December, 2003. Cairo: World Health Organisation,Regional Office for the Eastern Mediterranean.817
<strong>Healthcare</strong> <strong>System</strong> <strong>in</strong> <strong>Saudi</strong> <strong>Arabia</strong>: An Analysis <strong>of</strong> Structure, Total Quality Managementand Future ChallengesWorld Health Organisation (WHO), (2006). Country CooperationStrategy for <strong>Saudi</strong> <strong>Arabia</strong>, 2006-2011. Cairo: World Health Organisation,Regional Office for the Eastern Mediterranean.818